You might also like
- 2803NRS Acute Nursing Practice Exam NotesDocument18 pages2803NRS Acute Nursing Practice Exam NotesGrace CallowNo ratings yet
- Pathophysiology of Liver Cancer 2Document3 pagesPathophysiology of Liver Cancer 2Charis Paroginog92% (12)
- COVID-19 Rehabilitation Needs Questionnaire (RehabNeQ)Document7 pagesCOVID-19 Rehabilitation Needs Questionnaire (RehabNeQ)nataliu45No ratings yet
- Lesson Plan in Health 15Document2 pagesLesson Plan in Health 15Neil Declaro100% (5)
- General Form - en TypeDocument5 pagesGeneral Form - en TypeTinkercad SifatNo ratings yet
- Medical QuestionnaireDocument1 pageMedical QuestionnaireSanda AgungNo ratings yet
- Lnformation I. (RR+R: Medical QuestionnaireDocument1 pageLnformation I. (RR+R: Medical QuestionnaireMoori G BlackNo ratings yet
- Dental and Medical History FormDocument1 pageDental and Medical History FormBon QuiapoNo ratings yet
- MSA Medical QuestionnaireDocument2 pagesMSA Medical QuestionnairekqbyvmqcdmNo ratings yet
- 8. Эрүүл Мэндийн БичигDocument3 pages8. Эрүүл Мэндийн БичигOtgonbayar BattogtokhNo ratings yet
- Medical Conditions Declaration Form1Document1 pageMedical Conditions Declaration Form1Khôi Mạc NguyênNo ratings yet
- Health CertificateDocument3 pagesHealth CertificateĐĂNG TRỊNH HẢINo ratings yet
- Physiotherapy Patient History FormDocument5 pagesPhysiotherapy Patient History FormJean Pierre del Aguila MattaNo ratings yet
- Physio Assess Form Oct 2022Document5 pagesPhysio Assess Form Oct 2022RishaadNo ratings yet
- Physician S Report FormDocument4 pagesPhysician S Report FormpaolaNo ratings yet
- General Medical History Form PDFDocument1 pageGeneral Medical History Form PDFണг. ധн¡тε H̶A̶T̶No ratings yet
- Health Questionnaire: Name (Please Print)Document1 pageHealth Questionnaire: Name (Please Print)CarlosSchlozJuniorNo ratings yet
- Physician's Report Form: Part A (Completed by The Applicant) 1. 2. 3Document4 pagesPhysician's Report Form: Part A (Completed by The Applicant) 1. 2. 3Arturo MBNo ratings yet
- Medical Screening Questionnaire: Before You BeginDocument6 pagesMedical Screening Questionnaire: Before You Begins9sxxtjmqjNo ratings yet
- Health CheckDocument9 pagesHealth Checkamoon08.arNo ratings yet
- PagesDocument4 pagesPagesjanicewhismanNo ratings yet
- Ad01f4 Reyes, Althea Jeslyn CDocument2 pagesAd01f4 Reyes, Althea Jeslyn C[AP-Student] Althea Jeslyn ReyesNo ratings yet
- Antenatal Booking ProformaDocument10 pagesAntenatal Booking ProformaracaneteNo ratings yet
- Be Review of Systems Questionairet 122714Document1 pageBe Review of Systems Questionairet 122714Djev David DazaNo ratings yet
- Medical History QuestionnaireDocument1 pageMedical History QuestionnaireHare MasterYodaNo ratings yet
- COVID-19 Screening Form ... : Patient's Name: Date: DateDocument2 pagesCOVID-19 Screening Form ... : Patient's Name: Date: DateMichaelaKatrinaTrinidadNo ratings yet
- OGUK Medical FormDocument7 pagesOGUK Medical Formum erNo ratings yet
- Health Questionnaire Copy1Document2 pagesHealth Questionnaire Copy1dcNo ratings yet
- International Travel Medical QuestionnaireDocument4 pagesInternational Travel Medical QuestionnairecristinaNo ratings yet
- Health Questionnaire: Private & ConfidentialDocument3 pagesHealth Questionnaire: Private & Confidentialjames pownallNo ratings yet
- Your Full NameDocument2 pagesYour Full NameVagamundos ArgentinosNo ratings yet
- Full NameDocument2 pagesFull NameSaufa CenterNo ratings yet
- GeorgeDocument2 pagesGeorgeSteve MaguireNo ratings yet
- Soap Note 2 Alyssa MatulichDocument8 pagesSoap Note 2 Alyssa Matulichapi-456313554No ratings yet
- Pe Form (Cosare, Alessandra Maxinne E.-Dmd-1-Canine)Document6 pagesPe Form (Cosare, Alessandra Maxinne E.-Dmd-1-Canine)MoyeonieNo ratings yet
- Medicalhistoryformpg 1Document2 pagesMedicalhistoryformpg 1reynanfrancebernabeNo ratings yet
- BiodataDocument1 pageBiodataSaufa CenterNo ratings yet
- Health and Safety BlueDocument2 pagesHealth and Safety BlueAnonymous KWI6BGdLlJNo ratings yet
- Baseline Occupational Medical Evaluation Proposed Reporting Revised FormatDocument3 pagesBaseline Occupational Medical Evaluation Proposed Reporting Revised FormatAhmed OsmanNo ratings yet
- Adult in TakeDocument9 pagesAdult in TakeNaura CorporationNo ratings yet
- Health Declaration FormDocument1 pageHealth Declaration Formhasminkjk97No ratings yet
- MedFest Health History and Physical Exam Form NON US Programs FillableDocument4 pagesMedFest Health History and Physical Exam Form NON US Programs Fillableshariff gutierrezNo ratings yet
- Fitness Assessment Questionnaire PDFDocument4 pagesFitness Assessment Questionnaire PDFKatrina Pillagara0% (1)
- Daily Health Assessment Form - Student and ParentDocument1 pageDaily Health Assessment Form - Student and Parentapi-269483056No ratings yet
- Your Lifestyle QuestionaireDocument2 pagesYour Lifestyle QuestionairevaluedynamicmarineNo ratings yet
- Self Completion Medical History Form - PregnancyDocument4 pagesSelf Completion Medical History Form - PregnancymerjenNo ratings yet
- Health HistoryDocument2 pagesHealth History224edgebNo ratings yet
- Additional Questions Case Study FinalsDocument7 pagesAdditional Questions Case Study FinalsMia Grace GarciaNo ratings yet
- Health Declaration For Care 4 U Policy / Medical InsuranceDocument2 pagesHealth Declaration For Care 4 U Policy / Medical InsuranceMarco AglibotNo ratings yet
- Reflexology New Patient FormDocument7 pagesReflexology New Patient FormOana Iftimie100% (2)
- Medical Self Declaration FormDocument1 pageMedical Self Declaration FormVarun SinglaNo ratings yet
- Medical History Taking FormDocument6 pagesMedical History Taking FormRoanne DivinagraciaNo ratings yet
- Diabetes Hyperten Sion Anemia Palpitati On Tubercul Osis Breathle Ssness Epilepsy Jaundice MalariaDocument1 pageDiabetes Hyperten Sion Anemia Palpitati On Tubercul Osis Breathle Ssness Epilepsy Jaundice MalariaphanikrishnabNo ratings yet
- Global COVID-19 Clinical PlatformDocument8 pagesGlobal COVID-19 Clinical PlatformMaria Do SocorroNo ratings yet
- The Technical University of KenyaDocument3 pagesThe Technical University of Kenyalixus mwangi100% (1)
- Dengue Reporting FormDocument5 pagesDengue Reporting FormAbhi ShahNo ratings yet
- Screenshot 2022-06-28 at 9.33.56 AM PDFDocument1 pageScreenshot 2022-06-28 at 9.33.56 AM PDFhelen S. DeeNo ratings yet
- Lifestyle Assessment FormDocument2 pagesLifestyle Assessment FormBbg011No ratings yet
- Health Certificate PDFDocument2 pagesHealth Certificate PDFPedro KunstNo ratings yet
- Health SummaryDocument2 pagesHealth SummaryFrank RenNo ratings yet
- Patient Assessment Form For AdultsDocument2 pagesPatient Assessment Form For AdultsAriane CauanNo ratings yet
- 2020 Flu Vaccination Consent FormDocument1 page2020 Flu Vaccination Consent FormJoan LeeNo ratings yet
- Hypertensive Disorders of Pregnancy 33Document36 pagesHypertensive Disorders of Pregnancy 33Asteway MesfinNo ratings yet
- Cardiac Murmurs in Children: FactfileDocument2 pagesCardiac Murmurs in Children: FactfileResya I. NoerNo ratings yet
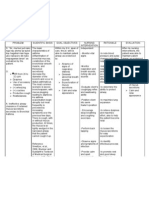
- Nursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationDocument8 pagesNursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationKrahNo ratings yet
- Module 1: Foundations of Health Assessment: Lesson 1: Physical Examination and History Taking: OverviewDocument10 pagesModule 1: Foundations of Health Assessment: Lesson 1: Physical Examination and History Taking: OverviewEmily BernatNo ratings yet
- Ineffective Airway ClearanceDocument1 pageIneffective Airway ClearancejomerdalonaNo ratings yet
- Drug Study Atropine SulfateDocument1 pageDrug Study Atropine Sulfateirhizzp75% (8)
- Duchene Muscular DystrophyDocument5 pagesDuchene Muscular Dystrophykshaf muzammil100% (1)
- Proximal BicepsDocument23 pagesProximal BicepsPrabath ChinthakaNo ratings yet
- Medical-Surgical Nursing Care: Caring For Clients With Diabetes MellitusDocument90 pagesMedical-Surgical Nursing Care: Caring For Clients With Diabetes MellitusJonalynCollodChewacheoNo ratings yet
- GDS K-6 - Newborn Physical ExaminationDocument44 pagesGDS K-6 - Newborn Physical ExaminationJosephine IrenaNo ratings yet
- CASE STUDY (ABNORMAL PREGNANCY) .Edited (2)Document9 pagesCASE STUDY (ABNORMAL PREGNANCY) .Edited (2)niyoc68859No ratings yet
- Psychiatry Passmedicine & Onexamination Notes 2016 PDFDocument34 pagesPsychiatry Passmedicine & Onexamination Notes 2016 PDFJyothi ReddyNo ratings yet
- ConcorDocument40 pagesConcorviczNo ratings yet
- Hematologic System Practice QuestionsDocument3 pagesHematologic System Practice QuestionsJoslyn GrossNo ratings yet
- Association Between Liver Cirrhosis and Diabetes Mellitus: A Review On Hepatic OutcomesDocument15 pagesAssociation Between Liver Cirrhosis and Diabetes Mellitus: A Review On Hepatic Outcomesdoremi miredoNo ratings yet
- 3 Combined AHA BLS ACLS Updates CombinedDocument5 pages3 Combined AHA BLS ACLS Updates Combinedamanrup randhawa100% (1)
- History and Physical Exam For COPDDocument2 pagesHistory and Physical Exam For COPDKarenJulioNo ratings yet
- Riltrava Aerosphere Epar Product Information enDocument42 pagesRiltrava Aerosphere Epar Product Information enshihyanghuangNo ratings yet
- "Bloody Scours": Swine DysenteryDocument29 pages"Bloody Scours": Swine DysenteryleaNo ratings yet
- Pre EclampsiaDocument13 pagesPre EclampsiaEniamrahs DnalonNo ratings yet
- Psychotherapy DAP NoteDocument2 pagesPsychotherapy DAP NoteMistor Williams100% (1)
- Tomografía Computarizada para El Diagnóstico de La Apendicitis Aguda en Pacientes AdultosDocument199 pagesTomografía Computarizada para El Diagnóstico de La Apendicitis Aguda en Pacientes AdultosMarco Jimenez HerreraNo ratings yet
- Laser Therapy ProtocolsDocument89 pagesLaser Therapy ProtocolsSYED ALI HUSSAINNo ratings yet
- CyanosisDocument11 pagesCyanosissr_sushil100% (1)
- Arizona Communicable Disease FlipchartDocument98 pagesArizona Communicable Disease Flipchartapi-308905421No ratings yet
- AHRQ Safety Program For Mechanically Ventilated PatientsDocument21 pagesAHRQ Safety Program For Mechanically Ventilated PatientsRosmira Agreda CabreraNo ratings yet
- Urnal Vox Sanguinis - 2023 - Pons - Prevalence of Red Blood Cell Alloantibodies Among Blood Donors in The French Military BloodDocument5 pagesUrnal Vox Sanguinis - 2023 - Pons - Prevalence of Red Blood Cell Alloantibodies Among Blood Donors in The French Military BloodFauzan.ANo ratings yet