You might also like
- Sample of PleadingsDocument3 pagesSample of PleadingsShiela Pilar100% (8)
- QRQC / 8D Form: D 1. Description of The ProblemDocument5 pagesQRQC / 8D Form: D 1. Description of The ProblemDearRed FrankNo ratings yet
- Agency Movement Form: General InformationDocument1 pageAgency Movement Form: General InformationAracelli EnerioNo ratings yet
- BALTIC EXCHANGE - GuidetoMarketBenchmarksDocument143 pagesBALTIC EXCHANGE - GuidetoMarketBenchmarksEisilisNo ratings yet
- TML-PSC-SQ Manufacturing Site Assessment Rev 2.0Document24 pagesTML-PSC-SQ Manufacturing Site Assessment Rev 2.0Narendran MNo ratings yet
- Business Requirements Document Template 38Document8 pagesBusiness Requirements Document Template 38BA PRENEURNo ratings yet
- ZPC Official Forms Ref: Zof: Vendor Information Sheet Form SpecificationsDocument10 pagesZPC Official Forms Ref: Zof: Vendor Information Sheet Form SpecificationsTodd E. L. UychocdeNo ratings yet
- FS - MM - Vendor PO Eligible ItemsDocument14 pagesFS - MM - Vendor PO Eligible ItemsSUBHOJIT BANERJEENo ratings yet
- RP50130 RTC 475 FS RP Production Tracking ReportDocument16 pagesRP50130 RTC 475 FS RP Production Tracking Reportravi4920No ratings yet
- Individual Performance Commitment and Review (Ipcr) Form: Social Security System Strategic Performance Management SystemDocument1 pageIndividual Performance Commitment and Review (Ipcr) Form: Social Security System Strategic Performance Management SystemSam LagoNo ratings yet
- TD.57 CR1067Document3 pagesTD.57 CR1067govindkushwahaNo ratings yet
- Water Flow Sensor YF-B3: Search For Products, Brands and PlatformsDocument3 pagesWater Flow Sensor YF-B3: Search For Products, Brands and PlatformsJaeger CRNo ratings yet
- Func Spec For New Output Creation For Nigeria Invoice PrintingDocument11 pagesFunc Spec For New Output Creation For Nigeria Invoice PrintingJagan MohanNo ratings yet
- Write Invest X RiteDocument13 pagesWrite Invest X RiteMustapha ElouafiNo ratings yet
- E4E - A - ES - GL - DT - Interface - INT - GL - 009 - XCNEC01E y XCFEC04E - v1.0Document44 pagesE4E - A - ES - GL - DT - Interface - INT - GL - 009 - XCNEC01E y XCFEC04E - v1.0JaimeNo ratings yet
- Professional Pilot Survey ReportDocument17 pagesProfessional Pilot Survey ReportFake IDNo ratings yet
- PR Request Amkor TNR 05152023Document12 pagesPR Request Amkor TNR 05152023Shiela May HerreraNo ratings yet
- MIS Assignment: Systems Approach and CyberneticsDocument6 pagesMIS Assignment: Systems Approach and CyberneticsmrityunjayNo ratings yet
- 3.1.9.1 - SD - Sales Plan - V1.0Document11 pages3.1.9.1 - SD - Sales Plan - V1.0zahid atiqNo ratings yet
- Dpramx06 - Hand Over Procedure.v1.3Document10 pagesDpramx06 - Hand Over Procedure.v1.3NoekKeijzerNo ratings yet
- Functional Specification: Bajaj Power Generation BusinessDocument5 pagesFunctional Specification: Bajaj Power Generation BusinessBipul KumarNo ratings yet
- 5 DILEEP Group Business Plan FormatDocument6 pages5 DILEEP Group Business Plan FormatJullie Kaye Frias Diamante100% (1)
- Ministry Loan Empowerment Application Form FinalDocument15 pagesMinistry Loan Empowerment Application Form FinalAndrew LukupwaNo ratings yet
- (New) - On Boarding Cessation Checklist FormDocument4 pages(New) - On Boarding Cessation Checklist Formpermata.klasik1998No ratings yet
- Implementation /tech. Support SheetDocument7 pagesImplementation /tech. Support SheetAbbas SyedNo ratings yet
- FC0007 ETDesign 0319Document9 pagesFC0007 ETDesign 0319Kenny Junior Mercedes RojasNo ratings yet
- Fda FormDocument14 pagesFda FormCharry MarquezNo ratings yet
- 20 FICO Tips - Series 2 - SAP BlogsDocument27 pages20 FICO Tips - Series 2 - SAP BlogsAnanthakumar ANo ratings yet
- Kasus Bentoel Big DataDocument41 pagesKasus Bentoel Big Datavita sarasi100% (1)
- Abap Func - SpecDocument7 pagesAbap Func - SpecKumar AjitNo ratings yet
- FSDocument15 pagesFSsathrughna thotaNo ratings yet
- GASS New Access Request Form JSOX Dealer v1.9Document2 pagesGASS New Access Request Form JSOX Dealer v1.9Chamsu EddinNo ratings yet
- 2 - 685 - PPAP PSW Submission+checklist - instructions+FAU F SPG 2430 EN 4Document8 pages2 - 685 - PPAP PSW Submission+checklist - instructions+FAU F SPG 2430 EN 4Helton MotaNo ratings yet
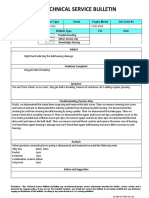
- Technical Service Bulletin: Manufacturer Machine Type Series Engine Model Job Order NoDocument3 pagesTechnical Service Bulletin: Manufacturer Machine Type Series Engine Model Job Order NoKhincho ayeNo ratings yet
- Introduction To Teleperformance Greece - May 2016Document31 pagesIntroduction To Teleperformance Greece - May 2016The Tun 91No ratings yet
- DFMEA - Robustness in Design Package - BlankTemplateDocument20 pagesDFMEA - Robustness in Design Package - BlankTemplateMoham'medAlthafAs'lamNo ratings yet
- Case - CFF GALA Rev 1 12-7-2023 1-51-11 PMDocument2 pagesCase - CFF GALA Rev 1 12-7-2023 1-51-11 PMIjoel Chuvu Part IINo ratings yet
- Case - CFF GALA Rev 1 12-11-2023 10-30-31 AMDocument2 pagesCase - CFF GALA Rev 1 12-11-2023 10-30-31 AMIjoel Chuvu Part IINo ratings yet
- FPTFC PUR SOP Procurement ProcedureDocument6 pagesFPTFC PUR SOP Procurement ProcedureDivina CelestialNo ratings yet
- COA Prescribed FormDocument32 pagesCOA Prescribed FormEden EscaloNo ratings yet
- Apqp Timing Plan...Document5 pagesApqp Timing Plan...Gourav SainiNo ratings yet
- ABM 8 B PlanDocument12 pagesABM 8 B PlanLovely MapiliNo ratings yet
- FS - MM - Vendor GET OPEN PO DETAILSDocument13 pagesFS - MM - Vendor GET OPEN PO DETAILSSUBHOJIT BANERJEENo ratings yet
- Waste Materials Report: Serial Nos.Document5 pagesWaste Materials Report: Serial Nos.Dumfergie KinkitoNo ratings yet
- OTC FS 4.7.2 ENH0689 EU Ehancements For Seeburger MapsDocument12 pagesOTC FS 4.7.2 ENH0689 EU Ehancements For Seeburger MapsdarapuNo ratings yet
- On Field Mission MascaraDocument24 pagesOn Field Mission MascaraAbdallah CHETTAHNo ratings yet
- Attachment 0Document86 pagesAttachment 0GuiguitoNo ratings yet
- 2023 Alumni Be Coach - Supercharge Efficiency and Scalability in A Big Multinational Company With Cutting-Edge TechnologyDocument28 pages2023 Alumni Be Coach - Supercharge Efficiency and Scalability in A Big Multinational Company With Cutting-Edge TechnologyRangga AdityaNo ratings yet
- Toshiba Support - Self-Service Receipt 170220Document2 pagesToshiba Support - Self-Service Receipt 170220Enrique Alfredo Sánchez PérezNo ratings yet
- Case - CFF GALA Rev 1 12-11-2023 10-39-48 AMDocument2 pagesCase - CFF GALA Rev 1 12-11-2023 10-39-48 AMIjoel Chuvu Part IINo ratings yet
- Borang RCA Report For KPI HPIADocument5 pagesBorang RCA Report For KPI HPIAashikin zamaludinNo ratings yet
- Recipient Committee Campaign Statement Cover PageDocument8 pagesRecipient Committee Campaign Statement Cover Pageapi-28862363No ratings yet
- FS DOCUMENT - FOR Tynor ZFOR IssueDocument3 pagesFS DOCUMENT - FOR Tynor ZFOR IssueSumit KumarNo ratings yet
- Functional Specification: Bajaj Power Generation BusinessDocument5 pagesFunctional Specification: Bajaj Power Generation BusinessBipul KumarNo ratings yet
- Memorandum: To: From: CC: Date: Subject: Standard Site Visit Report (SVR)Document3 pagesMemorandum: To: From: CC: Date: Subject: Standard Site Visit Report (SVR)Cisco MontalvoNo ratings yet
- Channel Strategy and Positioning: Group No - 4Document11 pagesChannel Strategy and Positioning: Group No - 4Nitin GoyalNo ratings yet
- GRP4Integrated Application Form XLSX FormatDocument15 pagesGRP4Integrated Application Form XLSX FormatIsabel PeraltaNo ratings yet
- 13sep Tabar MatthewDocument69 pages13sep Tabar MatthewMuhammad FaizanNo ratings yet
- User Request Form - 300721 - Open User Access For Zukhra Hasmin SSDocument2 pagesUser Request Form - 300721 - Open User Access For Zukhra Hasmin SSSony KristantoNo ratings yet
- Volume I I BookletDocument136 pagesVolume I I BookletDhamu Baby RajNo ratings yet
- Annex VII Revised Claims Procedure PMJJBY - 17062021Document3 pagesAnnex VII Revised Claims Procedure PMJJBY - 17062021Ratnesh KumarNo ratings yet
- McCarthy (2009) McCarty On Trademarks and Unfair CompetitionDocument9 pagesMcCarthy (2009) McCarty On Trademarks and Unfair CompetitionGiriNo ratings yet
- Tort Law Week 9: Dr. Megan Rae Blakely M.blakely@lancaster - Ac.ukDocument26 pagesTort Law Week 9: Dr. Megan Rae Blakely M.blakely@lancaster - Ac.ukDroidOfDoom HunterLeoNo ratings yet
- Edited Certificate of Completion in Work ImmersionDocument21 pagesEdited Certificate of Completion in Work Immersionfrederick sorianoNo ratings yet
- 2286 - Criminal Law II TestDocument2 pages2286 - Criminal Law II TestAkello Winnie princesNo ratings yet
- Birla Navya DeckDocument60 pagesBirla Navya Decksushil aroraNo ratings yet
- Annulment of Arbitral AwardsDocument29 pagesAnnulment of Arbitral AwardsmhamrawyNo ratings yet
- Abella v. Francisco, 55 Phil. 447 (1931)Document4 pagesAbella v. Francisco, 55 Phil. 447 (1931)Cza PeñaNo ratings yet
- SBD-Procurement of Plant Design Supply Installation-Revised February2018Document324 pagesSBD-Procurement of Plant Design Supply Installation-Revised February2018GeorgeNo ratings yet
- 2 Schedule ADocument82 pages2 Schedule Axue jun xiangNo ratings yet
- Con Law I Case ChartDocument22 pagesCon Law I Case ChartTristen LarsonNo ratings yet
- Order 41 Rule 27Document3 pagesOrder 41 Rule 27साकेत मिश्राNo ratings yet
- What Is The Difference Between A LawyerDocument3 pagesWhat Is The Difference Between A LawyerFRANCISCA CAROLINA LILLONo ratings yet
- Revised Joinder AgreementDocument5 pagesRevised Joinder AgreementNate BoroyanNo ratings yet
- Secretary'S Certificate: Know All Men by These PresentsDocument2 pagesSecretary'S Certificate: Know All Men by These PresentsEspina Rizzvill100% (1)
- Od 226180983725961000Document2 pagesOd 22618098372596100021Keshav C7ANo ratings yet
- Callister7e SM Ch03 25Document1 pageCallister7e SM Ch03 25Kassandra Keila Fernandes CostaNo ratings yet
- The Central Vista Project: A Brief DescriptionDocument11 pagesThe Central Vista Project: A Brief DescriptionKrinsh Jagiasi100% (3)
- Ketua Pengarah Pertubuhan Keselamatan Sosial V RajaparaDocument4 pagesKetua Pengarah Pertubuhan Keselamatan Sosial V RajaparanroshaNo ratings yet
- Carino Vs Carino 351 SCRA 127Document7 pagesCarino Vs Carino 351 SCRA 127Avatar09No ratings yet
- Pharmacokinetics of Antimicrobial DosingDocument3 pagesPharmacokinetics of Antimicrobial DosingAnisa FitriyahNo ratings yet
- Case No.18: Paulino M. Alecha vs. Jose L. Atienza JRDocument1 pageCase No.18: Paulino M. Alecha vs. Jose L. Atienza JRAlmiraNo ratings yet
- Hall Ticket: Date and Time of Examination: Venue of ExaminationDocument1 pageHall Ticket: Date and Time of Examination: Venue of Examinationmudassir mNo ratings yet
- Compliance Checklist PDFDocument37 pagesCompliance Checklist PDFShamli ShahNo ratings yet
- Tutorial Questions Week 8: Anonymous Data Are Recorded So That The Information Can Never Be Linked ToDocument4 pagesTutorial Questions Week 8: Anonymous Data Are Recorded So That The Information Can Never Be Linked Tosanjeet kumarNo ratings yet
- A Comparative Study Between Muslim Gift and WillDocument10 pagesA Comparative Study Between Muslim Gift and WillNewbieGamers - নিউবি গেমার্সNo ratings yet
- Recio v. Recio DigestDocument1 pageRecio v. Recio DigestMikee CandelariaNo ratings yet