You might also like
- Pediatric Immunology: A Case-Based Collection with MCQs, Volume 2From EverandPediatric Immunology: A Case-Based Collection with MCQs, Volume 2No ratings yet
- Neuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesFrom EverandNeuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesAmanda L. PiquetNo ratings yet
- Seminar: Enno Schmidt, Detlef ZillikensDocument13 pagesSeminar: Enno Schmidt, Detlef ZillikensUssiy RachmanNo ratings yet
- Pemphigus: by Demetris Ioannides, MD Associate Professor of DermatologyDocument43 pagesPemphigus: by Demetris Ioannides, MD Associate Professor of DermatologyYulita PurbaNo ratings yet
- Eosinofilia en Trastornos Reumatologicos VascularesDocument24 pagesEosinofilia en Trastornos Reumatologicos VascularesSaidNo ratings yet
- Aplastic AnemiaDocument26 pagesAplastic AnemiaIrina Moldovan100% (1)
- Jcad 6 8 23Document6 pagesJcad 6 8 23Hadi FirmansyahNo ratings yet
- Blood and Bone Marrow Evaluation For Eosinophilia: Daniel F. Boyer, MD, PHDDocument8 pagesBlood and Bone Marrow Evaluation For Eosinophilia: Daniel F. Boyer, MD, PHDlubna aloshibiNo ratings yet
- Anti-Glomerular Basement Membrane DiseaseDocument11 pagesAnti-Glomerular Basement Membrane DiseaseCARZ 42No ratings yet
- Chapter 53:: Paraneoplastic Pemphigus:: Grant J. Anhalt & Daniel MimouniDocument15 pagesChapter 53:: Paraneoplastic Pemphigus:: Grant J. Anhalt & Daniel MimouniFiraNo ratings yet
- CANINE-Pemphigus Complex-Pathogenesis and Clinical PresentationDocument5 pagesCANINE-Pemphigus Complex-Pathogenesis and Clinical Presentationtaner_soysuren100% (4)
- Pulmonary LymphangiomatosisDocument4 pagesPulmonary LymphangiomatosisAlina SarbuNo ratings yet
- Eosinophilia in Rheumatologic Vascular Disorders CNADocument24 pagesEosinophilia in Rheumatologic Vascular Disorders CNAReyner LeonNo ratings yet
- StudyDocument10 pagesStudyemranalshaibaniNo ratings yet
- Lupus 1Document9 pagesLupus 1karina hernandezNo ratings yet
- Aplastic Anemia: Etiology, Molecular Pathogenesis and Emerging ConceptsDocument17 pagesAplastic Anemia: Etiology, Molecular Pathogenesis and Emerging Conceptshabibe koçNo ratings yet
- 2023 38 2 163 173 EngDocument11 pages2023 38 2 163 173 EngHashem Essa QatawnehNo ratings yet
- EMPD Review (Shabihkhani) 2020 Appl Immunohistochem Mol MorphDocument14 pagesEMPD Review (Shabihkhani) 2020 Appl Immunohistochem Mol MorphCarloNo ratings yet
- Aplastic Anemia: Review of Etiology and TreatmentDocument7 pagesAplastic Anemia: Review of Etiology and TreatmentCleber MaiaNo ratings yet
- Direct Immmuno Flourescence Study in Auto Immune Bullous DisordersDocument3 pagesDirect Immmuno Flourescence Study in Auto Immune Bullous DisordersInternational Organization of Scientific Research (IOSR)No ratings yet
- Pemphigus vulgarisPPTDocument23 pagesPemphigus vulgarisPPTSiti HanisaNo ratings yet
- Systemic AL Amyloidosis Current Approaches To DiagDocument12 pagesSystemic AL Amyloidosis Current Approaches To DiagAnia WagnerNo ratings yet
- Patogenesis IMNDocument23 pagesPatogenesis IMNshiloinNo ratings yet
- Sickle Cell AnemiaDocument5 pagesSickle Cell Anemiaكل يوم فيديو ممتعNo ratings yet
- Bullous PemphigoidDocument5 pagesBullous PemphigoidHidayah MustaphaNo ratings yet
- Pemphigus Vulgaris: Ontinuing Edical DucationDocument15 pagesPemphigus Vulgaris: Ontinuing Edical Ducationcut winda agustiaNo ratings yet
- مناعة كاملةDocument135 pagesمناعة كاملةمحمد اللاميNo ratings yet
- Hematology 2006 Young 72 7Document6 pagesHematology 2006 Young 72 7Indira DeviNo ratings yet
- 2317 FullDocument14 pages2317 FulltorajasaNo ratings yet
- Immunopathogenesis of Pemphigus Vulgaris: A Brief ReviewDocument3 pagesImmunopathogenesis of Pemphigus Vulgaris: A Brief ReviewAnonymous SPrI0gbTr0No ratings yet
- Lupus Full PDFDocument12 pagesLupus Full PDFEzza noerNo ratings yet
- Aplastic AnemiaDocument5 pagesAplastic Anemiascremo_xtremeNo ratings yet
- Aetiology, Diagnosis and Treatment of Hydrops FoetalisDocument10 pagesAetiology, Diagnosis and Treatment of Hydrops FoetalisMargareta OktavianiNo ratings yet
- EsclerodermiaDocument15 pagesEsclerodermiaIvette Andrea HQNo ratings yet
- Abc 103 02 0165Document5 pagesAbc 103 02 0165Sumeet TripathiNo ratings yet
- Ocular Manifestations in Systemic Lupus Erythematosus: Sukhum Silpa-Archa, Joan J Lee, C Stephen FosterDocument8 pagesOcular Manifestations in Systemic Lupus Erythematosus: Sukhum Silpa-Archa, Joan J Lee, C Stephen FosterNadya Regina PermataNo ratings yet
- Anesthesia For Systemic Lupus Erythematosus ReviewDocument12 pagesAnesthesia For Systemic Lupus Erythematosus ReviewAnonymous x75qV3lGNo ratings yet
- Arpa - 2018 0219 RaDocument6 pagesArpa - 2018 0219 Rahuseikha velayazulfahdNo ratings yet
- 2017-July-Fanconi AnemiaDocument3 pages2017-July-Fanconi AnemiaHumaida Hasan SamiraNo ratings yet
- Hemoptysis in A Healthy 13-Year-Old Boy: PresentationDocument5 pagesHemoptysis in A Healthy 13-Year-Old Boy: PresentationluishelNo ratings yet
- Cerebral Malaria Immunopathology PDFDocument11 pagesCerebral Malaria Immunopathology PDFAurelia WetondieNo ratings yet
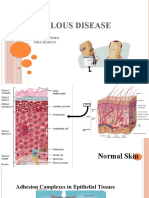
- Bullous Disease: Farah Alsheikh Dima ArabiyatDocument58 pagesBullous Disease: Farah Alsheikh Dima ArabiyatAhmad AltarefeNo ratings yet
- Systemic Lupus Erythematosus: Authors: DR Jessica J Manson and DR Anisur RahmanDocument0 pagesSystemic Lupus Erythematosus: Authors: DR Jessica J Manson and DR Anisur RahmanRizka Norma WiwekaNo ratings yet
- Stroke in Systemic Lupus Erythematosus and Antiphospholipid Syndrome: Risk Factors, Clinical Manifestations, Neuroimaging, and TreatmentDocument9 pagesStroke in Systemic Lupus Erythematosus and Antiphospholipid Syndrome: Risk Factors, Clinical Manifestations, Neuroimaging, and TreatmentKarl Martin PinedaNo ratings yet
- Review: K. Osterbur, F.A. Mann, K. Kuroki, and A. DeclueDocument11 pagesReview: K. Osterbur, F.A. Mann, K. Kuroki, and A. DeclueMill Jan CruzNo ratings yet
- SplnectomyDocument3 pagesSplnectomydheeraj vermaNo ratings yet
- 1 s2.0 S0749070421001019 MainDocument17 pages1 s2.0 S0749070421001019 MainEliseu AmaralNo ratings yet
- Bone Marrow Hypoplasia 2022Document34 pagesBone Marrow Hypoplasia 2022Jose Angel Cobian GaliciaNo ratings yet
- Diagnosisandclinical Featuresofpemphigus Vulgaris: Supriya S. Venugopal,, Dédée F. MurrellDocument1 pageDiagnosisandclinical Featuresofpemphigus Vulgaris: Supriya S. Venugopal,, Dédée F. MurrellDwiKamaswariNo ratings yet
- Saaf Avances Diagnostico y Manejo 2023Document20 pagesSaaf Avances Diagnostico y Manejo 2023Cristian RiveraNo ratings yet
- Treatment For Aplastic AnemiaDocument13 pagesTreatment For Aplastic Anemiagustianto hutama pNo ratings yet
- Bone Marrow Hypoplasia 2023Document34 pagesBone Marrow Hypoplasia 2023Dafne LunaNo ratings yet
- Infection-Genetics Relationship in Systemic Lupus ErythematosusDocument8 pagesInfection-Genetics Relationship in Systemic Lupus ErythematosusegonzalesrnNo ratings yet
- Lupus Research PaperDocument5 pagesLupus Research Paperttdqgsbnd100% (3)
- Atopy in NSDocument13 pagesAtopy in NSshiloinNo ratings yet
- Personal Practice: Subacute Sclerosing PanencephalitisDocument8 pagesPersonal Practice: Subacute Sclerosing PanencephalitisdrjghosalNo ratings yet
- Antiphosphilipid SyndromeDocument17 pagesAntiphosphilipid SyndromeEliDavidNo ratings yet
- Anemia Hemolítica CalienteDocument8 pagesAnemia Hemolítica CalienteJesús Evangelista GomerNo ratings yet
- Neuromyelitisoptica: Sarah L. Patterson,, Sarah E. GoglinDocument13 pagesNeuromyelitisoptica: Sarah L. Patterson,, Sarah E. GoglinErji K.No ratings yet
- Heart Valve Disease: State of the ArtFrom EverandHeart Valve Disease: State of the ArtJose ZamoranoNo ratings yet
- A Clinician's Guide To Topical Retinoids: Melika Motamedi, Ahmad Chehade, Ravina Sanghera, and Parbeer GrewalDocument8 pagesA Clinician's Guide To Topical Retinoids: Melika Motamedi, Ahmad Chehade, Ravina Sanghera, and Parbeer Grewalzendah123No ratings yet
- Outcomes of Severe PARDS On High-Frequency Oscillatory Ventilation - A Single Centre ExperienceDocument7 pagesOutcomes of Severe PARDS On High-Frequency Oscillatory Ventilation - A Single Centre Experiencezendah123No ratings yet
- Jones-Global Trends in Emerging Infectious DiseasesDocument5 pagesJones-Global Trends in Emerging Infectious DiseaseskagameNo ratings yet
- Impact of HFOV in pARDS Outcomes: Questions Remain: Letter Open AccessDocument2 pagesImpact of HFOV in pARDS Outcomes: Questions Remain: Letter Open Accesszendah123No ratings yet
- Parkinson and Parkinsonisme in AdultsDocument6 pagesParkinson and Parkinsonisme in Adultszendah123No ratings yet
- Upload 3Document13 pagesUpload 3zendah123No ratings yet
- Parkinson Disease in BimodalityDocument2 pagesParkinson Disease in Bimodalityzendah123No ratings yet
- Genetics in Parkinson DiseaseDocument23 pagesGenetics in Parkinson Diseasezendah123No ratings yet
- Fluid Management in Parkinson DiseaseDocument13 pagesFluid Management in Parkinson Diseasezendah123No ratings yet
- Mechanical VentilationDocument8 pagesMechanical Ventilationzendah123No ratings yet
- Management in Parkinson DiseaseDocument30 pagesManagement in Parkinson Diseasezendah123No ratings yet
- Norman CousinsDocument3 pagesNorman CousinsXochilt Medina100% (1)
- Blood Transfusion TherapyDocument38 pagesBlood Transfusion TherapyAnn Merlin JobinNo ratings yet
- Diagnostic Exam Funda ReviewDocument13 pagesDiagnostic Exam Funda Reviewmark OrpillaNo ratings yet
- Test Bank For Essentials of Pathophysiology 3rd Edition, PorthDocument23 pagesTest Bank For Essentials of Pathophysiology 3rd Edition, PorthILL110100% (1)
- q1 Elem Ls2 Cano-Candido-JrDocument4 pagesq1 Elem Ls2 Cano-Candido-JrIren Castor MabutinNo ratings yet
- Case 4 Reproductive Block PBLDocument9 pagesCase 4 Reproductive Block PBLFarisNo ratings yet
- Marquis Et Al 2023 CT Approach To Lung InjuryDocument19 pagesMarquis Et Al 2023 CT Approach To Lung InjuryMinh đăng ĐỗNo ratings yet
- Biochemistry of HormonDocument16 pagesBiochemistry of HormonMuhamad SdeqNo ratings yet
- Introduction - MIDocument10 pagesIntroduction - MIkhimiiiNo ratings yet
- Anim Na Sabado NG Beyblade Lesson PlanDocument6 pagesAnim Na Sabado NG Beyblade Lesson PlanJustin BaptistaNo ratings yet
- Cauda EquinaDocument9 pagesCauda EquinaMuhammad Iqbal Farhan RodhiNo ratings yet
- Davao Doctors College Nursing Program Nursing Care PlanDocument7 pagesDavao Doctors College Nursing Program Nursing Care PlanSHININo ratings yet
- DR - Tejashri Thakare M.D (Hom.) : Psora - As Deficiency, Syphilis - As Degeneration & Sycosis - As Over ConstructionDocument23 pagesDR - Tejashri Thakare M.D (Hom.) : Psora - As Deficiency, Syphilis - As Degeneration & Sycosis - As Over ConstructionKani M0zhyNo ratings yet
- Patau Syndrome: Signs and SymptomsDocument3 pagesPatau Syndrome: Signs and SymptomsDaniela BulmagăNo ratings yet
- Mallory Weiss Syndrome - StatPearls - NCBI BookshelfDocument9 pagesMallory Weiss Syndrome - StatPearls - NCBI BookshelfDaniela EstradaNo ratings yet
- Animal Diversity 7Th Edition Hickman Test Bank Full Chapter PDFDocument30 pagesAnimal Diversity 7Th Edition Hickman Test Bank Full Chapter PDFarthur.brown523100% (16)
- Antibiotic Guidelines For Adults 2018 PDFDocument58 pagesAntibiotic Guidelines For Adults 2018 PDFAhmad RizqiNo ratings yet
- 4TH Summative Test in English 10 Final PDFDocument3 pages4TH Summative Test in English 10 Final PDFKenneth Del Rosario100% (3)
- Health Talk On CholelithiasisDocument12 pagesHealth Talk On Cholelithiasisjyoti puniaNo ratings yet
- Intussusception: DR Phillipo Leo ChalyaDocument19 pagesIntussusception: DR Phillipo Leo ChalyaSibabaong'ombe MasakaNo ratings yet
- Excuse LetterDocument1 pageExcuse LetterKyllie Solis AngueNo ratings yet
- Analysis Prediction and Evaluation of CO PDFDocument6 pagesAnalysis Prediction and Evaluation of CO PDFSurfer LeoNo ratings yet
- Basic Science Notes MRCP AssDocument9 pagesBasic Science Notes MRCP AssUm HamoOdNo ratings yet
- CV By, Yvette02Document4 pagesCV By, Yvette02Yvette PamatmatNo ratings yet
- DiphtheriaDocument36 pagesDiphtheriaDr. SAMNo ratings yet
- Nursing Care Plan Assessment Diagnosis Inference Planning Intervention Rationale Evaluation Subjective: Short Term: Independent: Goal MetDocument4 pagesNursing Care Plan Assessment Diagnosis Inference Planning Intervention Rationale Evaluation Subjective: Short Term: Independent: Goal MetKiana OcampoNo ratings yet
- The Severe and Persistent Mental Illness Treatment Planner Practiceplanners Ebook PDF VersionDocument58 pagesThe Severe and Persistent Mental Illness Treatment Planner Practiceplanners Ebook PDF Versionpaul.trivino34896% (27)
- Syndromes and Periodontal Disease-An Insight!: Dr. Grishmi NiswadeDocument6 pagesSyndromes and Periodontal Disease-An Insight!: Dr. Grishmi NiswadeTJPRC PublicationsNo ratings yet
- Pulmonary Tuberculosis 2017Document13 pagesPulmonary Tuberculosis 2017GioNo ratings yet
- الاضطرابات النمائية الشاملةDocument26 pagesالاضطرابات النمائية الشاملةmohamedboumerdassi.2209No ratings yet