You might also like
- Adult Recon. Hip Knee AAOs2019 PDFDocument60 pagesAdult Recon. Hip Knee AAOs2019 PDFadnanNo ratings yet
- QBANK PasTest SAQs For DentistryDocument651 pagesQBANK PasTest SAQs For DentistrybassamNo ratings yet
- Drape Mayo TableDocument12 pagesDrape Mayo TableMark Arryson Casison100% (1)
- Traumatic Iatrogenic Complications Associated With Orthodontic Treatments: A Systematic ReviewDocument7 pagesTraumatic Iatrogenic Complications Associated With Orthodontic Treatments: A Systematic Reviewsunk86No ratings yet
- Arthroplasty Today: Case ReportDocument5 pagesArthroplasty Today: Case ReportCristina SavaNo ratings yet
- The Management of Bilateral Posterior Fracture Dislocations of The Shoulder: A Case Series Illustrating Management OptionsDocument7 pagesThe Management of Bilateral Posterior Fracture Dislocations of The Shoulder: A Case Series Illustrating Management OptionsGustavo BECERRA PERDOMONo ratings yet
- Joints OITE - 2012 2013 2014Document231 pagesJoints OITE - 2012 2013 2014SenthilNo ratings yet
- AAOS2001 ReconstructionDocument58 pagesAAOS2001 ReconstructionHéctor Pando SánchezNo ratings yet
- Anatomy of Pilon Fractures of The Distal Tibia: TraumaDocument6 pagesAnatomy of Pilon Fractures of The Distal Tibia: TraumaaiakobyNo ratings yet
- Protrusio Acetabuli PDFDocument10 pagesProtrusio Acetabuli PDFSoemantri DoankNo ratings yet
- Spinous Process Fractures in Osteoporotic Thoracolumbar Vertebral FracturesDocument4 pagesSpinous Process Fractures in Osteoporotic Thoracolumbar Vertebral FracturesAditya Arya PutraNo ratings yet
- Anatomic Posterolateral Corner ReconstructionDocument10 pagesAnatomic Posterolateral Corner Reconstructionethan.dumontNo ratings yet
- "A To P" Screw Versus Posterolateral Plate For PosteriorDocument6 pages"A To P" Screw Versus Posterolateral Plate For PosteriorErlin EsauNo ratings yet
- Metallosis and Cobalt e Chrome Intoxication After Hip ResurfacingDocument6 pagesMetallosis and Cobalt e Chrome Intoxication After Hip ResurfacingKaty Marlen GongoraNo ratings yet
- Angiographic Evaluation of Arterial Configuration After Acute Shortening 2013Document9 pagesAngiographic Evaluation of Arterial Configuration After Acute Shortening 2013aymanNo ratings yet
- Floating ElbowDocument5 pagesFloating ElbowpepitomuraNo ratings yet
- Morbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesDocument8 pagesMorbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesAthenaeum Scientific PublishersNo ratings yet
- Tang 2010Document5 pagesTang 2010Elena ShekaNo ratings yet
- Variability in Olecranon Ao Fracture Fixation: A Radiological StudyDocument6 pagesVariability in Olecranon Ao Fracture Fixation: A Radiological StudyFhietry Idrus ScaftweeNo ratings yet
- What Is The Single Most Important Technical AspectDocument6 pagesWhat Is The Single Most Important Technical AspecttripodegrandeNo ratings yet
- 1752 1947 6 171Document6 pages1752 1947 6 171Baharudin Yusuf RamadhaniNo ratings yet
- 3 Columnas Acetabulares ClasificaiconDocument11 pages3 Columnas Acetabulares Clasificaiconlriveros540No ratings yet
- Adult Reconstructive Surgery of The Hip and Knee Scored and Recorded Self-Assessment ExaminationDocument66 pagesAdult Reconstructive Surgery of The Hip and Knee Scored and Recorded Self-Assessment ExaminationZia Ur RehmanNo ratings yet
- Catastrophic Talar Bone Loss From High Velocity Trauma Treated With Structural Tricorticate Fibula Autograft Compression Frame and Midfoot Distraction ArthroplastyDocument9 pagesCatastrophic Talar Bone Loss From High Velocity Trauma Treated With Structural Tricorticate Fibula Autograft Compression Frame and Midfoot Distraction ArthroplastyAthenaeum Scientific PublishersNo ratings yet
- Assessment of The Anterior Talofibular Ligament Thickness 2017 Journal of MeDocument5 pagesAssessment of The Anterior Talofibular Ligament Thickness 2017 Journal of MeRyana Fitriana IINo ratings yet
- BackgroundDocument5 pagesBackgroundMaricar K. BrionesNo ratings yet
- Painful Knee 2024 International Journal of Surgery Case ReportsDocument6 pagesPainful Knee 2024 International Journal of Surgery Case ReportsRonald QuezadaNo ratings yet
- 13 19 Anatomy Pathophysiology and Classification of Posterior Tibial Tendon DysfunctionDocument7 pages13 19 Anatomy Pathophysiology and Classification of Posterior Tibial Tendon Dysfunctiongismaputri santosoNo ratings yet
- Miyamoto 2010 JBJS Current Concepts Review Distal-Biceps-Tendon-Injuries PDFDocument12 pagesMiyamoto 2010 JBJS Current Concepts Review Distal-Biceps-Tendon-Injuries PDFKuozram No MasNo ratings yet
- Ortho ArticleDocument2 pagesOrtho ArticleSamantha Dela Paz100% (1)
- AAOS2003 SpineDocument61 pagesAAOS2003 SpineHizkyas KassayeNo ratings yet
- West Indian Medical Journal: A Case of Pathological Rib Fractures: Focal Osteolysis or Osteoporosis?Document10 pagesWest Indian Medical Journal: A Case of Pathological Rib Fractures: Focal Osteolysis or Osteoporosis?IstianahNo ratings yet
- Articulo OsteonecrosisDocument5 pagesArticulo Osteonecrosisdaniela ramirezNo ratings yet
- Osteoblastoma A Spectrum of Presentation and TreatDocument10 pagesOsteoblastoma A Spectrum of Presentation and TreatmandetoperdiyuwanNo ratings yet
- Ortiz 2016Document23 pagesOrtiz 2016Tomás Urrutia JarpaNo ratings yet
- Effects On Inadvertent Endplate Fracture Following Lateral Cage Placement On Range of Motion and Indirect Spine Decompression in Lumbar Spine Fusion Constructs: A Cadaveric StudyDocument8 pagesEffects On Inadvertent Endplate Fracture Following Lateral Cage Placement On Range of Motion and Indirect Spine Decompression in Lumbar Spine Fusion Constructs: A Cadaveric Studysiti hanifahNo ratings yet
- Thesis Umesh A2z.doc Final Thesis CorrectionDocument79 pagesThesis Umesh A2z.doc Final Thesis CorrectionRakesh JhaNo ratings yet
- Analysis of Contemporary Tools For The Measurement of Enophthalmos: A PRISMA-driven Systematic ReviewDocument9 pagesAnalysis of Contemporary Tools For The Measurement of Enophthalmos: A PRISMA-driven Systematic Reviewstoia_sebiNo ratings yet
- Case Series of All-Arthroscopic Treatment For Terrible Triad of The Elbow: Indications and Clinical OutcomesDocument10 pagesCase Series of All-Arthroscopic Treatment For Terrible Triad of The Elbow: Indications and Clinical OutcomesdorfynatorNo ratings yet
- Nakama 2005Document7 pagesNakama 2005angelica barrazaNo ratings yet
- Morphology of Cranial Sutures and RadiologicDocument6 pagesMorphology of Cranial Sutures and RadiologicEvans RodrigezNo ratings yet
- Acetabulum Fracture Imaging Practice EssentialsDocument35 pagesAcetabulum Fracture Imaging Practice EssentialshaminatrafNo ratings yet
- Total Hip Arthroplasty With Trochanteric Ostectomy For Patients With Angular Deformity of The Proximal FemurDocument8 pagesTotal Hip Arthroplasty With Trochanteric Ostectomy For Patients With Angular Deformity of The Proximal Femurdrbane123No ratings yet
- Brief Resume of Intended WorkDocument7 pagesBrief Resume of Intended WorkNavin ChandarNo ratings yet
- Primary Hyperparathyroidism With Extensive Brown Tumors and Multiple Fractures in A 20-Year-Old WomanDocument6 pagesPrimary Hyperparathyroidism With Extensive Brown Tumors and Multiple Fractures in A 20-Year-Old WomanritvikNo ratings yet
- Anterolateral Ligament Reconstruction Technique An Anatomic BasedDocument5 pagesAnterolateral Ligament Reconstruction Technique An Anatomic BasedEmilio Eduardo ChoqueNo ratings yet
- Europeanjournalof Radiologyopen: Longitudinal Stress Fracture of The Femur: A Rare PresentationDocument4 pagesEuropeanjournalof Radiologyopen: Longitudinal Stress Fracture of The Femur: A Rare PresentationYusfaIndahNo ratings yet
- Erdogmus Et Al 2014 - BonesDocument8 pagesErdogmus Et Al 2014 - Bonesmattlight07No ratings yet
- Anehosur Et Al 2020 Concepts and Challenges in The Surgical Management of Edentulous Mandible Fractures A Case SeriesDocument7 pagesAnehosur Et Al 2020 Concepts and Challenges in The Surgical Management of Edentulous Mandible Fractures A Case SeriesHenry Adhy SantosoNo ratings yet
- Pictorial Essay: Spectrum of MR Imaging Findings in Spinal TuberculosisDocument5 pagesPictorial Essay: Spectrum of MR Imaging Findings in Spinal TuberculosisAnonymous vnv6QFNo ratings yet
- Radiographic Classification of Temporal Bone Fractures: Clinical Predictability Using A New SystemDocument5 pagesRadiographic Classification of Temporal Bone Fractures: Clinical Predictability Using A New SystemTaufik ShidkiNo ratings yet
- Biomechanical RationaleDocument10 pagesBiomechanical RationalekhudecNo ratings yet
- Heel Spur Formation and The Subcalcaneal Enthesis of The Plantar FasciaDocument3 pagesHeel Spur Formation and The Subcalcaneal Enthesis of The Plantar FasciaanurNo ratings yet
- Shape and Volume of Craniofacial Cavities in Intentional Skull DeformationsDocument10 pagesShape and Volume of Craniofacial Cavities in Intentional Skull DeformationsGastón SalasNo ratings yet
- iCVTPFDocument5 pagesiCVTPFErwin Chiquete, MD, PhDNo ratings yet
- Art3a10 10072fs00256-014-1842-5Document9 pagesArt3a10 10072fs00256-014-1842-5api-253958760No ratings yet
- New Symptomatic Compression Fracture After Percutaneous Vertebroplasty at The Thoracolumbar JunctionDocument4 pagesNew Symptomatic Compression Fracture After Percutaneous Vertebroplasty at The Thoracolumbar JunctionRamy ElmasryNo ratings yet
- Cefelometria y ATMDocument7 pagesCefelometria y ATMSharon Tolentino VidalNo ratings yet
- Dystrophic Scoliosis and Rib Resection Case ReportDocument8 pagesDystrophic Scoliosis and Rib Resection Case Reportdadakan16No ratings yet
- Case Report: A Rare Stapes AbnormalityDocument4 pagesCase Report: A Rare Stapes AbnormalityCarolina UrrutiaNo ratings yet
- Labiomandibular Paresthesia Caused by Endodontic Treatment - An Anatomic and Clinical Study PDFDocument13 pagesLabiomandibular Paresthesia Caused by Endodontic Treatment - An Anatomic and Clinical Study PDFAlexandra DumitracheNo ratings yet
- (MRI) Medial Patellar LigamentsDocument11 pages(MRI) Medial Patellar LigamentsyNo ratings yet
- Cartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesFrom EverandCartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesAaron J. KrychNo ratings yet
- NCEZID FRM Pass Attest Eng 508Document5 pagesNCEZID FRM Pass Attest Eng 508fabio andrey afanador quijanoNo ratings yet
- Cement Mantles Grading - BarrackDocument5 pagesCement Mantles Grading - BarrackRoberto GuanipaNo ratings yet
- Transcripción, Traducción (Ósmosis)Document15 pagesTranscripción, Traducción (Ósmosis)Roberto GuanipaNo ratings yet
- Polytrauma Definition Paper - J Trauma 2014Document7 pagesPolytrauma Definition Paper - J Trauma 2014Victor abramonteNo ratings yet
- 10 TipsDocument8 pages10 TipsRoberto GuanipaNo ratings yet
- AO Principles of Fracture Management - 3rd Ed. - Thieme - 2017Document7 pagesAO Principles of Fracture Management - 3rd Ed. - Thieme - 2017Roberto GuanipaNo ratings yet
- VA LCP Two Column Distal Radius Plate 2.4mm PDFDocument44 pagesVA LCP Two Column Distal Radius Plate 2.4mm PDFRoberto GuanipaNo ratings yet
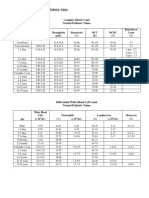
- 30a2131 Complete Blood Count Normal Pediatric Values PDFDocument1 page30a2131 Complete Blood Count Normal Pediatric Values PDFReziel Basilan Manalo100% (2)
- Suplemento Con Proteina Suero, ComplicacionesDocument26 pagesSuplemento Con Proteina Suero, ComplicacionesJosé Luis OjedaNo ratings yet
- Hysterosalpingography A Re - Emerging Study With CDocument7 pagesHysterosalpingography A Re - Emerging Study With CTuyul Yelsi 1No ratings yet
- Harga & Link Ecatalog Dispo-RegDocument2 pagesHarga & Link Ecatalog Dispo-RegPramusita PratyNo ratings yet
- Vto Seminar No.2Document115 pagesVto Seminar No.2Dr Shivam Verma100% (1)
- ACL Reconstruction SurgeryDocument8 pagesACL Reconstruction Surgeryjohn hagisNo ratings yet
- Anexure DDocument9 pagesAnexure DfarhanNo ratings yet
- Seminar 13Document60 pagesSeminar 13radhikamiNo ratings yet
- LTI Junior TermsDocument18 pagesLTI Junior TermsSai VenkatNo ratings yet
- Diastole and AnesthesiaDocument16 pagesDiastole and AnesthesiadrsubramanianNo ratings yet
- Chemical Peeling With Trichloroacetic Acid and Lactic Acid For Infraorbital Dark CirclesDocument6 pagesChemical Peeling With Trichloroacetic Acid and Lactic Acid For Infraorbital Dark CirclesAna Claudia Kordelos DinizNo ratings yet
- Achieve Programmable Automatic Biopsy System: Spring-Loaded Action For Fast, Accurate PenetrationDocument4 pagesAchieve Programmable Automatic Biopsy System: Spring-Loaded Action For Fast, Accurate PenetrationradeonunNo ratings yet
- Internal Fixation Nursing CareDocument5 pagesInternal Fixation Nursing Careeim100% (1)
- Conf ScolioDocument2 pagesConf ScolioMINt KookieNo ratings yet
- Physiotherapy Exercises After Abdominal SurgeryDocument32 pagesPhysiotherapy Exercises After Abdominal SurgeryHUZAIFA YAMAANNo ratings yet
- Method For Assessing Secondary Deformations of The Nose After Heilo UranoplastyDocument10 pagesMethod For Assessing Secondary Deformations of The Nose After Heilo UranoplastyCentral Asian StudiesNo ratings yet
- Humeral Shaft FracturesDocument11 pagesHumeral Shaft FracturesSugey PicoNo ratings yet
- Network List - MAY 2019Document192 pagesNetwork List - MAY 2019p4b5No ratings yet
- Kategori Tindakan OrthopediDocument1 pageKategori Tindakan OrthopediSilas SuryawijayaNo ratings yet
- A Review of Strategies To Decrease The Duration of Indwelling Urethral Catheters and Potentially Reduce The Incidence of Catheter-Associated Urinary Tract Infections - ProQuestDocument10 pagesA Review of Strategies To Decrease The Duration of Indwelling Urethral Catheters and Potentially Reduce The Incidence of Catheter-Associated Urinary Tract Infections - ProQuestHelmy HanafiNo ratings yet
- Handling Instruments Checklist - CABUGATANDocument3 pagesHandling Instruments Checklist - CABUGATANFar Ri NaNo ratings yet
- Vandooren Interdisc 2 LeseprobeDocument33 pagesVandooren Interdisc 2 LeseprobeAlfred OrozcoNo ratings yet
- CGHS RATE AHMEDABAD 2021Document51 pagesCGHS RATE AHMEDABAD 2021Chirag KoradiaNo ratings yet
- Severe Upper Gastrointestinal Bleeding in Extraluminal Diverticula in The Third Part of The Duodenum Michael Wilhelmsen, 1 Johnny FredsboDocument3 pagesSevere Upper Gastrointestinal Bleeding in Extraluminal Diverticula in The Third Part of The Duodenum Michael Wilhelmsen, 1 Johnny FredsboJuan Carlos C SolanoNo ratings yet
- Surgical Options in Oroantral Fistula Management: A Narrative ReviewDocument13 pagesSurgical Options in Oroantral Fistula Management: A Narrative Reviewmehak malhotraNo ratings yet
- Sheet 2 (Local Anesthesia 2)Document14 pagesSheet 2 (Local Anesthesia 2)ardesh abdilleNo ratings yet
- Esophagostomy in BovinesDocument23 pagesEsophagostomy in BovinesWasaq BukhariNo ratings yet
- Neumonia Por Aspiracion BookDocument232 pagesNeumonia Por Aspiracion BookRodrigo Navia ValenzuelaNo ratings yet
- Braddoms 2020 - Capitulo 9 - Protesis EessDocument23 pagesBraddoms 2020 - Capitulo 9 - Protesis EessSergio Navarrete VidalNo ratings yet