You might also like
- PGVIM International Symposium 2019Document76 pagesPGVIM International Symposium 2019AnoThai NitibhonNo ratings yet
- Construction Health and Safety ProgramDocument15 pagesConstruction Health and Safety ProgramKiel CorpuzNo ratings yet
- Approval of - Concurewb309-As Concrete Curing CompoundDocument4 pagesApproval of - Concurewb309-As Concrete Curing Compoundsalman tariqNo ratings yet
- Accounting Information Systems, 6: Edition James A. HallDocument46 pagesAccounting Information Systems, 6: Edition James A. Halljlp5329100% (1)
- Embeding Quotes Power PointDocument11 pagesEmbeding Quotes Power PointSumati SachdevNo ratings yet
- In-Wash Scent Boosters A Game Changer For Laundry CareDocument59 pagesIn-Wash Scent Boosters A Game Changer For Laundry CareSwati JainNo ratings yet
- Duchenne Muscular DystrophyDocument5 pagesDuchenne Muscular Dystrophyapi-3801039100% (3)
- Top Silk Testador de MosfetDocument1 pageTop Silk Testador de MosfetEspedito Alves SilvaNo ratings yet
- VIV SALUD Plano 2Document1 pageVIV SALUD Plano 2fabiola godoyNo ratings yet
- Senusa Siap Print A4Document2 pagesSenusa Siap Print A4Eduardo Lucero RNo ratings yet
- FHGJHDocument1 pageFHGJHBenito CameloNo ratings yet
- Summary of Quarterly Grades: Fourth QuarterDocument3 pagesSummary of Quarterly Grades: Fourth Quartermarvin agubanNo ratings yet
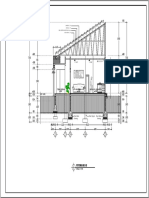
- Potongan B BDocument1 pagePotongan B BhabibsaukyzawfaniNo ratings yet
- Potongan B-B: R. Tamu 0.00 Dapur / R. Keluarga 0.00 Teras Depan - 0.00 M.T. - 0.30Document1 pagePotongan B-B: R. Tamu 0.00 Dapur / R. Keluarga 0.00 Teras Depan - 0.00 M.T. - 0.30Ethos SeptiansyahNo ratings yet
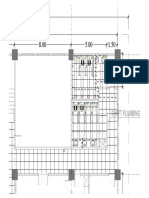
- Rencana Keramik LantaiDocument1 pageRencana Keramik Lantaigantino tinambunanNo ratings yet
- Denah Lantai 1: Skala 1: 100Document1 pageDenah Lantai 1: Skala 1: 100Hendra PratamaNo ratings yet
- Denah Rev 1Document1 pageDenah Rev 1tegar ramadhanNo ratings yet
- Escuela de Educacion Basica La Merced: EstudiantesDocument1 pageEscuela de Educacion Basica La Merced: EstudiantesdanielNo ratings yet
- St. Vincent's Catholic School of Bayambang, Inc.: Total TotalDocument6 pagesSt. Vincent's Catholic School of Bayambang, Inc.: Total TotalReygina Mae Sibayan PalaganasNo ratings yet
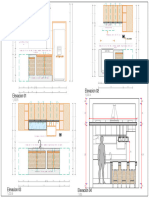
- Elevacion 02 Elevacion 01Document1 pageElevacion 02 Elevacion 01Jesus Angelo Vicente GarciaNo ratings yet
- E-CR JessaDocument26 pagesE-CR JessaJerome BalanquitNo ratings yet
- Section Diamond e Class RecordDocument24 pagesSection Diamond e Class RecordJerome BalanquitNo ratings yet
- Truss DetailDocument1 pageTruss DetailJezzrel SumalinogNo ratings yet
- TOMO - Konstrukcija - 1. StoryDocument1 pageTOMO - Konstrukcija - 1. StoryMatej RajičNo ratings yet
- 01.libro de BancosDocument15 pages01.libro de BancosCONTADORES PUBLICOS ASOCIADOSNo ratings yet
- 3.jembatan Sambungrejo - LelangDocument12 pages3.jembatan Sambungrejo - LelangOrin Orang InsyafNo ratings yet
- Glass Partitions Option 02Document1 pageGlass Partitions Option 02Sakib ChiplunkarNo ratings yet
- Truss Detail LegendDocument1 pageTruss Detail LegendGerard Paul CusiNo ratings yet
- Urban: Pay Date Cac No. Amount Paid Punch DateDocument1 pageUrban: Pay Date Cac No. Amount Paid Punch Dateanish kumarNo ratings yet
- Urban: Pay Date Cac No. Amount Paid Punch DateDocument1 pageUrban: Pay Date Cac No. Amount Paid Punch Dateanish kumarNo ratings yet
- Hitam PutihDocument1 pageHitam PutihKi Rekso AljeroNo ratings yet
- Hitam PutihDocument1 pageHitam PutihKi Rekso AljeroNo ratings yet
- Input Data Sheet For E-Class Record: Region Division School Name School Id School YearDocument6 pagesInput Data Sheet For E-Class Record: Region Division School Name School Id School Yearkoro angelicusNo ratings yet
- Wa0001Document1 pageWa0001Siphy MandlateNo ratings yet
- Flow SumpitDocument1 pageFlow SumpitMuhammad Fiqi SyaifuddinNo ratings yet
- PROYECTO 5CLL-ModelDocument1 pagePROYECTO 5CLL-ModelCESARNo ratings yet
- Rating Sheet CoverDocument3 pagesRating Sheet Coverbenjie panlicanNo ratings yet
- Rating Sheet: Capas National High SchoolDocument3 pagesRating Sheet: Capas National High Schoolbenjie panlicanNo ratings yet
- 0 20 40 60 80 100 Lag 0 20 40 60 80 100 LagDocument1 page0 20 40 60 80 100 Lag 0 20 40 60 80 100 LagStephanie PeRez GNo ratings yet
- Captura de Tela 2020-09-10 À(s) 10.19.04Document1 pageCaptura de Tela 2020-09-10 À(s) 10.19.04veronicascramimNo ratings yet
- LT 1Document1 pageLT 1febi rachmawatiNo ratings yet
- E ClassrecordDocument11 pagesE ClassrecordNedel Joyce Christine LibunaoNo ratings yet
- Detalle Estructural A3.Document1 pageDetalle Estructural A3.wincho Aparicio90No ratings yet
- Class Record: Region Division School Name School Id School YearDocument5 pagesClass Record: Region Division School Name School Id School YearSharmaine Nacional AlmodielNo ratings yet
- WTS Shaft AlignmentDocument65 pagesWTS Shaft Alignmentanak haruanNo ratings yet
- Eng, Fil, Esp, Ap Grade 1-10Document12 pagesEng, Fil, Esp, Ap Grade 1-10Jubylyn AficialNo ratings yet
- Cronograma de Adquisicion de Materiales: Proyecto: FechaDocument4 pagesCronograma de Adquisicion de Materiales: Proyecto: FechaBrian UrciaNo ratings yet
- Pedoman Early Warning System: Revisi 1Document7 pagesPedoman Early Warning System: Revisi 1Jihan ShelvyNo ratings yet
- Baza e Themeleve PDFDocument1 pageBaza e Themeleve PDFismet mehmetiNo ratings yet
- ARQUITECTURADocument1 pageARQUITECTURAfrancheska luana ramos chambiNo ratings yet
- Input Data Sheet For E-Class Record: Region Division District School Name School Id School YearDocument21 pagesInput Data Sheet For E-Class Record: Region Division District School Name School Id School Yeardavid johnNo ratings yet
- Class Record For English, Filipino, AP, ESPDocument26 pagesClass Record For English, Filipino, AP, ESPCeline AjeroNo ratings yet
- LS PTARD2-Layout2.pdf URGENTEDocument1 pageLS PTARD2-Layout2.pdf URGENTEHenrry H. Hernandez JuarezNo ratings yet
- Measured LHCP Computed LHCP Measured RHCP Computed RHCPDocument1 pageMeasured LHCP Computed LHCP Measured RHCP Computed RHCPMohd Najib Mohd YasinNo ratings yet
- New Taman-ModelDocument1 pageNew Taman-Modelagung bijaksanaNo ratings yet
- Field Measurement SheetDocument9 pagesField Measurement SheetEngr. Md. Fahad A AlamNo ratings yet
- U DITCH R1-Layout4Document1 pageU DITCH R1-Layout4AHMAD VALHEINNo ratings yet
- Gangguan Bulan Kosong 2019Document1 pageGangguan Bulan Kosong 2019Ahmad ZainuriNo ratings yet
- GambarDocument1 pageGambarAEF SATRIADINo ratings yet
- Conjunto de AnillosDocument1 pageConjunto de AnillosAubert EnamoradoNo ratings yet
- Input Data Sheet For E-Class Record: Region Division District School Name School Id School YearDocument21 pagesInput Data Sheet For E-Class Record: Region Division District School Name School Id School YearJOJONo ratings yet
- Drawings - ENYAU BRIDGE 2-15mDocument10 pagesDrawings - ENYAU BRIDGE 2-15mSolomon AhimbisibweNo ratings yet
- Detail GateDocument2 pagesDetail Gatearif budiantoNo ratings yet
- Option 1 Basketball Lay-Out LakawanDocument1 pageOption 1 Basketball Lay-Out LakawanJoseph DomingoNo ratings yet
- Projeto Estrutural - 01.02Document1 pageProjeto Estrutural - 01.02Paulo Cesar CosmeNo ratings yet
- JACUZZIDocument1 pageJACUZZIventasNo ratings yet
- The Final Girls - Horror's Hottest Scream Queens (Danielle Harris, Erin Marie Hogan, Victoria de Mare, Pandie Suicide Interview) (From Hustler - January 2017)Document6 pagesThe Final Girls - Horror's Hottest Scream Queens (Danielle Harris, Erin Marie Hogan, Victoria de Mare, Pandie Suicide Interview) (From Hustler - January 2017)ganeshsingh158No ratings yet
- Syllabus For Botany - PGDocument3 pagesSyllabus For Botany - PGSVB 2018No ratings yet
- Holmstrom1982 Moral Hazard in TeamsDocument18 pagesHolmstrom1982 Moral Hazard in TeamsfaqeveaNo ratings yet
- Python - How To Find The Exact Intersection of A Curve (As NP - Array) With y 0 - Stack OverflowDocument4 pagesPython - How To Find The Exact Intersection of A Curve (As NP - Array) With y 0 - Stack OverflowChristian ZoundjiNo ratings yet
- 6909 Gcse EnglishDocument13 pages6909 Gcse EnglishseekingNo ratings yet
- The Antennagate Crisis ManagementDocument7 pagesThe Antennagate Crisis ManagementMenghui DaiNo ratings yet
- Zenoss Core Administration r6.1.0 d1611.17.339 PDFDocument211 pagesZenoss Core Administration r6.1.0 d1611.17.339 PDFArdo HirmawanNo ratings yet
- Resource List For Young PeopleDocument16 pagesResource List For Young PeopleThe Five O'Clock ClubNo ratings yet
- Mail - Rodrigo Zúñiga García - Outlook 5Document2 pagesMail - Rodrigo Zúñiga García - Outlook 5Rodrigo Zúñiga GarcíaNo ratings yet
- Birao Sas 11 Microbiology and ParasitologyDocument10 pagesBirao Sas 11 Microbiology and ParasitologyFrancis Jacob Dejecacion GarcesNo ratings yet
- Donnie DarkoDocument8 pagesDonnie DarkoTopängä MändingoNo ratings yet
- Green Synthesis and Characterization of Carica Papaya Leaf Extract Coated Silver NanoparticlesDocument8 pagesGreen Synthesis and Characterization of Carica Papaya Leaf Extract Coated Silver Nanoparticlesmuhammad attiqueNo ratings yet
- Shivam Shivhare: Contact ProfileDocument1 pageShivam Shivhare: Contact ProfileShivam shivhareNo ratings yet
- Edited by Foxit Reader Copyright (C) by Foxit Corporation, 2005-2009 For EvaluationDocument5 pagesEdited by Foxit Reader Copyright (C) by Foxit Corporation, 2005-2009 For EvaluationChristopher RamseyNo ratings yet
- Pgdca SemDocument13 pagesPgdca SemArvind SharmaNo ratings yet
- Structural Identification of Humber Bridge For Performance Prognosis 2015Document18 pagesStructural Identification of Humber Bridge For Performance Prognosis 2015정주호No ratings yet
- Moz - Mapi 1 Unicorp ProfileDocument30 pagesMoz - Mapi 1 Unicorp ProfilePillai S KumarNo ratings yet
- ViewpdfDocument11 pagesViewpdfBhanu Pratap Singh TomarNo ratings yet
- Worksheet CPAR 6 FinalDocument27 pagesWorksheet CPAR 6 FinalGillian GabardaNo ratings yet
- Reading 30 Central ClearingDocument5 pagesReading 30 Central ClearingRahul GuptaNo ratings yet
- Ws1Ci: Water Specialist Control ValveDocument2 pagesWs1Ci: Water Specialist Control ValveDairo GomezNo ratings yet
- Wheel Cover Affected by The Heat Generated in The Brake SystemDocument14 pagesWheel Cover Affected by The Heat Generated in The Brake SystemRicardo Lopes FerreiraNo ratings yet
- Reaction Notes-ChemistryDocument19 pagesReaction Notes-ChemistrySirupyEwe GamerNo ratings yet