You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Group 3 Cardiovascular ProblemDocument52 pagesGroup 3 Cardiovascular ProblemWARREN WILLIAM PERAN100% (3)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Subjective Assessment FormDocument8 pagesSubjective Assessment FormTriana KarnadipaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Concept Map in Head and Neck CancerDocument3 pagesConcept Map in Head and Neck CancerWendy EscalanteNo ratings yet
- Consolidated Annotated Frequency List: We Make NO CLAIMS As To The Accuracy or Efficacy of The Frequencies Posted Here!Document69 pagesConsolidated Annotated Frequency List: We Make NO CLAIMS As To The Accuracy or Efficacy of The Frequencies Posted Here!Matimba SimangoNo ratings yet
- The Healing Power of GarlicDocument306 pagesThe Healing Power of Garlicphilanthropistxmidget9110100% (4)
- 4.0 Thick-Fluids-Poster 2 2019Document1 page4.0 Thick-Fluids-Poster 2 2019Ada EzeNo ratings yet
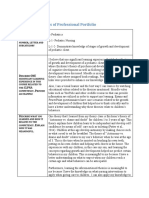
- Sample Professional Portfolio NFDN 2005 Developmental GrowthDocument2 pagesSample Professional Portfolio NFDN 2005 Developmental GrowthAda EzeNo ratings yet
- 4.0 Eating Well For Your GallbladderDocument2 pages4.0 Eating Well For Your GallbladderAda EzeNo ratings yet
- 3.2 Guiding Principle For Subcutaneous TherapyDocument8 pages3.2 Guiding Principle For Subcutaneous TherapyAda EzeNo ratings yet
- SBAR Report To Physician About A Critical SituationDocument3 pagesSBAR Report To Physician About A Critical SituationAda EzeNo ratings yet
- Pet BrochureDocument20 pagesPet BrochureSheikh Hasnain AliNo ratings yet
- First Aid Kit ContentsDocument8 pagesFirst Aid Kit Contentsalexis mae lavitoriaNo ratings yet
- Pressure Injuries (Pressure Ulcers) and Wound Care - Practice Essentials, Background, AnatomyDocument13 pagesPressure Injuries (Pressure Ulcers) and Wound Care - Practice Essentials, Background, AnatomyKarilNo ratings yet
- 6 TypesDocument3 pages6 TypesSelena BejoNo ratings yet
- Anxiety Related To Hospitalization and Disease Condition As Manifested by Fiscal Expression and VerbalizationDocument2 pagesAnxiety Related To Hospitalization and Disease Condition As Manifested by Fiscal Expression and VerbalizationmonaNo ratings yet
- The Wills Eye Hospital Atlas of Clinical Ophthalmology: Second EditionDocument495 pagesThe Wills Eye Hospital Atlas of Clinical Ophthalmology: Second EditionPeer TutorNo ratings yet
- Website Tachycardia Algorithm DiagramDocument1 pageWebsite Tachycardia Algorithm Diagramcolette zgheibNo ratings yet
- Chronic Kidney DiseaseDocument18 pagesChronic Kidney DiseaseAde Cahyo IslamiNo ratings yet
- Fibromatosis of The Breast Mimicking Cancer: A Case Report: SciencedirectDocument5 pagesFibromatosis of The Breast Mimicking Cancer: A Case Report: SciencedirectNabilla Rahma PutriNo ratings yet
- Epididymitis and OrchitisDocument11 pagesEpididymitis and Orchitiscitra08No ratings yet
- Ophthalmonics 1st EditionDocument116 pagesOphthalmonics 1st Editiondhavalb2086% (7)
- Tuberculosis Spondylitis IIDocument40 pagesTuberculosis Spondylitis IICendraiin MinangkabauNo ratings yet
- Infectious Diseases and Their Treatment in Georgian Written SourcesDocument21 pagesInfectious Diseases and Their Treatment in Georgian Written SourcesIrina GogonaiaNo ratings yet
- Wound AssessmentDocument64 pagesWound AssessmentKeown MukhtarNo ratings yet
- Gan Cao Xie Xin TangDocument2 pagesGan Cao Xie Xin TangAshley Flores100% (1)
- Agents of Opportunistic MycosesDocument6 pagesAgents of Opportunistic MycosesReinDePabloNo ratings yet
- H1N1 Diagnosis, Management and TreatmentDocument56 pagesH1N1 Diagnosis, Management and TreatmentNishanth BabuNo ratings yet
- Algorithm Immunisation Status Jan2020Document1 pageAlgorithm Immunisation Status Jan2020Afsan BulbulNo ratings yet
- Practical 4 Cardivascular and Hepatobiliary SystemDocument9 pagesPractical 4 Cardivascular and Hepatobiliary SystemchinNo ratings yet
- Seroprevalence of Leptospirosis Among People in Shabramant Village, EgyptDocument9 pagesSeroprevalence of Leptospirosis Among People in Shabramant Village, EgyptHielmy Auliya HasyimNo ratings yet
- Susunan Acara Simposium Pertemuan Ilmiah Ilmu Penyakit Dalam (Pit Ipd) 2020Document4 pagesSusunan Acara Simposium Pertemuan Ilmiah Ilmu Penyakit Dalam (Pit Ipd) 2020Getty InasNo ratings yet
- Venous InsufficiencyDocument32 pagesVenous InsufficiencyRalucaNo ratings yet
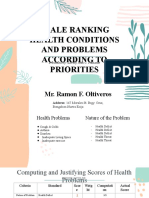
- SCALE RANKING HEALTH CONDITIONS AND PROBLEMS ACCORDING TO PRIORITIES - Funtanar, Lovely Jean C.Document15 pagesSCALE RANKING HEALTH CONDITIONS AND PROBLEMS ACCORDING TO PRIORITIES - Funtanar, Lovely Jean C.Lovely FuntanarNo ratings yet
- Stds MCQDocument181 pagesStds MCQhesham100% (1)
- Shri Guru Ram Rai University: School of Agricultural ScienceDocument27 pagesShri Guru Ram Rai University: School of Agricultural Sciencesuyash joshiNo ratings yet