You might also like
- ADAClaim FormDocument2 pagesADAClaim FormMcnet WideNo ratings yet
- Assigned by Plan Named in #3Document2 pagesAssigned by Plan Named in #3olimaziNo ratings yet
- Jurnal Rekam Medik 3Document2 pagesJurnal Rekam Medik 3Fitri AngginiNo ratings yet
- Dental Claim FormDocument2 pagesDental Claim Formmiranda criggerNo ratings yet
- EXC-MBR-MDM-EMP-BKR-Dental Claim FormDocument2 pagesEXC-MBR-MDM-EMP-BKR-Dental Claim Formnicholas beehnerNo ratings yet
- SBS Res Broker DentalClaimFormDocument2 pagesSBS Res Broker DentalClaimFormNarendra SubramanyaNo ratings yet
- Member Dental Claim Form: Mark All Applicable Boxes)Document4 pagesMember Dental Claim Form: Mark All Applicable Boxes)TreyNo ratings yet
- PA Covid EruwanDocument2 pagesPA Covid EruwanAhmad EruwanNo ratings yet
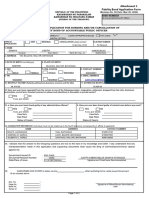
- Fidelity Bond Application Form BT2024Document2 pagesFidelity Bond Application Form BT2024jomarNo ratings yet
- Max Life Insurance Company Limited: Proposal NumberDocument5 pagesMax Life Insurance Company Limited: Proposal NumberArjun TyagiNo ratings yet
- cms1500 FormDocument2 pagescms1500 FormpalashNo ratings yet
- Financial Amendment Form: 1 General InformationDocument3 pagesFinancial Amendment Form: 1 General InformationRandolph QuilingNo ratings yet
- ONLINE-FORM-MAPFRE Travel International Application-ROSALESDocument2 pagesONLINE-FORM-MAPFRE Travel International Application-ROSALESkimdodok123No ratings yet
- Provider Data Record Health Care Professional: The President & CeoDocument1 pageProvider Data Record Health Care Professional: The President & CeojayinthelongrunNo ratings yet
- Advisor Change RequestDocument2 pagesAdvisor Change RequestJuan IsaacNo ratings yet
- Beneficiary Change Request: Purpose of The Form: Important NotesDocument4 pagesBeneficiary Change Request: Purpose of The Form: Important NotesRonald Garcia PreNo ratings yet
- ProposalForm 501434778Document14 pagesProposalForm 501434778rahul naveenNo ratings yet
- MediCard Standard Plan FormDocument31 pagesMediCard Standard Plan FormCheskaPink TemonesNo ratings yet
- Konsulta - ProviderDataRecord 2Document1 pageKonsulta - ProviderDataRecord 2Orlando PalomponNo ratings yet
- SLOCPI Address and Contact Information - Fill and SignDocument2 pagesSLOCPI Address and Contact Information - Fill and SignMichelle VillocogNo ratings yet
- NJ State Health Benefits Program (SHBP)Document2 pagesNJ State Health Benefits Program (SHBP)Sarah GomezNo ratings yet
- Form VBA 21-2680 AREDocument4 pagesForm VBA 21-2680 AREJane DoeNo ratings yet
- Fidelity Bond Application Form FBAFDocument2 pagesFidelity Bond Application Form FBAFREYES-DEVILLA LAW OFFICENo ratings yet
- KYC For Beneficial Owner and Third Party PayorDocument2 pagesKYC For Beneficial Owner and Third Party PayorQIANo ratings yet
- KYC For Beneficial Owner and Third Party PayorDocument2 pagesKYC For Beneficial Owner and Third Party PayorCarolie BacatanoNo ratings yet
- Beneficial Owner FormDocument1 pageBeneficial Owner FormrichlogNo ratings yet
- Companies Form 59Document3 pagesCompanies Form 59peter kachamaNo ratings yet
- Customer Information Sheet and DPC With Terms and Conditions - Individual - v2020Document8 pagesCustomer Information Sheet and DPC With Terms and Conditions - Individual - v2020jason geronaNo ratings yet
- Customer Information Form IndividualDocument2 pagesCustomer Information Form IndividualCiel AnnNo ratings yet
- Standard Insurance Company: Attending Dentist's Statement Treatment Plan and Insurance Claim ReportDocument2 pagesStandard Insurance Company: Attending Dentist's Statement Treatment Plan and Insurance Claim ReportAfzal ImamNo ratings yet
- Repagreement Comp PDFDocument2 pagesRepagreement Comp PDFLucian Ștefan BusnăNo ratings yet
- Dengue CRF - FillableDocument3 pagesDengue CRF - FillableRosario Dalida100% (1)
- Max Life Insurance Company Limited: Proposal NumberDocument9 pagesMax Life Insurance Company Limited: Proposal NumberAbhilasha JainNo ratings yet
- Confidential Info Sheet DBP LOAN FORMDocument2 pagesConfidential Info Sheet DBP LOAN FORMKeneth Samson Del Carmen100% (1)
- Life Insurance Beneficiary Designation Form - GeneraliDocument2 pagesLife Insurance Beneficiary Designation Form - Generalijohn gerald reynoNo ratings yet
- VA Form 21-4138Document2 pagesVA Form 21-4138carmenNo ratings yet
- Simplified Group Application FormDocument1 pageSimplified Group Application FormJammie Rize GautaneNo ratings yet
- Muthoot 1Document1 pageMuthoot 1Sanjeev Bisht-CrayontekNo ratings yet
- 2024 Medicard IF Application FormDocument2 pages2024 Medicard IF Application FormAlyzza EscalanteNo ratings yet
- Dental Expense Claim: SECTION 1: To Be Completed by EmployeeDocument6 pagesDental Expense Claim: SECTION 1: To Be Completed by EmployeeandryNo ratings yet
- SLF065 MultiPurposeLoanApplicationForm V03Document2 pagesSLF065 MultiPurposeLoanApplicationForm V03Belle Adante100% (1)
- Sunita Sharma: Application Form (For Resident Applicants) Asba Application FormDocument1 pageSunita Sharma: Application Form (For Resident Applicants) Asba Application Formitsyour vinESNo ratings yet
- Guideline On How To Fill Out The Customer Signature Card - ShopeeDocument2 pagesGuideline On How To Fill Out The Customer Signature Card - ShopeeCharisse Hope RadazaNo ratings yet
- UB Form - DJSDocument3 pagesUB Form - DJSD Delos SalNo ratings yet
- Vba 21 2680 AreDocument3 pagesVba 21 2680 AreAhmad Gamal Elden MAhanyNo ratings yet
- Ariel Padaca EpsDocument2 pagesAriel Padaca Epsariel padacaNo ratings yet
- Application Form Revision 9 July 3 2017Document2 pagesApplication Form Revision 9 July 3 2017OrlanNo ratings yet
- PagIBIG Loan FormDocument2 pagesPagIBIG Loan FormgdlveeplNo ratings yet
- Annex H Summary List of Beneficiaries Version 3Document4 pagesAnnex H Summary List of Beneficiaries Version 3Glenda Osia-DiazNo ratings yet
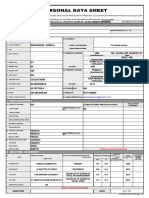
- PDS Nyka DS NewDocument7 pagesPDS Nyka DS NewReina Noreen IgnacioNo ratings yet
- Calamity Loan Application Form: Filipino FilipinoDocument2 pagesCalamity Loan Application Form: Filipino Filipinoaljhondelacruz22No ratings yet
- Relationship Maintenace FormDocument1 pageRelationship Maintenace FormArnel Albarando33% (3)
- Customer Information FormDocument4 pagesCustomer Information FormRobert MacalanaoNo ratings yet
- Application For MRI - SRI ClaimDocument2 pagesApplication For MRI - SRI ClaimivyNo ratings yet
- Cir 200457281200Document4 pagesCir 200457281200Robert MacalanaoNo ratings yet
- I10 FormDocument1 pageI10 Formleomal320% (1)
- Thrift Savings Plan: Form TSP-3 Designation of BeneficiaryDocument8 pagesThrift Savings Plan: Form TSP-3 Designation of BeneficiaryMarsha MainesNo ratings yet
- Horizon Medical Health Insurance Claim Form: Please Read This Important InformationDocument2 pagesHorizon Medical Health Insurance Claim Form: Please Read This Important InformationBrianReagerNo ratings yet
- The Telephone Answering Service Industry: Preparing for the FutureFrom EverandThe Telephone Answering Service Industry: Preparing for the FutureNo ratings yet
- Principles and Practice of Single Implant and Restoration - Saunders 1 Edition (March 26, 2013)Document204 pagesPrinciples and Practice of Single Implant and Restoration - Saunders 1 Edition (March 26, 2013)Sergiu Pinte100% (1)
- Jagiellonian University in KrakówDocument18 pagesJagiellonian University in KrakówCarlos EsquivelNo ratings yet
- Enamel and Dentin BondingDocument9 pagesEnamel and Dentin Bondinghelmuthw0207No ratings yet
- July 8Document48 pagesJuly 8fijitimescanadaNo ratings yet
- Khyber Pakhtunkhwa Public Service Commission: Dvertisement ODocument16 pagesKhyber Pakhtunkhwa Public Service Commission: Dvertisement OFaizan KhiljNo ratings yet
- Fee Structure 2023 24Document6 pagesFee Structure 2023 24Vasu SharmaNo ratings yet
- Sno Rank App - No Name Community T.Mark AllottedDocument39 pagesSno Rank App - No Name Community T.Mark AllottedSuriya SamNo ratings yet
- Oral Pathology For The Dental Hygienist e Book 7th Edition Ebook PDFDocument61 pagesOral Pathology For The Dental Hygienist e Book 7th Edition Ebook PDFdoris.heck867100% (33)
- Admission Reuglations 2020 For MBBS and BDSDocument16 pagesAdmission Reuglations 2020 For MBBS and BDSaayedNo ratings yet
- Career Path Exploration GridDocument2 pagesCareer Path Exploration Gridapi-490808450No ratings yet
- Ra 9484 Original Document SignedDocument17 pagesRa 9484 Original Document SignedStudy PlaceNo ratings yet
- Mosby's Dental Drug ReferenceDocument3 pagesMosby's Dental Drug ReferenceNada Gaafer Abdelrahim0% (1)
- Dental List PDFDocument84 pagesDental List PDFDeck Magana100% (1)
- Ing. Serag M. A Comparative Study of The Accuracy of Dies Made From Digital IntraDocument6 pagesIng. Serag M. A Comparative Study of The Accuracy of Dies Made From Digital IntraBavilonia K PaolaNo ratings yet
- Pgimer MD Ms ProspectusDocument28 pagesPgimer MD Ms ProspectusJonathan FergusonNo ratings yet
- Government Government of Tamil Nadu: Cost 500/ 500Document99 pagesGovernment Government of Tamil Nadu: Cost 500/ 500JackNo ratings yet
- HPU/Exams-III/BDS. 2nd (Annual) /2021: NAAC Accredited 'A' Grade UniversityDocument13 pagesHPU/Exams-III/BDS. 2nd (Annual) /2021: NAAC Accredited 'A' Grade UniversitySneha SinghNo ratings yet
- ResumeDocument1 pageResumeLaura GoviNo ratings yet
- Comedk Pget-2007 BrochureDocument30 pagesComedk Pget-2007 Brochuremahesh100% (3)
- A Concise Textbook of Oral and Maxillofacial SurgeryDocument304 pagesA Concise Textbook of Oral and Maxillofacial SurgeryDodo AlvaNo ratings yet
- Chaturvedi: Doctors' Directory 2017Document125 pagesChaturvedi: Doctors' Directory 2017dhananjay71% (7)
- Essentials of Oral MedicineDocument389 pagesEssentials of Oral MedicineKishendran R GanandranNo ratings yet
- Mqpgprospectus2020-21 0 0Document26 pagesMqpgprospectus2020-21 0 0Sai Krishna SeethamrajuNo ratings yet
- The History of Articulators - A Perspective On The Early Years, Part 1Document3 pagesThe History of Articulators - A Perspective On The Early Years, Part 1Mário FerreiraNo ratings yet
- NTR University Mbbs-Bds Admisssions Regulations 2011Document28 pagesNTR University Mbbs-Bds Admisssions Regulations 2011Narasimha SastryNo ratings yet
- Preview of The Dental Pulp Biology Pathology and Regenerative TherapiesDocument12 pagesPreview of The Dental Pulp Biology Pathology and Regenerative TherapiesMuchlis fauziNo ratings yet
- CPMEE 2016 ProspectusDocument20 pagesCPMEE 2016 ProspectusMota ChashmaNo ratings yet
- DR Data GhaziabadDocument36 pagesDR Data Ghaziabadprateek gangwaniNo ratings yet
- 2011 Diagnosis and Treatment in ProsthodonticsDocument353 pages2011 Diagnosis and Treatment in ProsthodonticsAnonymous 0pg1qSpO100% (1)
- FrontiersDocument10 pagesFrontiersghanimNo ratings yet