0% found this document useful (0 votes)
41 views4 pagesType 2 Diabetes Case Study Analysis
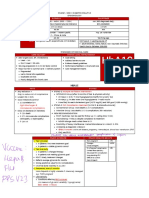
The document details the medical findings and assessment of a 45-year-old female patient diagnosed with type 2 diabetes. Key findings include elevated blood sugar and A1C levels, as well as risk factors like family history, smoking, lack of exercise and poor diet. The resolution outlines treatment and lifestyle changes recommended, including medication, diet modification, exercise and smoking cessation.
Uploaded by
19100424Copyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
41 views4 pagesType 2 Diabetes Case Study Analysis
The document details the medical findings and assessment of a 45-year-old female patient diagnosed with type 2 diabetes. Key findings include elevated blood sugar and A1C levels, as well as risk factors like family history, smoking, lack of exercise and poor diet. The resolution outlines treatment and lifestyle changes recommended, including medication, diet modification, exercise and smoking cessation.
Uploaded by
19100424Copyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd