You might also like
- Employment Application Form 09Document3 pagesEmployment Application Form 09api-19987040No ratings yet
- Environmental+Management+Employment+ApplicationDocument4 pagesEnvironmental+Management+Employment+Applicationsheladiyachintan13No ratings yet
- GAL Application - Become A GAL in SCDocument5 pagesGAL Application - Become A GAL in SCWylde FaerieNo ratings yet
- Application For Employment For Office Use OnlyDocument9 pagesApplication For Employment For Office Use OnlyMr. PicklesNo ratings yet
- Application For EmploymentDocument2 pagesApplication For EmploymentChuck SlaughterNo ratings yet
- Personnel Information Sheet (New)Document5 pagesPersonnel Information Sheet (New)Lyra ValdezNo ratings yet
- 124 W. Michigan Ave, 6 Floor City Hall, Lansing, MI 48933: 54-A District Court Employment ApplicationDocument4 pages124 W. Michigan Ave, 6 Floor City Hall, Lansing, MI 48933: 54-A District Court Employment ApplicationcdmbNo ratings yet
- Lincoln-Woodstock Cooperative School District SAU # 68Document4 pagesLincoln-Woodstock Cooperative School District SAU # 68Daniel AdamsNo ratings yet
- Plex App Form 2022Document4 pagesPlex App Form 2022wjdhnpj4ndNo ratings yet
- Personnel Information Sheet (New) PDFDocument5 pagesPersonnel Information Sheet (New) PDFLoo PeaNo ratings yet
- 1 Basic Information SheetDocument2 pages1 Basic Information SheetCyndy Loraine SilvestreNo ratings yet
- HVL ApplicationDocument3 pagesHVL Application56hrsw2qb8No ratings yet
- Work Experience Certification For Journeyman PlumberDocument2 pagesWork Experience Certification For Journeyman Plumberabood30513No ratings yet
- Application Form TitleDocument4 pagesApplication Form TitleSaarthak SangamnerkarNo ratings yet
- Enrollment AppDocument10 pagesEnrollment Appapi-218391675No ratings yet
- PDF Staff Application07 2018Document3 pagesPDF Staff Application07 2018HummNo ratings yet
- Johnny Q - Employment Application FormDocument3 pagesJohnny Q - Employment Application Formprettyboiricky54No ratings yet
- Internship Application FormDocument2 pagesInternship Application FormRichelle ManocayNo ratings yet
- Tenant ApplicationDocument2 pagesTenant ApplicationHoggz PhotographyNo ratings yet
- Employee Data Sheet FormDocument1 pageEmployee Data Sheet Formmark santosNo ratings yet
- Application For Program EntryDocument6 pagesApplication For Program EntryAngela FrizellNo ratings yet
- Senior Brag Sheet PDFDocument3 pagesSenior Brag Sheet PDFVũ Thanh An NguyễnNo ratings yet
- Target Job Application Form PrintableDocument5 pagesTarget Job Application Form PrintableDom HilliardNo ratings yet
- Applicant Application FormDocument6 pagesApplicant Application FormJocelyn Joy ArcegaNo ratings yet
- BDB Job Application Form PDFDocument4 pagesBDB Job Application Form PDFpema dekiNo ratings yet
- Dube Trade Port Application FormDocument7 pagesDube Trade Port Application FormNcediswaNo ratings yet
- Application For RentalDocument3 pagesApplication For RentalreenywNo ratings yet
- Police Verification FormDocument2 pagesPolice Verification Formshaikhfaisal100% (1)
- MCK FormDocument3 pagesMCK FormMauro CesarNo ratings yet
- Detailed Application Form: Roll NoDocument4 pagesDetailed Application Form: Roll NoRAVALI BNo ratings yet
- Candidate Application Form V2 23 June 2015 Neo EltariDocument4 pagesCandidate Application Form V2 23 June 2015 Neo Eltarianita nahakNo ratings yet
- Re Admission FormDocument2 pagesRe Admission FormMissy SamanthaNo ratings yet
- EmploymentApp 2018-03-01 Walk UpDocument2 pagesEmploymentApp 2018-03-01 Walk UpKOLD News 13No ratings yet
- Appplication FormDocument8 pagesAppplication FormDannaRoseGonzalesNo ratings yet
- FEBC Info Sheet - NEWDocument5 pagesFEBC Info Sheet - NEWnigel alinsug0% (1)
- Employment Application FormDocument5 pagesEmployment Application FormRJ Crafty InkNo ratings yet
- Undergraduate Application Form-23022022Document2 pagesUndergraduate Application Form-23022022bongisebodgeNo ratings yet
- Employment Application for Office AdministratorDocument5 pagesEmployment Application for Office AdministratorVivian StanleyNo ratings yet
- Employment Application PDFDocument4 pagesEmployment Application PDFWhy MooreNo ratings yet
- UP College of Medicine Application GuideDocument5 pagesUP College of Medicine Application GuideHenrietta QuillaNo ratings yet
- Completete SET OF HR FORMSDocument9 pagesCompletete SET OF HR FORMSALEXANDER DIMAFELIX JR.No ratings yet
- Empapp 2016 BDocument5 pagesEmpapp 2016 Bapi-393899350No ratings yet
- Mps Retail PVT LTD.: Personal DetailsDocument4 pagesMps Retail PVT LTD.: Personal DetailsSelvarajNo ratings yet
- Clinical Health RequirementsDocument6 pagesClinical Health RequirementsbarneylovesbagelsNo ratings yet
- Senior Brag SheetDocument3 pagesSenior Brag Sheetapi-307211076No ratings yet
- Employment Job ApplicationDocument4 pagesEmployment Job Applicationapi-294681692No ratings yet
- Internship Application Form - BlankDocument3 pagesInternship Application Form - BlankDap DapNo ratings yet
- Initial Questionnaire - Family Law Case in ProgressDocument7 pagesInitial Questionnaire - Family Law Case in ProgressAndros MaldanerNo ratings yet
- Berlin Deutsche Energy Ag - Interview FormDocument7 pagesBerlin Deutsche Energy Ag - Interview FormcristinaNo ratings yet
- 02.joining Report FormatDocument13 pages02.joining Report FormatAnonymous g7uPednINo ratings yet
- Info SheetDocument7 pagesInfo SheetALJON DONGALLONo ratings yet
- HR Services Request For QuoteDocument5 pagesHR Services Request For QuoteSandeep MisraNo ratings yet
- Monessen Application For Employment DraftDocument5 pagesMonessen Application For Employment DraftWilmer A Mosquera FigueroaNo ratings yet
- HR - Personal History StatementDocument4 pagesHR - Personal History StatementCherry AldayNo ratings yet
- Application Form School of GovernmentDocument3 pagesApplication Form School of GovernmentRobert RoblesNo ratings yet
- 15 Exercises On Resume WritingDocument38 pages15 Exercises On Resume Writingangeline salongaNo ratings yet
- 3 Employment Application FormDocument3 pages3 Employment Application FormDiemquynhdangNo ratings yet
- Will QuestionnaireDocument16 pagesWill Questionnaireneha.banNo ratings yet
- Call For Application For The Mexican Government Scholarship Program For Foreigners 2011Document7 pagesCall For Application For The Mexican Government Scholarship Program For Foreigners 2011syedmohammadsamarNo ratings yet
- PastLifeTherapy Weiss 2005-03-12Document29 pagesPastLifeTherapy Weiss 2005-03-12Fazal HaqueNo ratings yet
- Certain VictoryDocument460 pagesCertain VictoryFazal Haque100% (1)
- Edgar Cayce, The Children of The Law of One and The Lost Teachings of AtlantisDocument396 pagesEdgar Cayce, The Children of The Law of One and The Lost Teachings of AtlantisTezza1396% (70)
- 03 ZimmermanDocument9 pages03 ZimmermanFazal HaqueNo ratings yet
- Ehli Daimonion 2017Document17 pagesEhli Daimonion 2017Vojtěch HladkýNo ratings yet
- Unit 3Document11 pagesUnit 3banaz.aliNo ratings yet
- Graham & Doddsville - Issue 20 - Winter 2014 - FinalDocument68 pagesGraham & Doddsville - Issue 20 - Winter 2014 - Finalbpd3kNo ratings yet
- Carmelita DivinagraciaDocument9 pagesCarmelita DivinagraciaLynn Florence LazaroNo ratings yet
- DepEdClub Math Lesson Plan for Teaching DecimalsDocument4 pagesDepEdClub Math Lesson Plan for Teaching DecimalsBimbo Cuyangoan100% (1)
- Teen MarriageDocument23 pagesTeen MarriageDeneshwaran Balarajan0% (1)
- MY FINAL DEMO & For ApplicationDocument6 pagesMY FINAL DEMO & For ApplicationRica Mae AnciadoNo ratings yet
- Vampire The Requiem - SAS - Scenes of FrenzyDocument16 pagesVampire The Requiem - SAS - Scenes of FrenzyCaio César100% (1)
- Maintenance Stationary EngineerDocument3 pagesMaintenance Stationary EngineerShams TabrezNo ratings yet
- Roles of A System AnalystDocument17 pagesRoles of A System AnalystMohan William SharmaNo ratings yet
- Chapter 3 HRDocument47 pagesChapter 3 HRAnonymous s98FwgOYCNo ratings yet
- Grade 10 ICT Lesson on Photoshop Image EnhancementDocument2 pagesGrade 10 ICT Lesson on Photoshop Image EnhancementEarl Vestidas CapurasNo ratings yet
- Nursing Student Helps Patient Open UpDocument5 pagesNursing Student Helps Patient Open UpNica SalazarNo ratings yet
- Research ProposalDocument5 pagesResearch ProposalLueween Acay CansinoNo ratings yet
- Shadow and Solitude: A play by Claro M. Recto about gossip and social conventionsDocument34 pagesShadow and Solitude: A play by Claro M. Recto about gossip and social conventionsharrohhoraytNo ratings yet
- Unit Topic: Data Interpretation & Graphing Grade Level: 8 Stage 1 - Desired Results Content Standard/Established Goals(s)Document4 pagesUnit Topic: Data Interpretation & Graphing Grade Level: 8 Stage 1 - Desired Results Content Standard/Established Goals(s)VartyYeremianNo ratings yet
- Good Knight Slide ShowDocument39 pagesGood Knight Slide ShowPradipKhatuaNo ratings yet
- Andrew J. Mitchell and Peter Trawny (Eds.) - Heidegger's Black Notebooks - Responses To Anti-Semitism-Columbia University Press (2017) PDFDocument275 pagesAndrew J. Mitchell and Peter Trawny (Eds.) - Heidegger's Black Notebooks - Responses To Anti-Semitism-Columbia University Press (2017) PDFfernapoNo ratings yet
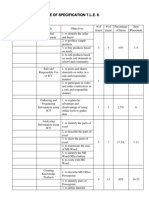
- Table of Specification T.L.E. 6Document3 pagesTable of Specification T.L.E. 6Autumn Thorn SebastianNo ratings yet
- Lit17 Ev g11 U4 Awc ST Twa2 Ak CADocument3 pagesLit17 Ev g11 U4 Awc ST Twa2 Ak CAbebepic355No ratings yet
- Art as an Expression in 40 CharactersDocument14 pagesArt as an Expression in 40 CharactersBernadette FernandezNo ratings yet
- Process Plant Design II Rubric For Presentation 1Document5 pagesProcess Plant Design II Rubric For Presentation 1Nazurul Ezzati100% (1)
- Reflection Paper On DancingDocument2 pagesReflection Paper On DancingJohn Paul S. DucusinNo ratings yet
- 21st Century Skills Map: Designed in Cooperation With The Nation'S World Language Educ AtorsDocument21 pages21st Century Skills Map: Designed in Cooperation With The Nation'S World Language Educ Atorscasalim_34No ratings yet
- Resources For Mental HealthDocument3 pagesResources For Mental HealthDhriti AgarwalNo ratings yet
- Outcomes of DemocracyDocument2 pagesOutcomes of DemocracyaishuunniNo ratings yet
- Wmels Guiding PrinciplesDocument10 pagesWmels Guiding Principlesapi-267528958No ratings yet
- Types of Hostage TakersDocument5 pagesTypes of Hostage Takersjanine aquebayNo ratings yet
- MS Project 2010 Training Presnetation For BeginersDocument21 pagesMS Project 2010 Training Presnetation For BeginersRasool ShaikNo ratings yet
- Curriculum Design Principles for Effective Teaching and LearningDocument5 pagesCurriculum Design Principles for Effective Teaching and LearningPatrick kenneth GacayanNo ratings yet
- Not a Crime to Be Poor: The Criminalization of Poverty in AmericaFrom EverandNot a Crime to Be Poor: The Criminalization of Poverty in AmericaRating: 4.5 out of 5 stars4.5/5 (37)
- High-Risers: Cabrini-Green and the Fate of American Public HousingFrom EverandHigh-Risers: Cabrini-Green and the Fate of American Public HousingNo ratings yet
- Workin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherFrom EverandWorkin' Our Way Home: The Incredible True Story of a Homeless Ex-Con and a Grieving Millionaire Thrown Together to Save Each OtherNo ratings yet
- Poor Economics: A Radical Rethinking of the Way to Fight Global PovertyFrom EverandPoor Economics: A Radical Rethinking of the Way to Fight Global PovertyRating: 4.5 out of 5 stars4.5/5 (263)
- Fucked at Birth: Recalibrating the American Dream for the 2020sFrom EverandFucked at Birth: Recalibrating the American Dream for the 2020sRating: 4 out of 5 stars4/5 (173)
- Nickel and Dimed: On (Not) Getting By in AmericaFrom EverandNickel and Dimed: On (Not) Getting By in AmericaRating: 4 out of 5 stars4/5 (186)
- When Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfFrom EverandWhen Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfRating: 5 out of 5 stars5/5 (36)
- The Meth Lunches: Food and Longing in an American CityFrom EverandThe Meth Lunches: Food and Longing in an American CityRating: 5 out of 5 stars5/5 (5)
- Same Kind of Different As Me Movie Edition: A Modern-Day Slave, an International Art Dealer, and the Unlikely Woman Who Bound Them TogetherFrom EverandSame Kind of Different As Me Movie Edition: A Modern-Day Slave, an International Art Dealer, and the Unlikely Woman Who Bound Them TogetherRating: 4 out of 5 stars4/5 (685)
- Heartland: A Memoir of Working Hard and Being Broke in the Richest Country on EarthFrom EverandHeartland: A Memoir of Working Hard and Being Broke in the Richest Country on EarthRating: 4 out of 5 stars4/5 (188)
- Hillbilly Elegy: A Memoir of a Family and Culture in CrisisFrom EverandHillbilly Elegy: A Memoir of a Family and Culture in CrisisRating: 4 out of 5 stars4/5 (4277)
- The Great Displacement: Climate Change and the Next American MigrationFrom EverandThe Great Displacement: Climate Change and the Next American MigrationRating: 4 out of 5 stars4/5 (19)
- Skimmed: Breastfeeding, Race, and InjusticeFrom EverandSkimmed: Breastfeeding, Race, and InjusticeRating: 5 out of 5 stars5/5 (1)
- The Great Displacement: Climate Change and the Next American MigrationFrom EverandThe Great Displacement: Climate Change and the Next American MigrationRating: 4.5 out of 5 stars4.5/5 (32)
- The Mole People: Life in the Tunnels Beneath New York CityFrom EverandThe Mole People: Life in the Tunnels Beneath New York CityRating: 3.5 out of 5 stars3.5/5 (190)
- Who Really Owns Ireland: How we became tenants in our own land - and what we can do about itFrom EverandWho Really Owns Ireland: How we became tenants in our own land - and what we can do about itNo ratings yet
- When Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfFrom EverandWhen Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfRating: 4 out of 5 stars4/5 (126)
- Charity Detox: What Charity Would Look Like If We Cared About ResultsFrom EverandCharity Detox: What Charity Would Look Like If We Cared About ResultsRating: 4 out of 5 stars4/5 (9)
- This Is Ohio: The Overdose Crisis and the Front Lines of a New AmericaFrom EverandThis Is Ohio: The Overdose Crisis and the Front Lines of a New AmericaRating: 4 out of 5 stars4/5 (37)
- Alienated America: Why Some Places Thrive While Others CollapseFrom EverandAlienated America: Why Some Places Thrive While Others CollapseRating: 4 out of 5 stars4/5 (35)
- Nickel and Dimed: On (Not) Getting By in AmericaFrom EverandNickel and Dimed: On (Not) Getting By in AmericaRating: 3.5 out of 5 stars3.5/5 (197)
- Heartland: A Memoir of Working Hard and Being Broke in the Richest Country on EarthFrom EverandHeartland: A Memoir of Working Hard and Being Broke in the Richest Country on EarthRating: 4 out of 5 stars4/5 (269)
- Superclass: The Global Power Elite and the World They Are MakingFrom EverandSuperclass: The Global Power Elite and the World They Are MakingRating: 3.5 out of 5 stars3.5/5 (32)