You might also like
- The en Cultured Body-BookDocument174 pagesThe en Cultured Body-BooksidorelaNo ratings yet
- Peer Support Within A Health Care Context - A Concept AnalysisDocument12 pagesPeer Support Within A Health Care Context - A Concept AnalysisretnoNo ratings yet
- Ecg Essentials 2 PDFDocument45 pagesEcg Essentials 2 PDFjaikishan marathe 69No ratings yet
- Acute Heart FailureDocument71 pagesAcute Heart FailureVivek Anandan100% (1)
- Flourishing: Health, Disease, and Bioethics in Theological PerspectiveFrom EverandFlourishing: Health, Disease, and Bioethics in Theological PerspectiveNo ratings yet
- Solution Manual For Statistics For Nursing Research A Workbook For Evidence Based Practice 3rd Edition Susan Grove Daisha Cipher Full DownloadDocument3 pagesSolution Manual For Statistics For Nursing Research A Workbook For Evidence Based Practice 3rd Edition Susan Grove Daisha Cipher Full Downloadandreasmithpitornwgbc100% (39)
- Crawford HEALTHISM AND THE MEDICALIZATION OF EVERYDAY LIFEDocument25 pagesCrawford HEALTHISM AND THE MEDICALIZATION OF EVERYDAY LIFElilit sol100% (1)
- Priority in Public Health PDFDocument351 pagesPriority in Public Health PDFKheir Mussa100% (2)
- CHF (Dr. Devi, SP - JP)Document17 pagesCHF (Dr. Devi, SP - JP)sriworoNo ratings yet
- Interactive Code Blue Evaluation FormDocument2 pagesInteractive Code Blue Evaluation FormAyman Ali100% (1)
- On Emergency DrugsDocument25 pagesOn Emergency DrugsBikram Chhetry100% (1)
- Caring, Curing, Coping: Nurse, Physician, and Patient RelationshipsFrom EverandCaring, Curing, Coping: Nurse, Physician, and Patient RelationshipsNo ratings yet
- Distributing Health Care: Principles, Practices and PoliticsFrom EverandDistributing Health Care: Principles, Practices and PoliticsNo ratings yet
- Population HealthDocument444 pagesPopulation HealthC R D100% (3)
- Handbook of Qualitative Health Research For Evidence-Based PracticeDocument569 pagesHandbook of Qualitative Health Research For Evidence-Based PracticeMariana LepinskyNo ratings yet
- PIIS0140673616325703Document3 pagesPIIS0140673616325703Jose Angel BarreraNo ratings yet
- Wellness Beliefs Scale PostPrintDocument32 pagesWellness Beliefs Scale PostPrintSophia YangNo ratings yet
- B MJ Defining HealthDocument4 pagesB MJ Defining HealthWathsala ShyamaliNo ratings yet
- Health Social Care Comm - 2011 - Lucock - Self Care in Mental Health Services A Narrative ReviewDocument15 pagesHealth Social Care Comm - 2011 - Lucock - Self Care in Mental Health Services A Narrative ReviewDina NabilaNo ratings yet
- September/October 2010 Leaders' LinkDocument5 pagesSeptember/October 2010 Leaders' LinkiqsolutionsNo ratings yet
- September/October 2011 Leaders' LinkDocument4 pagesSeptember/October 2011 Leaders' LinkiqsolutionsNo ratings yet
- How Should We Define Health?: BMJ (Online) July 2011Document4 pagesHow Should We Define Health?: BMJ (Online) July 2011DigiferNo ratings yet
- 2002 Bringing The Best of Medical Librarianship To TheDocument10 pages2002 Bringing The Best of Medical Librarianship To TheXavier JorgeNo ratings yet
- How Should We Define Health?: BMJ Clinical Research July 2011Document4 pagesHow Should We Define Health?: BMJ Clinical Research July 2011John Joseph SalvaleonNo ratings yet
- How Should We Define Health?: BMJ Clinical Research July 2011Document4 pagesHow Should We Define Health?: BMJ Clinical Research July 2011AbysekaNo ratings yet
- How Should We Define Health?: BMJ Clinical Research July 2011Document4 pagesHow Should We Define Health?: BMJ Clinical Research July 2011Rej HaanNo ratings yet
- Environmental, Social, and Governance: A Framework for the Future of HealthcareFrom EverandEnvironmental, Social, and Governance: A Framework for the Future of HealthcareNo ratings yet
- DiabetesDocument6 pagesDiabetesAyin FajarNo ratings yet
- How Should We Define Health?: BMJ (Online) July 2011Document4 pagesHow Should We Define Health?: BMJ (Online) July 2011Frances Iehsia VillaNo ratings yet
- I Thought I Was Not For Medical Field, Until I WasDocument5 pagesI Thought I Was Not For Medical Field, Until I WasDanica EasabelleNo ratings yet
- CHN2 JournalDocument4 pagesCHN2 JournalTAYABAN, KENNETH JAKE, Q.No ratings yet
- Harrington God Health PDFDocument28 pagesHarrington God Health PDFjulfukarNo ratings yet
- Yates-Doerr. Contando Cuerpos...Document18 pagesYates-Doerr. Contando Cuerpos...María BergeroNo ratings yet
- Why Not User Charges? The Real Issues: Greg Stoddart Morris Barer Robert Evans Vandna BhatiaDocument34 pagesWhy Not User Charges? The Real Issues: Greg Stoddart Morris Barer Robert Evans Vandna BhatiaUmair JumaniNo ratings yet
- July/August 2010 Leaders' LinkDocument3 pagesJuly/August 2010 Leaders' LinkiqsolutionsNo ratings yet
- Public Health Research PapersDocument7 pagesPublic Health Research Papersp1zajywigyd2100% (1)
- BMJdefininghealthDocument4 pagesBMJdefininghealthjab0010No ratings yet
- Evaluating Marketing Strategies in Organ DonationDocument8 pagesEvaluating Marketing Strategies in Organ DonationSharuni GanesonNo ratings yet
- Exploring Experiences of and Attitudes Towards Mental Illness and Disclosure Amongst Health Care Professionals A Qualitative StudyDocument8 pagesExploring Experiences of and Attitudes Towards Mental Illness and Disclosure Amongst Health Care Professionals A Qualitative StudyleticiaNo ratings yet
- Greymatter January2017Document8 pagesGreymatter January2017sNo ratings yet
- @does Gender and Cultural Diversity Matter For SustainabilityDocument18 pages@does Gender and Cultural Diversity Matter For SustainabilityKlislaine LimaNo ratings yet
- An International Comparison of Factors Affecting Quality of Life Among Patients With Congestive Heart Failure: A Cross-Sectional StudyDocument15 pagesAn International Comparison of Factors Affecting Quality of Life Among Patients With Congestive Heart Failure: A Cross-Sectional Studyشبلي غرايبهNo ratings yet
- Guia Laboratorio. ReglamentoDocument4 pagesGuia Laboratorio. ReglamentoNathalia MojicaNo ratings yet
- Iastate DissertationDocument8 pagesIastate DissertationWriteMyCollegePaperForMeSingapore100% (1)
- BMJdefininghealthDocument4 pagesBMJdefininghealthTibiNo ratings yet
- Annotated BibliographyDocument8 pagesAnnotated BibliographySuchitaNo ratings yet
- LC 2Document11 pagesLC 2kvargasNo ratings yet
- How Should We Define Health?: BMJ (Online) July 2011Document4 pagesHow Should We Define Health?: BMJ (Online) July 2011hmzphs kolamuruNo ratings yet
- 2 - Huber Et Al (2011) - How Shold We Define HealthDocument4 pages2 - Huber Et Al (2011) - How Shold We Define HealthCorrado BisottoNo ratings yet
- Public Health EthicsDocument17 pagesPublic Health EthicsNongre ArphonNo ratings yet
- NSG 106Document12 pagesNSG 106Anipah AmintaoNo ratings yet
- Family-Centered Health PromotionDocument4 pagesFamily-Centered Health PromotionDasha KudelskayaNo ratings yet
- Healthcare: Spirituality in Renal Supportive Care: A Thematic ReviewDocument20 pagesHealthcare: Spirituality in Renal Supportive Care: A Thematic ReviewAmna ShahNo ratings yet
- Nurturing Hope, A Human Centric Approach To Kidney Transplant Awareness and Organ Donation EducationDocument4 pagesNurturing Hope, A Human Centric Approach To Kidney Transplant Awareness and Organ Donation EducationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- How To Write A Public Health Research PaperDocument8 pagesHow To Write A Public Health Research Paperwqbdxbvkg100% (1)
- BMC Public HealthDocument28 pagesBMC Public Healthzeeleung99No ratings yet
- COVID 19 Anxiety, Peteet, J. RDocument2 pagesCOVID 19 Anxiety, Peteet, J. RJackyDanielsNo ratings yet
- The Nhs in 2030 PDFDocument48 pagesThe Nhs in 2030 PDFIsaac StanleyNo ratings yet
- Ni Hms 898083Document18 pagesNi Hms 898083Thusith WijayawardenaNo ratings yet
- Ni Hms 898083Document18 pagesNi Hms 898083Thusith WijayawardenaNo ratings yet
- Organizing Healthcare For Changing Markets: The Case of Ascension HealthDocument14 pagesOrganizing Healthcare For Changing Markets: The Case of Ascension Healtheman mamdohNo ratings yet
- Sociology of Medicine PDFDocument13 pagesSociology of Medicine PDFaditya_2k100% (1)
- Faith Healing Research PaperDocument8 pagesFaith Healing Research Paperfveec9sx100% (1)
- Gille, Felix, Sarah Smith, and Nicholas MaysDocument4 pagesGille, Felix, Sarah Smith, and Nicholas MaysMuhammad NasherNo ratings yet
- Paul Willis - Trans AdultsDocument11 pagesPaul Willis - Trans Adultsมา ยาNo ratings yet
- Acute Chest PainDocument103 pagesAcute Chest PainYajjat GargNo ratings yet
- Family Medicine I - All Questions For Final and MidtermDocument64 pagesFamily Medicine I - All Questions For Final and Midtermzdfdgsdgsh sggaesgsNo ratings yet
- Pathophysiology of Cardiogenic Pulmonary Edema - UpToDateDocument14 pagesPathophysiology of Cardiogenic Pulmonary Edema - UpToDateStefani AtlleNo ratings yet
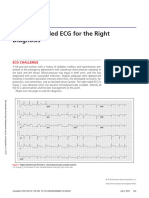
- 2018.the Right-Sided ECG For The Right DiagnosisDocument3 pages2018.the Right-Sided ECG For The Right DiagnosisWeila dos Santos VieiraNo ratings yet
- Adult, Child, and Infant Written Exam CPR Pro For The Professional RescuerDocument7 pagesAdult, Child, and Infant Written Exam CPR Pro For The Professional RescuerNguyen NamNo ratings yet
- Cardiac Function TestsDocument40 pagesCardiac Function TestsAkua Konama AttakoraNo ratings yet
- Table of Contents YjcafDocument3 pagesTable of Contents Yjcafntsn3100No ratings yet
- Practice ECGStripsDocument300 pagesPractice ECGStripsrobby zayendraNo ratings yet
- Use of Vasopressors and Inotropes - UpToDateDocument25 pagesUse of Vasopressors and Inotropes - UpToDateVictor Mendoza - MendezNo ratings yet
- ABCD2 ScoreDocument1 pageABCD2 ScoreMayo EnterprisesNo ratings yet
- Central Venous Monitoring 2022Document17 pagesCentral Venous Monitoring 2022AngieNo ratings yet
- RAAS WorksheetDocument2 pagesRAAS WorksheetParis ParisNo ratings yet
- Oefc 00 Ae Medicine 1 SB Un1Document8 pagesOefc 00 Ae Medicine 1 SB Un1Angela MercadoNo ratings yet
- CHAPTER 2 CT in CardiologyDocument9 pagesCHAPTER 2 CT in CardiologyAshvanee sharmaNo ratings yet
- Vascular Dementia: By: Omar Nuhic 4th Year Student Subject: PsychiatryDocument10 pagesVascular Dementia: By: Omar Nuhic 4th Year Student Subject: PsychiatryOmar NuhicNo ratings yet
- Test Bank For Therapeutic Exercise Foundations and Techniques 6th Edition KisnerDocument5 pagesTest Bank For Therapeutic Exercise Foundations and Techniques 6th Edition KisnerXavierKimydfj100% (29)
- Case Điện tâm đồDocument287 pagesCase Điện tâm đồSelina BerniceNo ratings yet
- Jurnal Reaading - Egi Dwi Satria Versi PDFDocument21 pagesJurnal Reaading - Egi Dwi Satria Versi PDFEgi Dwi SatriaNo ratings yet
- Heart Failure: Applied Medicine BY: Dr. Kinza IftikharDocument17 pagesHeart Failure: Applied Medicine BY: Dr. Kinza IftikharsabaamjadNo ratings yet
- Outspoken Raina Ash Full ChapterDocument77 pagesOutspoken Raina Ash Full Chapternancy.wesley488100% (3)
- Swimming Exercise: Impact of Aquatic Exercise On Cardiovascular HealthDocument11 pagesSwimming Exercise: Impact of Aquatic Exercise On Cardiovascular HealthMihail RonnyNo ratings yet
- Hypertrophic Cardiomyopathy: Joisy Aloor Leonard Shaju Smit Bhaisare Shawn RyneDocument36 pagesHypertrophic Cardiomyopathy: Joisy Aloor Leonard Shaju Smit Bhaisare Shawn RyneJoisy Aloor100% (1)
- 2 Book Clinical - Applications - and - Interaction - Between - HRV - and - Heart - RateDocument168 pages2 Book Clinical - Applications - and - Interaction - Between - HRV - and - Heart - RateJulio OliveiraNo ratings yet
- Microcirculation Monitoring - LOCAL GhalebDocument46 pagesMicrocirculation Monitoring - LOCAL GhalebGHALEB A. AlmekhlafiNo ratings yet