You might also like
- Moonlight PDFDocument371 pagesMoonlight PDFFerzada Sajiran100% (2)
- Lab ValuesDocument68 pagesLab ValuesJayr ValmoresNo ratings yet
- AQA Biology Unit 1: Revision Notes: myrevisionnotes, #1From EverandAQA Biology Unit 1: Revision Notes: myrevisionnotes, #1Rating: 5 out of 5 stars5/5 (2)
- Last Minute RevisionDocument63 pagesLast Minute RevisionSachin Shukla100% (1)
- Introduction To Blood and PhlebotomyDocument149 pagesIntroduction To Blood and PhlebotomyTahir AzizNo ratings yet
- Csec HSB June 2011 p2Document16 pagesCsec HSB June 2011 p2Sachin Bahadoorsingh100% (1)
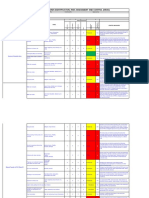
- HIRAC Electrical Installation For Temporary SupplyDocument7 pagesHIRAC Electrical Installation For Temporary Supplyanton jr clemente75% (4)
- Introduction To Waterborne PathogensDocument60 pagesIntroduction To Waterborne PathogensSyed Alwi Alattas100% (1)
- Third Quarter Exam Mapeh Grade 10Document4 pagesThird Quarter Exam Mapeh Grade 10Lanie Tamacio Baday100% (1)
- Examination of UrineDocument7 pagesExamination of UrineDaniel LamasonNo ratings yet
- Communicable Nursing - LecturervDocument329 pagesCommunicable Nursing - LecturervCarl WaletNo ratings yet
- Dengue Lesson PlanDocument12 pagesDengue Lesson Plankarlacamilledeleon100% (7)
- Micro - para FINALDocument53 pagesMicro - para FINALfilchibuff94% (18)
- Need To Memorize For NCLEXDocument12 pagesNeed To Memorize For NCLEXmyra0462100% (2)
- Contrast Media and Adverse Effects - Vijay KumarDocument41 pagesContrast Media and Adverse Effects - Vijay KumarTapshi SohalNo ratings yet
- IMCIDocument2 pagesIMCIsweet_lily_valleyNo ratings yet
- MULTIPLE CHOICE. Read The Following Questions and Choose The Best Answer by Shading TheDocument14 pagesMULTIPLE CHOICE. Read The Following Questions and Choose The Best Answer by Shading ThePrince Mark BadilloNo ratings yet
- Concept Communicable DiseasesDocument421 pagesConcept Communicable DiseasesJoric Magusara91% (11)
- Randox ControlDocument103 pagesRandox ControlSunlifecare CardNo ratings yet
- Name of Chemical: Clothianidin Reason For Issuance: Conditional Registration Date Issued: May 30, 2003Document19 pagesName of Chemical: Clothianidin Reason For Issuance: Conditional Registration Date Issued: May 30, 2003Laney SommerNo ratings yet
- Food Control: Sciverse SciencedirectDocument7 pagesFood Control: Sciverse SciencedirectAdriana CerlincaNo ratings yet
- LMR 2020Document106 pagesLMR 2020VideoScoNo ratings yet
- In Vitro Food Diagnostics: CompanyDocument32 pagesIn Vitro Food Diagnostics: CompanyFamar HiveNo ratings yet
- Arcella Et al-2016-EFSA JournalDocument32 pagesArcella Et al-2016-EFSA JournalhüseyinNo ratings yet
- Concentrations of Veterinary Drug Residues in Milk From Individual Farms in CroatiaDocument8 pagesConcentrations of Veterinary Drug Residues in Milk From Individual Farms in CroatiaAlemayehu LetNo ratings yet
- Tetralogy of Fallot: Supervisor: Dr. Muhammad Ali, Sp.A (K) Presentator: Citra Aryanti 080100050 Marianto 080100112Document48 pagesTetralogy of Fallot: Supervisor: Dr. Muhammad Ali, Sp.A (K) Presentator: Citra Aryanti 080100050 Marianto 080100112Faskanita NadapdapNo ratings yet
- 30 210 Coulomn and Nitrogen Carrier Gas.: Agricultural Prac-TiceDocument8 pages30 210 Coulomn and Nitrogen Carrier Gas.: Agricultural Prac-TiceIkne Kecil BhaktivedantaNo ratings yet
- Epidemiology Practical IA Answers-12-9-23Document5 pagesEpidemiology Practical IA Answers-12-9-23KirNo ratings yet
- Bacteriology OSPEDocument20 pagesBacteriology OSPEKrithik B Rajesh100% (1)
- Biological Water Quality ParametersDocument26 pagesBiological Water Quality ParametersNikhil C me18s303No ratings yet
- 5.nutrition Study and Quality Assurance Analysis by HPLCaaDocument65 pages5.nutrition Study and Quality Assurance Analysis by HPLCaayen88tvNo ratings yet
- Microbial Analysis of FoodDocument77 pagesMicrobial Analysis of FoodAbdurrazaq YakubuNo ratings yet
- Factores Intrin ExtrinsDocument12 pagesFactores Intrin ExtrinsIsa Cessa CarvajalNo ratings yet
- Protein Energy Malnutrition (PEM)Document30 pagesProtein Energy Malnutrition (PEM)stephen X-SILVERNo ratings yet
- Ultimate Comprehensive ABSITE Study Guide1Document125 pagesUltimate Comprehensive ABSITE Study Guide1Steven GodelmanNo ratings yet
- NEJM appendixPDF2020Document7 pagesNEJM appendixPDF2020Marin AndreiNo ratings yet
- Top 93 Nursing Skills, Procedures and Normal Values - OkDocument26 pagesTop 93 Nursing Skills, Procedures and Normal Values - OkWilmaBongotanPadawil100% (1)
- Tropane Alkoloids Food Chemistry 331Document9 pagesTropane Alkoloids Food Chemistry 331tunalizadeNo ratings yet
- 01-The Rest of The Story CDSDocument12 pages01-The Rest of The Story CDSvdusanNo ratings yet
- Development and Validation of A Green HPLC Method For The Analysis ofDocument10 pagesDevelopment and Validation of A Green HPLC Method For The Analysis ofNguyễn Phú SỹNo ratings yet
- Pancreatic Function TestDocument9 pagesPancreatic Function TestAyioKunNo ratings yet
- REVIEW NOTES Things To RememberDocument37 pagesREVIEW NOTES Things To RememberblazegomezNo ratings yet
- MALONDIALDEHYDE - IARC (1985) and The Compound Was Classified in IARCDocument11 pagesMALONDIALDEHYDE - IARC (1985) and The Compound Was Classified in IARCPritta TaradipaNo ratings yet
- Sc. College Journal Res.72Document174 pagesSc. College Journal Res.72Pratik AmanNo ratings yet
- Summary Diet and Health Lecture 1-14Document30 pagesSummary Diet and Health Lecture 1-14Safira100% (1)
- Bacteria ToxicologyDocument37 pagesBacteria ToxicologyFrank FontaineNo ratings yet
- And Their Relation To Birth SizeDocument13 pagesAnd Their Relation To Birth SizeYagnesh SutharNo ratings yet
- Indicator OrganismsDocument17 pagesIndicator Organisms27- Sadhana YadavNo ratings yet
- Campylobacter PDFDocument78 pagesCampylobacter PDFKhushi PatelNo ratings yet
- Anti-Carcinogenic Properties of Solanum Melongena (Eggplant) Fruit and Leaf Extracts in Vitro Camilo-Laguardia-LuceroDocument15 pagesAnti-Carcinogenic Properties of Solanum Melongena (Eggplant) Fruit and Leaf Extracts in Vitro Camilo-Laguardia-Luceronino corpuzNo ratings yet
- Body FluidsDocument24 pagesBody FluidsMohamed MidoNo ratings yet
- FOOD AND NUTRITIONAL ANALYSIS Fruits and Fruit Products-334-341Document8 pagesFOOD AND NUTRITIONAL ANALYSIS Fruits and Fruit Products-334-341fernandoferozNo ratings yet
- Brain Dump FinalDocument6 pagesBrain Dump FinalMarilia FarensenaNo ratings yet
- Fish Disease & ManagementDocument54 pagesFish Disease & ManagementShakeel KhanNo ratings yet
- Animl NutriDocument12 pagesAniml NutriGregory M. CoronadoNo ratings yet
- Reduction of Salmonella Enteritidis Population Sizes On Almond Kernels With Infrared HeatDocument8 pagesReduction of Salmonella Enteritidis Population Sizes On Almond Kernels With Infrared HeatDiana StetcoNo ratings yet
- Corn Straw: Function and Dysfunction of The Rumi-Nant ForestomachDocument24 pagesCorn Straw: Function and Dysfunction of The Rumi-Nant ForestomachShahzaib FaisalNo ratings yet
- Case Report Tyhoid FeverDocument48 pagesCase Report Tyhoid FeverDesyHandayaniNo ratings yet
- Determination of Uric AcidDocument4 pagesDetermination of Uric AcidHasan ShahriarNo ratings yet
- Chemical HazardDocument22 pagesChemical HazardkhayleeNo ratings yet
- Antimicrobial Effect of Rosemary ExtractsDocument10 pagesAntimicrobial Effect of Rosemary ExtractsNgân KimNo ratings yet
- Food MCB II NotesDocument73 pagesFood MCB II NotesRichard Simon KisituNo ratings yet
- Ansc321 Lab Exam Study GuideDocument7 pagesAnsc321 Lab Exam Study Guideapi-585093321No ratings yet
- Dengue Haemorrhagic Fever: Case ReportDocument37 pagesDengue Haemorrhagic Fever: Case ReportmhimiNo ratings yet
- Acido Ibotenico en Amanita MuscariaDocument4 pagesAcido Ibotenico en Amanita MuscariaSergio Rockdríguez LealNo ratings yet
- AUB - Physical Examination of UrineDocument3 pagesAUB - Physical Examination of UrineJeanne RodiñoNo ratings yet
- An Enzyme Linked Immunosorbent Assay ELISA For The Major Crustacean Allergen Tropomyosin in Food PDFDocument11 pagesAn Enzyme Linked Immunosorbent Assay ELISA For The Major Crustacean Allergen Tropomyosin in Food PDFVeronica DrgNo ratings yet
- Bacteriological Water AnalysisDocument6 pagesBacteriological Water Analysisramkrishna01No ratings yet
- Part 1 CD Mastery TestDocument15 pagesPart 1 CD Mastery TestRika MaeNo ratings yet
- D.S.S Aiims Prepration Test Series: (B) Rabies (C) Diphtheria (D) Measles (E) TetanusDocument6 pagesD.S.S Aiims Prepration Test Series: (B) Rabies (C) Diphtheria (D) Measles (E) TetanusDr-Sanjay SinghaniaNo ratings yet
- National Guidelines On Management of Dengue Fever & Dengue Haemorrhagic Fever in Children and Adolescents - Sri LankaDocument53 pagesNational Guidelines On Management of Dengue Fever & Dengue Haemorrhagic Fever in Children and Adolescents - Sri LankaNational Dengue Control Unit,Sri Lanka100% (1)
- Dengue Virus - A Global Human Threat - Review of LiteratureDocument6 pagesDengue Virus - A Global Human Threat - Review of LiteratureSadio KeitaNo ratings yet
- Dengue QuizDocument10 pagesDengue QuizAfifah SelamatNo ratings yet
- Dengue-Malaria TOT For Doctors 2022 District Dengue PPTDocument88 pagesDengue-Malaria TOT For Doctors 2022 District Dengue PPTRanjeet SinghNo ratings yet
- Global Vector Control Response 2017-2030: Fourth Draft (Version 4.3)Document50 pagesGlobal Vector Control Response 2017-2030: Fourth Draft (Version 4.3)Febby WadoeNo ratings yet
- Viral Hemorrhagic Fever Surveillance Protocol: Provider ResponsibilitiesDocument32 pagesViral Hemorrhagic Fever Surveillance Protocol: Provider ResponsibilitiesAmadi OgbondaNo ratings yet
- The History and Natural History of Dengue FeverDocument2 pagesThe History and Natural History of Dengue Feverchiquilon749100% (1)
- Reading ComprehensionDocument4 pagesReading ComprehensionSanisha ChandrasagamNo ratings yet
- Numerical Methods in Real LifeDocument4 pagesNumerical Methods in Real LifeArjay Mandigma AbacanNo ratings yet
- Introduction (1-60)Document61 pagesIntroduction (1-60)Arjay RoselNo ratings yet
- National Guidelines On Clinical Management of Dengue Infection in Pregnancy Reprint Version - New PDFDocument78 pagesNational Guidelines On Clinical Management of Dengue Infection in Pregnancy Reprint Version - New PDFsarakg vathNo ratings yet
- Monthly Report On Dengue Entomological Surveillance Vol. 01 :issue 02Document2 pagesMonthly Report On Dengue Entomological Surveillance Vol. 01 :issue 02National Dengue Control Unit,Sri LankaNo ratings yet
- APPA Bulletin 85-7-2022Document12 pagesAPPA Bulletin 85-7-2022yanoodNo ratings yet
- Class Xi WritingDocument32 pagesClass Xi Writingjaymaity3333% (3)
- MANUSCRIPTDocument37 pagesMANUSCRIPTAngeline ShackletonNo ratings yet
- Search Results For: Dengue: FeverDocument18 pagesSearch Results For: Dengue: FeverlakshmibavaNo ratings yet
- DR. NOEL CASUMPANG vs. CORTEJO G.R. No. 171127, March 11, 2015Document21 pagesDR. NOEL CASUMPANG vs. CORTEJO G.R. No. 171127, March 11, 2015FD BalitaNo ratings yet
- Read The Short Story Below and Answer The Questions That FollowDocument13 pagesRead The Short Story Below and Answer The Questions That FollowRaqueliza Molina VillapaNo ratings yet