You might also like
- Malaria Microscopy WHO PDFDocument140 pagesMalaria Microscopy WHO PDFsarasNo ratings yet
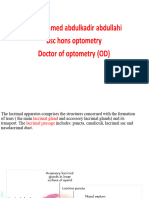
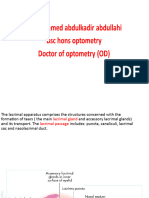
- Ch02 LacrimalDocument13 pagesCh02 Lacrimalwessam284No ratings yet
- 02.lacrimal Drainage SystemDocument15 pages02.lacrimal Drainage SystemSilvia RozaNo ratings yet
- 295212557-Dakriosistitis Id enDocument22 pages295212557-Dakriosistitis Id enSelfa YunitaNo ratings yet
- DacryocystorhinostomyDocument2 pagesDacryocystorhinostomyamolsuryaNo ratings yet
- Ophtha The Lacrimal SystemDocument32 pagesOphtha The Lacrimal SystemGeorgemar AranaNo ratings yet
- NewDocument24 pagesNewdevb110695No ratings yet
- L5 lacrimal apparatous -Document28 pagesL5 lacrimal apparatous -X And ZNo ratings yet
- Coclia EyelidDocument5 pagesCoclia EyelidFaradila HakimNo ratings yet
- Anatomy of Eye AppendigesDocument19 pagesAnatomy of Eye AppendigesSiyaNo ratings yet
- Endoscopic Dacryocystorhinostomy - DCR - Surgical TechniqueDocument11 pagesEndoscopic Dacryocystorhinostomy - DCR - Surgical TechniqueLuis De jesus SolanoNo ratings yet
- Anatomy & Physiology of Lacrimal Secretion & Outflow: DR - Nurcahya Ab, SPMDocument51 pagesAnatomy & Physiology of Lacrimal Secretion & Outflow: DR - Nurcahya Ab, SPMLianSiahaanNo ratings yet
- L5 lacrimal apparatous -Document28 pagesL5 lacrimal apparatous -X And ZNo ratings yet
- Anatomy & Physiology of Lacrimal Secretion & Outflow: DR - Nurcahya Ab, SPMDocument51 pagesAnatomy & Physiology of Lacrimal Secretion & Outflow: DR - Nurcahya Ab, SPMsaddamNo ratings yet
- Phatology The Eyelids, Lacrimal GlandsDocument62 pagesPhatology The Eyelids, Lacrimal GlandsGermanyNo ratings yet
- نسخة Opthalmology AnatomyDocument25 pagesنسخة Opthalmology AnatomyMhm MhmNo ratings yet
- The Tearing Patient: Diagnosis and Management: Ophthalmic PearlsDocument3 pagesThe Tearing Patient: Diagnosis and Management: Ophthalmic PearlsAnonymous otk8ohj9No ratings yet
- Ocular PhysiologyDocument80 pagesOcular PhysiologyKenny KayNo ratings yet
- Wolff's Anatomy-Capitulo 2Document55 pagesWolff's Anatomy-Capitulo 2Agustín AlberdiNo ratings yet
- Anatomy and Physiology of Lacrimal Apparatus: Dr.M.keerthana Dept of OphthalmologyDocument54 pagesAnatomy and Physiology of Lacrimal Apparatus: Dr.M.keerthana Dept of OphthalmologykeerthanaNo ratings yet
- PDF TraumaoculinonperforansDocument4 pagesPDF TraumaoculinonperforansCHRISTINE EriskaNo ratings yet
- Ocular Anatomy OverviewDocument89 pagesOcular Anatomy OverviewFikri M Asgar SNo ratings yet
- Tear Production and Drainage: Eyelid MusclesDocument2 pagesTear Production and Drainage: Eyelid MusclesMaksum Muh MaksumNo ratings yet
- Opthal Book Piyush SirDocument210 pagesOpthal Book Piyush Sirselmon468No ratings yet
- Jurnal ET 12Document13 pagesJurnal ET 12shendi amalia putriNo ratings yet
- 8 Lacrimal Drainage System Diseases by James PMDocument63 pages8 Lacrimal Drainage System Diseases by James PMCharles AntonyNo ratings yet
- Crvo CraoDocument80 pagesCrvo CraoRakshit AgrawalNo ratings yet
- Pathogenesis of Glaucoma: Determinants of Intraocular PressureDocument17 pagesPathogenesis of Glaucoma: Determinants of Intraocular PressureAdi TriNo ratings yet
- Resume Ulkus CorneaDocument10 pagesResume Ulkus CorneaNita RosianiNo ratings yet
- Anatomy & Physiology of Lacrimal Secretion & OutflowDocument60 pagesAnatomy & Physiology of Lacrimal Secretion & OutflowHenok BirukNo ratings yet
- Conjuctiva 1Document47 pagesConjuctiva 1maleeha shahzadNo ratings yet
- Kelenjar LakrimalDocument44 pagesKelenjar LakrimalNurfanida Natasya MNo ratings yet
- Puyalasa (Dacryocystitis) : Dr. Preeti PatelDocument37 pagesPuyalasa (Dacryocystitis) : Dr. Preeti PatelPreeti PatelNo ratings yet
- Kanski Clinical Ophthalmology Chapter 3 ORBITDocument43 pagesKanski Clinical Ophthalmology Chapter 3 ORBITSekar Ayu WulandariNo ratings yet
- Superficie Ocular ConejosDocument14 pagesSuperficie Ocular ConejosRueca HelenciyaNo ratings yet
- Repair Cherry Eye in DogsDocument11 pagesRepair Cherry Eye in DogsPambudiNo ratings yet
- Cornea Structure and Keratoconus IntroductionDocument33 pagesCornea Structure and Keratoconus IntroductionMuhammad MustafaNo ratings yet
- Jurnal 2Document9 pagesJurnal 2budiNo ratings yet
- 1-Anatomy of The Eye BallDocument6 pages1-Anatomy of The Eye BalltressNo ratings yet
- Tema 2Document3 pagesTema 2Hey its MuliNo ratings yet
- Eye and AdnexaDocument22 pagesEye and AdnexaWadabiNo ratings yet
- DACRYOCYSTITISDocument3 pagesDACRYOCYSTITISaynin39No ratings yet
- Lesiones Del Globo OcularDocument10 pagesLesiones Del Globo OcularRulo LugoNo ratings yet
- AP LacrimalDocument38 pagesAP LacrimalIoana MovileanuNo ratings yet
- Conjunctiva: Fourth Year Omar Al-Mukhtar Univercity 2019-2020Document55 pagesConjunctiva: Fourth Year Omar Al-Mukhtar Univercity 2019-2020Helene AlawamiNo ratings yet
- ANATOMY & PHYSIOLOGY: INNER EYEDocument71 pagesANATOMY & PHYSIOLOGY: INNER EYEGermanyNo ratings yet
- Corneal Vascularization: David G. CoganDocument9 pagesCorneal Vascularization: David G. CoganPraful ChaudharyNo ratings yet
- Phaco NightmaresDocument13 pagesPhaco NightmaresNiloy BasakNo ratings yet
- Anatomy of The Lacrimal ApparatusDocument22 pagesAnatomy of The Lacrimal ApparatusSivateja Reddy ChallaNo ratings yet
- Lacrimal SystemDocument31 pagesLacrimal Systemsulmiawatisyam100% (1)
- Anatomy'S Modul 10 Blok: Laboratory Anatomy Medical Faculty Muhammadiyah University of Purwokerto 2016Document21 pagesAnatomy'S Modul 10 Blok: Laboratory Anatomy Medical Faculty Muhammadiyah University of Purwokerto 2016Sari MentariNo ratings yet
- Diseases of The Eyelids: Mshangila Barnabas MD, M.MedDocument31 pagesDiseases of The Eyelids: Mshangila Barnabas MD, M.MedCharles AnthonyNo ratings yet
- Diseases of Lacrimal ApparatusDocument46 pagesDiseases of Lacrimal Apparatusসপ্নে ছোয়া মন100% (1)
- ProP TropicalSerumforTreatmentDocument4 pagesProP TropicalSerumforTreatmentGhita Andreea-IoanaNo ratings yet
- External Dacrocystorhinostomy (DCR)Document3 pagesExternal Dacrocystorhinostomy (DCR)Zen KuangNo ratings yet
- Eyeball Movements and Accessory StructuresDocument16 pagesEyeball Movements and Accessory StructuresabdirizakNo ratings yet
- CONJUNCTIVADocument17 pagesCONJUNCTIVACHIMA ONWUKA MONGNo ratings yet
- Lacrimal System and Disorders: DR Asad FrazDocument30 pagesLacrimal System and Disorders: DR Asad FrazAsad Fraz0% (1)
- Trabeculectomy TechniqueDocument8 pagesTrabeculectomy TechniqueJose Antonio Fuentes VegaNo ratings yet
- Suprachoroidal Space InterventionsFrom EverandSuprachoroidal Space InterventionsShohista SaidkasimovaNo ratings yet
- 2021 Jun 6Document7 pages2021 Jun 6ujjwalbhardwazNo ratings yet
- Muluki Ain 2074 - Forensic MedicineDocument9 pagesMuluki Ain 2074 - Forensic MedicineujjwalbhardwazNo ratings yet
- Community 3Document4 pagesCommunity 3ujjwalbhardwazNo ratings yet
- Community 1Document4 pagesCommunity 1ujjwalbhardwazNo ratings yet
- 100 Objective Question and Answer of Plant PathologyDocument23 pages100 Objective Question and Answer of Plant PathologyNavneet KumarNo ratings yet
- Nursing Care for Clients with InfertilityDocument23 pagesNursing Care for Clients with Infertilityastraeax pandaNo ratings yet
- Efficacy ClotrimazoleDocument4 pagesEfficacy ClotrimazoleAlexandra ConstantinescuNo ratings yet
- Rickets and Osteomalacia: Moderator: Dr. P. TahbildarDocument43 pagesRickets and Osteomalacia: Moderator: Dr. P. TahbildarNorman RiyadiNo ratings yet
- Activated Charcoal UseDocument6 pagesActivated Charcoal UseRodney LangleyNo ratings yet
- Worksheet-3 17/06/2021: Microorganisms: Friend and Foe Class 8 Mcqs Questions With AnswersDocument6 pagesWorksheet-3 17/06/2021: Microorganisms: Friend and Foe Class 8 Mcqs Questions With Answersstory manNo ratings yet
- Enderal Book CollectionDocument266 pagesEnderal Book CollectionMagazyn BotNo ratings yet
- Name of The Medicinal ProductDocument7 pagesName of The Medicinal Productddandan_2No ratings yet
- CWTS Final For InstructorDocument147 pagesCWTS Final For Instructorbarbie janeNo ratings yet
- Validity and Reliability of The Portuguese Version of Mandibular Function Impairment QuestionnaireDocument8 pagesValidity and Reliability of The Portuguese Version of Mandibular Function Impairment QuestionnaireredhaputriNo ratings yet
- Podologia EquinaDocument9 pagesPodologia Equinaositos.amorositos26No ratings yet
- 2.0 Classification of Mental DisordersDocument3 pages2.0 Classification of Mental DisordersJohnBenedictRazNo ratings yet
- Office Orthopaedics: Ramirez, Bryan Paul GDocument57 pagesOffice Orthopaedics: Ramirez, Bryan Paul GBryan Paul RamirezNo ratings yet
- Urinary EliminationDocument9 pagesUrinary EliminationTuTitNo ratings yet
- HBV EASL CPG Slide Deck 2020Document48 pagesHBV EASL CPG Slide Deck 2020Ajeng TunjungputriNo ratings yet
- Detect Sugars in Foods and DrinksDocument6 pagesDetect Sugars in Foods and DrinksWen LongNo ratings yet
- Synergy CementlessDocument32 pagesSynergy CementlessSergiu Plesca100% (1)
- Arbour2013 HypoplasiaDocument5 pagesArbour2013 HypoplasiaCarolina GomezNo ratings yet
- Urinary Tract Infections in ChildrenDocument8 pagesUrinary Tract Infections in ChildrenLorelie AsisNo ratings yet
- Family Coping IndexDocument5 pagesFamily Coping IndexDarcey NicholeNo ratings yet
- Tumour Markers PPT by DR VijayDocument31 pagesTumour Markers PPT by DR Vijaydr vijay60% (5)
- Oncoward 5 April 2021Document140 pagesOncoward 5 April 2021MegaSariDewiNo ratings yet
- What Is Bronchitis 2Document3 pagesWhat Is Bronchitis 2lea jumawanNo ratings yet
- Chronic Fatigue Syndrome PDFDocument22 pagesChronic Fatigue Syndrome PDFsteffiecruz06No ratings yet
- Diseases of Gall Bladder & Bile DuctsDocument24 pagesDiseases of Gall Bladder & Bile DuctsChampak PaulNo ratings yet
- Cell Parts and Their FunctionsDocument6 pagesCell Parts and Their FunctionsJonathan MayoNo ratings yet
- Biology One Liner QuestionsDocument17 pagesBiology One Liner Questionskrishna100% (1)
- Baby Vaccination ProgramDocument1 pageBaby Vaccination Programplainspeak100% (1)
- لحل مشكلة كتابة الروشتات للأطفال PDFDocument253 pagesلحل مشكلة كتابة الروشتات للأطفال PDFOmarAly100% (4)