You might also like
- Nihms 260877 PDFDocument23 pagesNihms 260877 PDFfebyan yohanesNo ratings yet
- Antidiabetes Untuk Pasien CKDDocument6 pagesAntidiabetes Untuk Pasien CKDRosalina AmbarNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFAlejandro Guerrero LeónNo ratings yet
- SX Nefrotico 2014Document10 pagesSX Nefrotico 2014Nancy MoranchelNo ratings yet
- Prevention of The ComplicationsDocument19 pagesPrevention of The ComplicationsChan ChanNo ratings yet
- MEHU130 - U2 - T43 - Nefropatia DiabeticaDocument110 pagesMEHU130 - U2 - T43 - Nefropatia DiabeticaStefani AtlleNo ratings yet
- Neuropatia DiabéticaDocument18 pagesNeuropatia DiabéticaGustavo PestanaNo ratings yet
- Nefropatia DiabeticaDocument13 pagesNefropatia DiabeticagerardoNo ratings yet
- Hipertensi Dalam Retinopati DMDocument6 pagesHipertensi Dalam Retinopati DMivanaNo ratings yet
- Microvascular and Macrovascular Complications of Diabetes: Editor's Note: This Article Is The 6th in ADocument6 pagesMicrovascular and Macrovascular Complications of Diabetes: Editor's Note: This Article Is The 6th in AnadyaNo ratings yet
- Cleveland Clinic Journal of Medicine-2013-Appel-209-17 Nefropatia DiabeticaDocument9 pagesCleveland Clinic Journal of Medicine-2013-Appel-209-17 Nefropatia DiabeticaMary DiazNo ratings yet
- Diabeticneuropathypart1: Overview and Symmetric PhenotypesDocument21 pagesDiabeticneuropathypart1: Overview and Symmetric PhenotypesPrima Heptayana NainggolanNo ratings yet
- Drugs To Use in CKDDocument8 pagesDrugs To Use in CKDMANOJTHUTHIJANo ratings yet
- Up-Date On Diabetic NephropathyDocument17 pagesUp-Date On Diabetic NephropathykvyNo ratings yet
- Chronic Complications of Diabetes MellitusDocument35 pagesChronic Complications of Diabetes MellitusironNo ratings yet
- 331 FullDocument15 pages331 FullsaravabioNo ratings yet
- Diabetic Vascular Diseases: Molecular Mechanisms and Therapeutic StrategiesDocument29 pagesDiabetic Vascular Diseases: Molecular Mechanisms and Therapeutic StrategiesBBD BBDNo ratings yet
- CrimesDocument6 pagesCrimesShirmayne TangNo ratings yet
- Jrip 2 73Document8 pagesJrip 2 73devyNo ratings yet
- Approaches To Peripheral Artery Disease in DiabetesDocument18 pagesApproaches To Peripheral Artery Disease in DiabetesNabita AuliaNo ratings yet
- 20200800.0-00029 Preoperative GlucosaDocument9 pages20200800.0-00029 Preoperative GlucosaLuis OrdóñezNo ratings yet
- Копия Towards prevention of diabetic peripheral neuropathy clinical presentation, pathogenesis, and new treatmentsDocument15 pagesКопия Towards prevention of diabetic peripheral neuropathy clinical presentation, pathogenesis, and new treatmentsn01zelolNo ratings yet
- PIIS2468024919314652Document4 pagesPIIS2468024919314652adri20121989No ratings yet
- Diabetic NeuropathyDocument10 pagesDiabetic Neuropathyrafael rocha novaesNo ratings yet
- Porrini 2015Document10 pagesPorrini 2015aparajitaNo ratings yet
- 28sici 291096 9136 28199802 2915 3A2 3C97 3A 3aaid Dia523 3e3.0.co 3B2 5 PDFDocument16 pages28sici 291096 9136 28199802 2915 3A2 3C97 3A 3aaid Dia523 3e3.0.co 3B2 5 PDFHesbon MomanyiNo ratings yet
- EMReports HyperkalemiaDocument14 pagesEMReports HyperkalemiaLuis Miguel VillanuevaNo ratings yet
- Wa0011.Document180 pagesWa0011.Mohamed AbdelmoniemNo ratings yet
- Drug Therapy Prevention and Treatment DiabetesDocument8 pagesDrug Therapy Prevention and Treatment DiabetesBaba diawNo ratings yet
- Les 2Document8 pagesLes 2Soemi BautistaNo ratings yet
- Complicaciones Diabetes 1Document16 pagesComplicaciones Diabetes 1danielentuxtlaNo ratings yet
- Complic DM 1Document16 pagesComplic DM 1Bárbara RiffoNo ratings yet
- 08 Tarr Et Al 2012Document13 pages08 Tarr Et Al 2012abbhyasa5206No ratings yet
- Arnold Et Al 2016 Neurological Complications in Chronic Kidney DiseaseDocument13 pagesArnold Et Al 2016 Neurological Complications in Chronic Kidney DiseaseM. Putra Ardhimas KesumaNo ratings yet
- Articulo de Retinopatia DiabeticaDocument4 pagesArticulo de Retinopatia DiabeticaJohana DíazNo ratings yet
- Diabetes Melitus Jurnal Remed BiomedDocument6 pagesDiabetes Melitus Jurnal Remed BiomedNur Roza Aulia RNo ratings yet
- Glomerulopatías PrimariasDocument8 pagesGlomerulopatías PrimariasGSENo ratings yet
- Tes Faye 2009Document3 pagesTes Faye 2009ardyariniNo ratings yet
- Management of Patients With Nephrotic Syndrome: Sophie de Seigneux, Pierre-Yves MartinDocument7 pagesManagement of Patients With Nephrotic Syndrome: Sophie de Seigneux, Pierre-Yves MartinGarit Hapsari KiranaNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument6 pagesDiabetes & Metabolic Syndrome: Clinical Research & ReviewsRizki NovNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument6 pagesDiabetes & Metabolic Syndrome: Clinical Research & ReviewsRizki NovNo ratings yet
- Thomas2015 PDFDocument20 pagesThomas2015 PDFleandroNo ratings yet
- Diabetes ComplicationsDocument7 pagesDiabetes ComplicationstalaNo ratings yet
- 77 FullDocument6 pages77 FullRizkaNNatsirNo ratings yet
- Role of Oxidative Stress On Chronic Kidney Disease ProgressionDocument9 pagesRole of Oxidative Stress On Chronic Kidney Disease ProgressionMohammad WahyuNo ratings yet
- Ec 21 0097Document9 pagesEc 21 0097Irvin MarcelNo ratings yet
- Continuous Ambulatory Peritoneal Dialysis in Diabetic PatientsDocument6 pagesContinuous Ambulatory Peritoneal Dialysis in Diabetic PatientsAjeng SuparwiNo ratings yet
- Asssociation of Glycaemia With Macrovascular and Microvascular ComplicationsDocument8 pagesAsssociation of Glycaemia With Macrovascular and Microvascular ComplicationsMartha CoradoNo ratings yet
- NRDP 201518Document20 pagesNRDP 201518ENRIQUE ZAMORA RODRIGUEZNo ratings yet
- Nefropati Pada Pasien Diabetes Mellitus: Toga A. Simatupang, Sumanto WijayaDocument8 pagesNefropati Pada Pasien Diabetes Mellitus: Toga A. Simatupang, Sumanto WijayakressaNo ratings yet
- Ni Hms 933167Document30 pagesNi Hms 933167sung rae rimNo ratings yet
- Outpatientassessmentand Managementofthediabeticfoot: John A. DipretaDocument21 pagesOutpatientassessmentand Managementofthediabeticfoot: John A. DipretaAnonymous kdBDppigENo ratings yet
- Hyperuricemia and Gout in CKDDocument28 pagesHyperuricemia and Gout in CKDDEPO TOWERNo ratings yet
- Chronic DM ComplicationsDocument24 pagesChronic DM ComplicationsHillary RabinNo ratings yet
- Atm 08 13 825Document9 pagesAtm 08 13 825Titan LinggastiwiNo ratings yet
- Cardiac Autonomic Neuropathy in Diabetes: A Clinical PerspectiveDocument8 pagesCardiac Autonomic Neuropathy in Diabetes: A Clinical PerspectiveHandriee Oka DiputeraNo ratings yet
- Manejo Perioperativo Del Páciente Diabético en La Cirugía OrtopédicaDocument10 pagesManejo Perioperativo Del Páciente Diabético en La Cirugía OrtopédicaVicente David Treviño NavarroNo ratings yet
- ##Default - Genres.article## 28348 2 10 20210116Document14 pages##Default - Genres.article## 28348 2 10 20210116Vega VirlyNo ratings yet
- Nephrotic Syndrome in Adults: Acute Medicine 2018 17 (1) : 36-43 36Document8 pagesNephrotic Syndrome in Adults: Acute Medicine 2018 17 (1) : 36-43 36Deddy TriwijayaNo ratings yet
- Emergencies in Diabetes: Diagnosis, Management and PreventionFrom EverandEmergencies in Diabetes: Diagnosis, Management and PreventionNo ratings yet
- Insulin AspartDocument2 pagesInsulin AspartPatricia MaglasangNo ratings yet
- PHARMACEUTICAL CHEMISTRY - AntihistaminesDocument283 pagesPHARMACEUTICAL CHEMISTRY - AntihistaminesGianniNo ratings yet
- Chapter 47 Diabetes Mellitus PDFDocument14 pagesChapter 47 Diabetes Mellitus PDFRLLT100% (1)
- 8.5 Biotechnology ApplicationsDocument3 pages8.5 Biotechnology ApplicationsNarasimha MurthyNo ratings yet
- Physioex Lab Report: Pre-Lab Quiz ResultsDocument4 pagesPhysioex Lab Report: Pre-Lab Quiz ResultsAnggina SiregarNo ratings yet
- Protein Therapeutics - Summary and Pharmacological Classification PDFDocument19 pagesProtein Therapeutics - Summary and Pharmacological Classification PDFTigno AhmadNo ratings yet
- SCIENCE TECHNOLOGY SOCIETY Quiz 1 6 1Document35 pagesSCIENCE TECHNOLOGY SOCIETY Quiz 1 6 1User Name100% (8)
- EAT-FAT GET-FIT Essentials: Low Carb Wellness Made Easy - Learn To Thrive Rather Than Merely Survive in Less Than 60 MinutesDocument50 pagesEAT-FAT GET-FIT Essentials: Low Carb Wellness Made Easy - Learn To Thrive Rather Than Merely Survive in Less Than 60 MinutesTed Neckowicz100% (1)
- Antidiabetic Drugs: DR Naser Ashraf Tadvi Associate Professor, Pharmacology Ayaan Institute of Medical SciencesDocument63 pagesAntidiabetic Drugs: DR Naser Ashraf Tadvi Associate Professor, Pharmacology Ayaan Institute of Medical SciencesMelati SatriasNo ratings yet
- NovoRapid (Insulin Aspart) PDFDocument113 pagesNovoRapid (Insulin Aspart) PDFAchmad SuryadiNo ratings yet
- Diabetes Mellitus Resource UnitDocument21 pagesDiabetes Mellitus Resource UnitPmoigki100% (1)
- Fructose-1,6-Bisphosphatase Inhibitors A Review 2017Document33 pagesFructose-1,6-Bisphosphatase Inhibitors A Review 2017alejandra vazquez vazquezNo ratings yet
- Diabetes and HerbsDocument132 pagesDiabetes and HerbsAjmal KhanNo ratings yet
- DiabetiesDocument11 pagesDiabetiesAnil ChityalNo ratings yet
- Insulin Resistance PDFDocument275 pagesInsulin Resistance PDFuzzal ahmedNo ratings yet
- 2019 Nuclear Medicine in Oncology PDFDocument346 pages2019 Nuclear Medicine in Oncology PDFLiliana Patricia Torres Agredo100% (1)
- 5 Idiopathic Diseases: Arranged By: Aryana Budiawan Septian Hidayat Zaki Fahrul AziDocument14 pages5 Idiopathic Diseases: Arranged By: Aryana Budiawan Septian Hidayat Zaki Fahrul AziZaki Azki TigabelasNo ratings yet
- Intro To MED-SurgDocument47 pagesIntro To MED-SurgMarites Santos AquinoNo ratings yet
- AP Bio - Chapter 40 OutlineDocument8 pagesAP Bio - Chapter 40 OutlineEllen LiNo ratings yet
- Unseen PassageDocument7 pagesUnseen PassageChanya SardanaNo ratings yet
- Insulin Drug StudyDocument2 pagesInsulin Drug StudyRai Hanah92% (13)
- Material On PHYSIOLOGICAL CHANGES DURING PREGNANCYDocument21 pagesMaterial On PHYSIOLOGICAL CHANGES DURING PREGNANCYAnuradha MauryaNo ratings yet
- Diabetes Types: Aseel Saleh Al-OmariDocument11 pagesDiabetes Types: Aseel Saleh Al-OmariHasan AlomariNo ratings yet
- The Road To Free Insulin: Guyana Case StudyDocument5 pagesThe Road To Free Insulin: Guyana Case StudyarmanNo ratings yet
- Recombinant Dna: Quarter 3 / Week 1Document16 pagesRecombinant Dna: Quarter 3 / Week 1Sherry Macalalad GarciaNo ratings yet
- Sugar Control and Diabetes Exam-Style Questions (+ Mark Scheme)Document14 pagesSugar Control and Diabetes Exam-Style Questions (+ Mark Scheme)Emaan MaryamNo ratings yet
- Medifocus April 2007Document61 pagesMedifocus April 2007Pushpanjali Crosslay HospitalNo ratings yet
- Bwcs Feedback Final September 2023Document56 pagesBwcs Feedback Final September 2023Babloo50% (2)
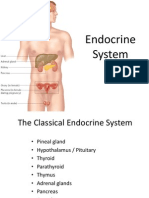
- Endocrine SystemDocument96 pagesEndocrine SystemSandhya Kakkar100% (3)
- Iridology and HypoglycemiaDocument15 pagesIridology and Hypoglycemiasohail_mashwnaiNo ratings yet