You might also like
- Tatalakasana Diabetes - Intoduce InsulinDocument53 pagesTatalakasana Diabetes - Intoduce InsulinChristina XavierNo ratings yet
- Guideline Perkeni 2019 PDFDocument36 pagesGuideline Perkeni 2019 PDFCut Aulia MaulizaNo ratings yet
- Guideline Perkeni 2019 - 4Document36 pagesGuideline Perkeni 2019 - 4jktrlsNo ratings yet
- Slide Deck RTD Pre Diabetes - FinalDocument39 pagesSlide Deck RTD Pre Diabetes - FinalVieca FauziahNo ratings yet
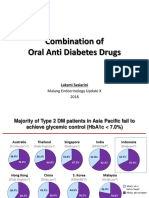
- Combination of Oads - Edit PDFDocument45 pagesCombination of Oads - Edit PDFrent3010No ratings yet
- Update Diagnosis Dan Manajemen DM Tipe 2 Perkeni 2019 - Dr. Kurniawan Agung YuwonoDocument39 pagesUpdate Diagnosis Dan Manajemen DM Tipe 2 Perkeni 2019 - Dr. Kurniawan Agung YuwonoLaura CintyaNo ratings yet
- Early Insulin Initiation in Type 2 DM Management: DR - Yosef S.Sugi, SPPDDocument36 pagesEarly Insulin Initiation in Type 2 DM Management: DR - Yosef S.Sugi, SPPDyosefsugiNo ratings yet
- 3rd Session - Management of Hyperglycemic Crisis - DR Lukman Hatta SPPDDocument24 pages3rd Session - Management of Hyperglycemic Crisis - DR Lukman Hatta SPPDAndhika WicaksanaNo ratings yet
- RTD Levemir®Document54 pagesRTD Levemir®rizkiNo ratings yet
- Short Article DiabetesDocument6 pagesShort Article DiabetesIGusti Putu Suka AryanaNo ratings yet
- Prediabetes - OKE - IDI LMGNDocument48 pagesPrediabetes - OKE - IDI LMGNruthmindosiahaanNo ratings yet
- Materi Diabetes Mellitus - WAHYUDocument29 pagesMateri Diabetes Mellitus - WAHYUAli Sibra MulluziNo ratings yet
- RTD Levemir v1 2018Document38 pagesRTD Levemir v1 2018Risma SaroyaNo ratings yet
- Diabetes Melitus: Makbul M AmanDocument69 pagesDiabetes Melitus: Makbul M AmanDwi YantiNo ratings yet
- SuastikaDocument10 pagesSuastikaDeedee RenovaldiNo ratings yet
- XXXXDocument40 pagesXXXXsundance127No ratings yet
- Diabetes Melitus & Sindroma Metabolik PITDocument48 pagesDiabetes Melitus & Sindroma Metabolik PITharryruswantoNo ratings yet
- Diabetes Excelente 2018Document10 pagesDiabetes Excelente 2018cochipinkNo ratings yet
- D1 001 Prof Rudi STAR - DM in Indonesia - From Theory To The Real WorldDocument37 pagesD1 001 Prof Rudi STAR - DM in Indonesia - From Theory To The Real WorldNovietha Lia FarizymelinNo ratings yet
- Management of Hyperglycemia in Type 2Document45 pagesManagement of Hyperglycemia in Type 2namjiji 9No ratings yet
- Diabetes Mellitus: Vy Vu Doctor of Pharmacy Hutech University 07/29/2020Document56 pagesDiabetes Mellitus: Vy Vu Doctor of Pharmacy Hutech University 07/29/2020cyber elf XNo ratings yet
- Inadequate Glycaemic Control and Therapeutic Management of Adults Over 65 Years Old With Type 2 Diabetes Mellitus in SpainDocument6 pagesInadequate Glycaemic Control and Therapeutic Management of Adults Over 65 Years Old With Type 2 Diabetes Mellitus in SpainDaniel BenitezNo ratings yet
- 12 - CHEER Predicting PreDM CVD Risk Obese TeensDocument61 pages12 - CHEER Predicting PreDM CVD Risk Obese TeensMinerva StanciuNo ratings yet
- DM Control and SGLT2Document75 pagesDM Control and SGLT2Thanc FishNo ratings yet
- BIOS LIFE - Diabetes in Control Study #2 by Steven Freed and David JoffeDocument1 pageBIOS LIFE - Diabetes in Control Study #2 by Steven Freed and David JoffeHisWellnessNo ratings yet
- DiabetesDocument30 pagesDiabetesSahar JoshNo ratings yet
- Diabetes ValuesDocument67 pagesDiabetes Valuesluckytung07100% (1)
- Increase Prevalence of DM in Indonesia: Kapan Seseorang Dikatakan Diabetes? Kapan Seseorang Dikatakan Diabetes?Document8 pagesIncrease Prevalence of DM in Indonesia: Kapan Seseorang Dikatakan Diabetes? Kapan Seseorang Dikatakan Diabetes?riniNo ratings yet
- RABBIT-2 Surgery - (12 - 2010)Document32 pagesRABBIT-2 Surgery - (12 - 2010)aromerozNo ratings yet
- Insulin Therapy in Type 1 Diabetes UpdateDocument83 pagesInsulin Therapy in Type 1 Diabetes UpdateasupicuNo ratings yet
- Initiation and Dose Optimization Basal Insulin in DM Patient. Are All Basal Insulin SameDocument65 pagesInitiation and Dose Optimization Basal Insulin in DM Patient. Are All Basal Insulin SameSyahrialNo ratings yet
- Glucose Control in Diabetes: Focus On SulfhonylureaDocument93 pagesGlucose Control in Diabetes: Focus On SulfhonylureascribdNo ratings yet
- Advisory Board PPT (Dr-2. Ida Ayu Kshanti SPPD, KEMD)Document29 pagesAdvisory Board PPT (Dr-2. Ida Ayu Kshanti SPPD, KEMD)scribdNo ratings yet
- Jack Leahy Insulin TherapyDocument44 pagesJack Leahy Insulin TherapyFrancisNo ratings yet
- The Basics of Diabetes: Phar 811 Peyton Teets Pharmd Candidate School of Pharmacy - West Virginia UniversityDocument39 pagesThe Basics of Diabetes: Phar 811 Peyton Teets Pharmd Candidate School of Pharmacy - West Virginia UniversityMa'rifatulAuliaNo ratings yet
- Asuhan Keperawatan Pada Diabetes Mellitus: Tavip Dwi Wahyuni, Skep. NS, M.KesDocument45 pagesAsuhan Keperawatan Pada Diabetes Mellitus: Tavip Dwi Wahyuni, Skep. NS, M.KesTiyan Ramanda PNo ratings yet
- Epidemiologi, Pathogenesis, Diagnosis DM, BPJS 2015Document35 pagesEpidemiologi, Pathogenesis, Diagnosis DM, BPJS 2015Samuel Albert Andrian SiagianNo ratings yet
- Management of Gestational Diabetes and Type-2 Diabetes in PR PDFDocument75 pagesManagement of Gestational Diabetes and Type-2 Diabetes in PR PDFYohannis AsefaNo ratings yet
- Obesity, Cardiovascular Disease,: Diabetes Mellitus, CancerDocument28 pagesObesity, Cardiovascular Disease,: Diabetes Mellitus, CancerEmran HossainNo ratings yet
- Dr. D.N. Prastowo, SP - PD: Bagian Penyakit Dalam Rs. Hana Charitas - Arga Makmur Bengkulu 2017Document45 pagesDr. D.N. Prastowo, SP - PD: Bagian Penyakit Dalam Rs. Hana Charitas - Arga Makmur Bengkulu 2017nanikNo ratings yet
- Himawan - BPJSDocument26 pagesHimawan - BPJSAndi Upik FathurNo ratings yet
- Practical Management Considerations For Patients With Type 2 DiabetesDocument47 pagesPractical Management Considerations For Patients With Type 2 DiabetesRahmah HambaliNo ratings yet
- 202-Article Text-345-1-10-20180117Document6 pages202-Article Text-345-1-10-20180117Fifi RetiatyNo ratings yet
- 3 - Case Study 2-Insulin For IntensificationDocument30 pages3 - Case Study 2-Insulin For IntensificationBiswojit BeheraNo ratings yet
- Association Between Eating Behavior and Poor Glycemic Control in Japanese AdultsDocument6 pagesAssociation Between Eating Behavior and Poor Glycemic Control in Japanese AdultsmosabNo ratings yet
- Understanding Chronic Kidney Disease (CKD) : Epidemiology, Identification, and Monitoring Medical Nutrition TherapyDocument81 pagesUnderstanding Chronic Kidney Disease (CKD) : Epidemiology, Identification, and Monitoring Medical Nutrition TherapyDaniel Apuan SalviejoNo ratings yet
- Jurnal Pilihan PDFDocument4 pagesJurnal Pilihan PDFIWayanSuparthanayaNo ratings yet
- Association Between Betel-Nut Chewing and Chronic Kidney Disease in MenDocument6 pagesAssociation Between Betel-Nut Chewing and Chronic Kidney Disease in MenAaron Paul BernasNo ratings yet
- The Role of Prandial Insulin After Basal Optimization Slide IntentionDocument25 pagesThe Role of Prandial Insulin After Basal Optimization Slide IntentionsatyabasukiNo ratings yet
- Simpo 3 - Dr. Bowo SP - pd-kEMD - How TPatients With Co-Formulation InsulinDocument35 pagesSimpo 3 - Dr. Bowo SP - pd-kEMD - How TPatients With Co-Formulation InsulinAgnes Irene ZagotoNo ratings yet
- Insulinoterapia: Luis Antonio Rodríguez. Fellow-Endocrinología Clínica y Metabolismo 2020Document106 pagesInsulinoterapia: Luis Antonio Rodríguez. Fellow-Endocrinología Clínica y Metabolismo 2020Carlos PerezNo ratings yet
- Prevalence of Pre-Diabetes and Diabetes Mellitus in Polycystic Ovarian Syndrome (PCOS)Document2 pagesPrevalence of Pre-Diabetes and Diabetes Mellitus in Polycystic Ovarian Syndrome (PCOS)dkhatri01No ratings yet
- Diabetes Educat Today To Protect TomorrowDocument2 pagesDiabetes Educat Today To Protect Tomorrowoarc oarcNo ratings yet
- Diabetes Management GuidelinesDocument52 pagesDiabetes Management GuidelinesJoana MarauNo ratings yet
- Jakoby2011 PROTOCOLODocument6 pagesJakoby2011 PROTOCOLOMau MillanNo ratings yet
- Early Insulinization - CloreDocument26 pagesEarly Insulinization - Cloremozartiano07No ratings yet
- Fullpapers Ph309d49688cfull PDFDocument14 pagesFullpapers Ph309d49688cfull PDFWindy Dwi ElviraNo ratings yet
- Kuliah DM Dr. Amrizal, SPPD, Finasim 2Document50 pagesKuliah DM Dr. Amrizal, SPPD, Finasim 2Ahmad RamadhanuNo ratings yet
- DkaDocument83 pagesDkaRajaKumar Ponnana100% (1)
- Assignment #1 - Therapist Personality TraitsDocument9 pagesAssignment #1 - Therapist Personality TraitsLekai TaoNo ratings yet
- Medication GuidesDocument38 pagesMedication GuidesEko YuliantoNo ratings yet
- Therapeutic Monitoring of Amiodarone PharmacokinetDocument11 pagesTherapeutic Monitoring of Amiodarone PharmacokinetNanda apriliantoNo ratings yet
- Psychology - Psychological BoundariesDocument5 pagesPsychology - Psychological BoundariesDisha TNo ratings yet
- Polyps and PolyposisDocument52 pagesPolyps and PolyposisorianattNo ratings yet
- Schizophrenia As A Disorder of The SelfDocument7 pagesSchizophrenia As A Disorder of The Selfburrito2000No ratings yet
- Abnormaluterineaction 100515015711 Phpapp01Document40 pagesAbnormaluterineaction 100515015711 Phpapp01Seema Vashisht100% (1)
- Exit Test: Name: - Date: - Section 1: VocabularyDocument3 pagesExit Test: Name: - Date: - Section 1: VocabularyPaulina CardinaleNo ratings yet
- Prenatal DiagnosisDocument5 pagesPrenatal Diagnosissarguss14No ratings yet
- Nmrao ResumeDocument4 pagesNmrao ResumeNag Mallesh RaoNo ratings yet
- Different Inflammatory Arthitis: Juvenile Idiopathic ArthritisDocument1 pageDifferent Inflammatory Arthitis: Juvenile Idiopathic ArthritisDinesh ReddyNo ratings yet
- Anecca 10 Points Poster EnglishDocument1 pageAnecca 10 Points Poster EnglishDrake Wa YesuNo ratings yet
- Electrocauterio ManualDocument52 pagesElectrocauterio ManualEsther Copeland100% (1)
- Wiley Protocol Consumer Newsletter September 2009Document3 pagesWiley Protocol Consumer Newsletter September 2009WileyProtocolNo ratings yet
- Profed07-Foundation of Special and Inclusive Education-Chapter 2Document9 pagesProfed07-Foundation of Special and Inclusive Education-Chapter 2Ken100% (1)
- Peds Pu 39-41Document60 pagesPeds Pu 39-41Abel Jr IdusmaNo ratings yet
- Life of Dr. Clarke: Author: Sue YoungDocument4 pagesLife of Dr. Clarke: Author: Sue Youngkrishna2205100% (1)
- ETT Vs LMADocument33 pagesETT Vs LMAitaindrianiNo ratings yet
- Laura Armistead ResumeDocument3 pagesLaura Armistead Resumeapi-384327266No ratings yet
- Existentialism in Personal DevelopmentDocument19 pagesExistentialism in Personal DevelopmentjasmingacutanNo ratings yet
- Chapter 1. History and Physical Examination - Art and ScienceDocument3 pagesChapter 1. History and Physical Examination - Art and SciencecarolineNo ratings yet
- BLS Manual For Online - Clerks PDFDocument41 pagesBLS Manual For Online - Clerks PDFMiko Vargas100% (2)
- Coolsculpting Fat Removal SurgeryeztwiDocument8 pagesCoolsculpting Fat Removal Surgeryeztwishadowvault0No ratings yet
- Dr. Vanessa Kusumawardhani, Dipl - Cidesco, Dipl - CibtacDocument2 pagesDr. Vanessa Kusumawardhani, Dipl - Cidesco, Dipl - CibtacRyo KlasikaNo ratings yet
- Anesthesiology: Ketamine Psychedelic and Antinociceptive Effects Are ConnectedDocument62 pagesAnesthesiology: Ketamine Psychedelic and Antinociceptive Effects Are ConnectedMichiel van ElkNo ratings yet
- Anzca Blue Book 2011Document222 pagesAnzca Blue Book 2011pink_gorillazNo ratings yet
- Nursing Process SOAPIEDocument33 pagesNursing Process SOAPIEChoi Gong Ju100% (4)
- HyponatremiaDocument42 pagesHyponatremiaAbdu Raheem100% (1)
- Ointments For FungalDocument11 pagesOintments For FungalCrisanta MarieNo ratings yet
- Activity DesignDocument2 pagesActivity DesignRhu New Lucena90% (20)