You might also like
- NFRC 100-2010 E0a8Document108 pagesNFRC 100-2010 E0a8Ali KassidNo ratings yet
- Ag3110apdf Mkrulebookebook RevisedDocument68 pagesAg3110apdf Mkrulebookebook RevisedRektaro100% (1)
- Recommended Price List (RPL) RPL RS.: RheinlandDocument16 pagesRecommended Price List (RPL) RPL RS.: RheinlandHemant Panpaliya100% (2)
- Modern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.From EverandModern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.No ratings yet
- TIVA Pocket Reference 2nd Edition (June 2013)Document42 pagesTIVA Pocket Reference 2nd Edition (June 2013)Charlene TanNo ratings yet
- Recipes Deep Covered Baker BookletDocument11 pagesRecipes Deep Covered Baker BookletjulilewNo ratings yet
- ARDS Concept Map - BunayogDocument2 pagesARDS Concept Map - BunayogJacela Annsyle BunayogNo ratings yet
- TM 5-2410-241-23-3Document1,284 pagesTM 5-2410-241-23-3"Rufus"100% (4)
- Ketamine HydrochlorideDocument5 pagesKetamine Hydrochlorideamin138ir100% (1)
- Siemens - Medium Voltage Equipment Range For SubstationsDocument16 pagesSiemens - Medium Voltage Equipment Range For SubstationsUrsula JohnsonNo ratings yet
- Method Statement For Laying of MCC Duct and Civil Works For MCC NetworkDocument26 pagesMethod Statement For Laying of MCC Duct and Civil Works For MCC NetworkVenkadesh PeriathambiNo ratings yet
- BOQ Fire Fighting (Hydrant) System R0 18-03-2020Document7 pagesBOQ Fire Fighting (Hydrant) System R0 18-03-2020balabhaviniNo ratings yet
- Rocky Manual PDFDocument211 pagesRocky Manual PDFRaghul Ravi88% (8)
- 2007-Catálogo Burndy ConectoresDocument724 pages2007-Catálogo Burndy ConectoresAlexis ArayNo ratings yet
- ACN - TCD Examination Techniques and InterpretationDocument8 pagesACN - TCD Examination Techniques and InterpretationHanh NguyenNo ratings yet
- Prospective Randomized Comparison of External Dacryocystorhinostomy and Endonasal Laser DacryocystorhinostomyDocument8 pagesProspective Randomized Comparison of External Dacryocystorhinostomy and Endonasal Laser DacryocystorhinostomySaaraAlleyahAlAnaziNo ratings yet
- 91 PDFDocument7 pages91 PDFsultan zeb khanNo ratings yet
- 91 PDFDocument7 pages91 PDFsultan zeb khanNo ratings yet
- The Effect of Different Sterilization Methods On PP SyringeDocument11 pagesThe Effect of Different Sterilization Methods On PP SyringeAyu WinarniNo ratings yet
- 2022-ASCO Phase II LTX-315 ACTDocument1 page2022-ASCO Phase II LTX-315 ACTichengmelody0108No ratings yet
- Comparison of Enflurane and Propofol in Electroconvulsive Therapy, A Randomized Crossover Open Preliminary Study On Seizure Duration and Anaesthetic RecoveryDocument9 pagesComparison of Enflurane and Propofol in Electroconvulsive Therapy, A Randomized Crossover Open Preliminary Study On Seizure Duration and Anaesthetic Recoverymohammad alhajNo ratings yet
- Vira-Evaluating The Clinical Efficacy of Maxillary Labial FrenectomyDocument5 pagesVira-Evaluating The Clinical Efficacy of Maxillary Labial FrenectomyBedah Mulut dan Maksilofasial 2023No ratings yet
- Pharmacology of Anaesthetic Agents II: Inhalation Anaesthetic AgentsDocument6 pagesPharmacology of Anaesthetic Agents II: Inhalation Anaesthetic Agentsmouxritsa_83No ratings yet
- 06 Applications of Office-Based 445 NM Blue Laser Transnasal Flexible Laser SurgeryDocument8 pages06 Applications of Office-Based 445 NM Blue Laser Transnasal Flexible Laser SurgeryG WNo ratings yet
- Awake Laser Laryngeal Stenosis Surgery, 2020Document5 pagesAwake Laser Laryngeal Stenosis Surgery, 2020Araceli BarreraNo ratings yet
- Endofistula Laser Ablation of Fistula-In-Ano - A New Minimally Invasive Technique For The Treatment of Fistula-In-AnoDocument6 pagesEndofistula Laser Ablation of Fistula-In-Ano - A New Minimally Invasive Technique For The Treatment of Fistula-In-AnoagusNo ratings yet
- Pharmacology of Anaesthetic Agents II: Inhalation Anaesthetic AgentsDocument6 pagesPharmacology of Anaesthetic Agents II: Inhalation Anaesthetic AgentsAna Lucia SaavedraNo ratings yet
- Comparison of MMS and CL GradingDocument8 pagesComparison of MMS and CL GradingIndhu SubbuNo ratings yet
- The CO2-laser in The Treatment of Laryngeal and Tracheal Stenosis. Our Personal Experiences. 2020Document9 pagesThe CO2-laser in The Treatment of Laryngeal and Tracheal Stenosis. Our Personal Experiences. 2020Araceli BarreraNo ratings yet
- Altan2015 N Faz ParteDocument10 pagesAltan2015 N Faz ParteAntonio LoureiroNo ratings yet
- HyperforinDocument2 pagesHyperforintangopaganNo ratings yet
- Transtympanic - Tripod - Shaped - Angiocatheter.24 - Park JM - Park SN PDFDocument6 pagesTranstympanic - Tripod - Shaped - Angiocatheter.24 - Park JM - Park SN PDFFurkan AydemirNo ratings yet
- Literature - Review - of - Surgical 2020 - Excelente ResumoDocument13 pagesLiterature - Review - of - Surgical 2020 - Excelente ResumoliligunnerNo ratings yet
- Diagnosis and Treatment of Radiation ProctitisDocument2 pagesDiagnosis and Treatment of Radiation ProctitispatNo ratings yet
- Anaesthetic Management - Release of Post Burn ContractureDocument1 pageAnaesthetic Management - Release of Post Burn ContractureMadhusudan TiwariNo ratings yet
- MKT 038Document6 pagesMKT 038peter_soósNo ratings yet
- MRN000410 BnCWy5eDocument11 pagesMRN000410 BnCWy5eAn JNo ratings yet
- Nonsurgical Treatment of Acetabular Labrum Tears: A Case SeriesDocument8 pagesNonsurgical Treatment of Acetabular Labrum Tears: A Case SeriesJonathan BaldeonNo ratings yet
- Published Spinal AmyloidosisDocument5 pagesPublished Spinal AmyloidosisJabraan JNo ratings yet
- Comparison of A Novel Aspergillus Lateral-Flow Device and TheDocument1 pageComparison of A Novel Aspergillus Lateral-Flow Device and TheIndrid RomeroNo ratings yet
- P 194 14icml-1Document1 pageP 194 14icml-1shaza elkourashyNo ratings yet
- EpinephrineDocument5 pagesEpinephrinesheynnaNo ratings yet
- Sushil Khanal, Bibhush Shrestha, Roshana Amatya, Moda Nath MarhattaDocument5 pagesSushil Khanal, Bibhush Shrestha, Roshana Amatya, Moda Nath MarhattaachyutsharmaNo ratings yet
- Inhalasi Jurnal 1Document6 pagesInhalasi Jurnal 1Fanhy liebe smartNo ratings yet
- Vascular and Endovascular Surgery Tolva Et AlDocument5 pagesVascular and Endovascular Surgery Tolva Et AlronnyNo ratings yet
- Ea Idn Injury Hkiac 2011Document2 pagesEa Idn Injury Hkiac 2011Yiu Kai WongNo ratings yet
- TACE Standards of PracticeDocument17 pagesTACE Standards of PracticeRuminRuNo ratings yet
- SVN 2021 001321Document5 pagesSVN 2021 001321viva dialysisNo ratings yet
- Renal Doppler Based Assessment of Regional Organ.18Document2 pagesRenal Doppler Based Assessment of Regional Organ.18Mario TGNo ratings yet
- Articulo YALE 2Document9 pagesArticulo YALE 2Ana Carolina Chacon GonzalezNo ratings yet
- Tomlinson Acp2010Document1 pageTomlinson Acp2010Rayan BossNo ratings yet
- 2010 Guías de Manejo de Anticoag en Proced EndoscópicosDocument15 pages2010 Guías de Manejo de Anticoag en Proced EndoscópicosSantiago AlonsoNo ratings yet
- Meeting 10 - Rismawati 190106126Document3 pagesMeeting 10 - Rismawati 190106126RismawatiNo ratings yet
- Electrical Contraction of The Anal Sphincter For Intraoperative Visualization of Anal FunctionDocument11 pagesElectrical Contraction of The Anal Sphincter For Intraoperative Visualization of Anal FunctionCaratasu Catalin CezarNo ratings yet
- Comparison Between Racemic Bupivacaine and Levobupivacaine Both Combined With Low Dose Fentanyl, Through Intrathecal Route For Transurethral Resection of ProstateDocument4 pagesComparison Between Racemic Bupivacaine and Levobupivacaine Both Combined With Low Dose Fentanyl, Through Intrathecal Route For Transurethral Resection of ProstateInternational Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- Profopol Vs KTMDocument7 pagesProfopol Vs KTMAuliaRusdiAllmuttaqienNo ratings yet
- Current Practice Issues in Thoracic Anesthesia.20Document12 pagesCurrent Practice Issues in Thoracic Anesthesia.20Claudia Isabel Rojas VazquezNo ratings yet
- 2016 Phlebology Bootun ReviewDocument10 pages2016 Phlebology Bootun ReviewronnyNo ratings yet
- RUG Tudy: Medicatio N Action Indication Contraindication Adverse Effects Nursing Considerati ONDocument4 pagesRUG Tudy: Medicatio N Action Indication Contraindication Adverse Effects Nursing Considerati ONGiselle EstoquiaNo ratings yet
- Comparison of Short Term Outcomes Between Endovenous 1940 NM Laser Ablation and 6981Document4 pagesComparison of Short Term Outcomes Between Endovenous 1940 NM Laser Ablation and 6981KHALIL JOUININo ratings yet
- Clarivein - Early Results From A Large Single-Centre Series of Mechanochemical Endovenous Ablation For Varicose VeinsDocument7 pagesClarivein - Early Results From A Large Single-Centre Series of Mechanochemical Endovenous Ablation For Varicose VeinsronnyNo ratings yet
- Chepalgia JournalDocument10 pagesChepalgia JournalRanintha SurbaktiNo ratings yet
- pRESENTASI TURBINATESDocument50 pagespRESENTASI TURBINATESPeter SalimNo ratings yet
- Dermatology: Dermatopharmacologic Investigations of Halobetasol Propionate in Comparison With Clobetasol 17-PropionateDocument8 pagesDermatology: Dermatopharmacologic Investigations of Halobetasol Propionate in Comparison With Clobetasol 17-PropionateMahfud WidianaNo ratings yet
- Actas Urológicas Españolas: Partial Laparoscopic Adrenalectomy in Primary HyperaldosteronismDocument4 pagesActas Urológicas Españolas: Partial Laparoscopic Adrenalectomy in Primary Hyperaldosteronismluis ortizNo ratings yet
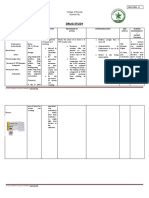
- Drug Study: La Salle UniversityDocument3 pagesDrug Study: La Salle UniversityJb RosillosaNo ratings yet
- Histological Assessment of On-Ablative Laser Stimulation of Tissue Repair in Acellular Dermal GraftsDocument8 pagesHistological Assessment of On-Ablative Laser Stimulation of Tissue Repair in Acellular Dermal GraftsLívia ZerbinatiNo ratings yet
- Module 3c-Drug StudyDocument8 pagesModule 3c-Drug StudyHaleNo ratings yet
- Ncm107rle Drugstudy Finished2Document3 pagesNcm107rle Drugstudy Finished2Charisse BulalaqueNo ratings yet
- Diaphragm Ultrasound As A New Method To Predict Extubation Outcome in Mechanically VentilaDocument7 pagesDiaphragm Ultrasound As A New Method To Predict Extubation Outcome in Mechanically VentilaSilvanaNo ratings yet
- Harvesting and Marketing Vegetables: HELE 5: Quarter 2-W3-W4Document4 pagesHarvesting and Marketing Vegetables: HELE 5: Quarter 2-W3-W4Rajon G. TulioNo ratings yet
- Nims Tariff ListDocument54 pagesNims Tariff ListsreekanthNo ratings yet
- Converters For EV PDFDocument25 pagesConverters For EV PDFasdfghjkuiytNo ratings yet
- Govt SchemeDocument46 pagesGovt SchemeBoda SrikanthNo ratings yet
- Summary G1 Newton's LawsDocument1 pageSummary G1 Newton's Laws『IntTouchz』No ratings yet
- 20MA101 Set 1Document10 pages20MA101 Set 1Dheeraj KumarNo ratings yet
- As 1074-1989 Steel Tubes and Tubulars For Ordinary ServiceDocument7 pagesAs 1074-1989 Steel Tubes and Tubulars For Ordinary ServiceSAI Global - APAC50% (2)
- Ekam - School Referal Details-2008-9Document115 pagesEkam - School Referal Details-2008-9vasanthbalaNo ratings yet
- Compositematerial Synopsis PDFDocument3 pagesCompositematerial Synopsis PDFMANJUNATH BALAGARNo ratings yet
- 08 05 Lake EcosystemDocument9 pages08 05 Lake EcosystemBharath KumarNo ratings yet
- KV-29FQ65B and OtherDocument85 pagesKV-29FQ65B and Otherstavros61No ratings yet
- PCP GQ 22021Document51 pagesPCP GQ 22021András SzántaiNo ratings yet
- Poly Gear PG en PDFDocument2 pagesPoly Gear PG en PDFAlfredo CarlosNo ratings yet
- Micrologic 2.2 / 2.3-AB: Ratings (A) in at 40°C 100 160 240 400Document1 pageMicrologic 2.2 / 2.3-AB: Ratings (A) in at 40°C 100 160 240 400Slobodan SavicNo ratings yet
- Cetpa Infotech Pvt. LTD: Department of Embedded SystemDocument42 pagesCetpa Infotech Pvt. LTD: Department of Embedded SystemKapil VijNo ratings yet
- Module 1 Practice Questions For Quiz (Anatomy and Physiology)Document2 pagesModule 1 Practice Questions For Quiz (Anatomy and Physiology)Shaina Marie RamosNo ratings yet
- Cookbook FrittataDocument2 pagesCookbook FrittataJilly CookeNo ratings yet
- Edwards, C. M. (1986) - The Running Maiden From Eleusis and The Early Classical Image of Hekate. American Journal of Archaeology, 90 (3), 307.Document17 pagesEdwards, C. M. (1986) - The Running Maiden From Eleusis and The Early Classical Image of Hekate. American Journal of Archaeology, 90 (3), 307.Denisa MateiNo ratings yet
- Just Imagin Unit 2 Test 9th Grade 1-4 Final UPDATEDDocument4 pagesJust Imagin Unit 2 Test 9th Grade 1-4 Final UPDATEDalikhalilaseelNo ratings yet
- Voice RecognitionDocument18 pagesVoice Recognitionr100% (1)