You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Orthopedic Surgery Clerkship A Quick Reference Guide For Senior Medical StudentsDocument750 pagesOrthopedic Surgery Clerkship A Quick Reference Guide For Senior Medical StudentsGreenIron9100% (1)
- 7th Edition NRP Update FinalDocument18 pages7th Edition NRP Update FinaliamlucilNo ratings yet
- Smoking - Effects On Your Body - Better Health ChannelDocument7 pagesSmoking - Effects On Your Body - Better Health ChannelUmair MalikNo ratings yet
- Pediatric PolysomnographyDocument7 pagesPediatric Polysomnographysavvy_as_98-1No ratings yet
- Neonatal Sepsis: A Study of The Risk FactorsDocument42 pagesNeonatal Sepsis: A Study of The Risk FactorsNithin100% (3)
- Assessment and Management of Patients With Hematologic DisordersDocument20 pagesAssessment and Management of Patients With Hematologic DisordersJhosita Flora LarocoNo ratings yet
- Study Guide For The Psychiatry NBME Content Exam AKA The Psychiatry Shelf Exam!Document2 pagesStudy Guide For The Psychiatry NBME Content Exam AKA The Psychiatry Shelf Exam!DoriNo ratings yet
- PMS and MassageDocument6 pagesPMS and MassageSiva Shanmugam100% (1)
- Crohn's DiseaseDocument1 pageCrohn's DiseaseibrahimNo ratings yet
- Ambulatory Care 2Document5 pagesAmbulatory Care 2api-273330093No ratings yet
- Revalida QuestionsDocument6 pagesRevalida QuestionsCarolyn Calupitan100% (1)
- Chapter 2 ImmunologyDocument38 pagesChapter 2 ImmunologyBryan JanierNo ratings yet
- Telerehab in Covid and CopdDocument13 pagesTelerehab in Covid and CopdNelson LoboNo ratings yet
- Cardiovascular Disease NCPDocument5 pagesCardiovascular Disease NCPShyla ManguiatNo ratings yet
- Kleinman 2011Document9 pagesKleinman 2011rsthsn6z8xNo ratings yet
- Pediatric Surgery: Diagnosis and Management Prem Puri Michael E. HöllwarthDocument1,479 pagesPediatric Surgery: Diagnosis and Management Prem Puri Michael E. Höllwarthjuao100% (1)
- Nursing Health Assessment Exam 2Document45 pagesNursing Health Assessment Exam 2Jennifer Jaworsky100% (3)
- Seminar: Jonathan Posner, Guilherme V Polanczyk, Edmund Sonuga-BarkeDocument13 pagesSeminar: Jonathan Posner, Guilherme V Polanczyk, Edmund Sonuga-BarkeCristinaNo ratings yet
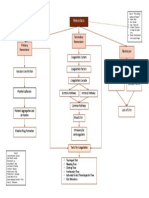
- B4M1 Case 2 My Concept MapDocument1 pageB4M1 Case 2 My Concept MapMabuhigh ErnieNo ratings yet
- NARPAA E-Class Module 3 - Historical Definitions of AutismDocument19 pagesNARPAA E-Class Module 3 - Historical Definitions of AutismnarpaaNo ratings yet
- 01 Pediatrics in Review - January2010Document69 pages01 Pediatrics in Review - January2010Madhaw BajajNo ratings yet
- Woc ArdsDocument2 pagesWoc Ardssyarifah salmaNo ratings yet
- Stress ManagementDocument19 pagesStress ManagementAnand DubeyNo ratings yet
- Hematology Sop (Revise 2023)Document8 pagesHematology Sop (Revise 2023)Jeffrey GaliciaNo ratings yet
- Practice ExamDocument25 pagesPractice ExamNimra NazeerNo ratings yet
- Joni Jane Asignacion Wianne Mae Balatongle: Preterm BirthsDocument2 pagesJoni Jane Asignacion Wianne Mae Balatongle: Preterm BirthsMary Ann Pastolero BalatongleNo ratings yet
- Pre-Operative AssessmentDocument33 pagesPre-Operative AssessmentKartika FitriNo ratings yet
- Assessment Is Making Assumptions. When You See It, You Attach It ToDocument18 pagesAssessment Is Making Assumptions. When You See It, You Attach It ToDonn Patrick AlegreNo ratings yet
- Tongue DisordersDocument10 pagesTongue DisordersMohan VeerabomalaNo ratings yet
- Kode Diagnosa Icd 10Document5 pagesKode Diagnosa Icd 10Heri SetiawanNo ratings yet