You might also like
- Salivary Gland TumoursDocument34 pagesSalivary Gland Tumoursnsv.epicNo ratings yet
- 50315-72475-1-PB (1) Parotid TumorDocument3 pages50315-72475-1-PB (1) Parotid TumorShashank MisraNo ratings yet
- Parotidectomy: H.Shameer AhamedDocument47 pagesParotidectomy: H.Shameer AhamedAndreas RendraNo ratings yet
- Parotid Gland NeoplasmDocument107 pagesParotid Gland NeoplasmigorNo ratings yet
- Salivary Gland Tumours and Other Lesions BDS 4Document38 pagesSalivary Gland Tumours and Other Lesions BDS 4dunisanijamesonNo ratings yet
- Salivary Gland TumorsDocument29 pagesSalivary Gland Tumorssajidali143No ratings yet
- Pediatric Neck Masses, TEF, Diaphragmatic HerniaDocument101 pagesPediatric Neck Masses, TEF, Diaphragmatic HerniaDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Tumors of External and Middle EarDocument42 pagesTumors of External and Middle EarAmiteshwar SinghNo ratings yet
- Tumors of Salivary GlandDocument28 pagesTumors of Salivary Glandrameshparajuli14100% (1)
- Parotid Ek Tom IDocument25 pagesParotid Ek Tom IYondi Piter PapulungNo ratings yet
- Kelainan KongenitalDocument20 pagesKelainan KongenitalMelita GanNo ratings yet
- Congenital Cystic Masses of NeckDocument47 pagesCongenital Cystic Masses of NeckFibrianti SeputriNo ratings yet
- Approach To Parapharyngeal SpaceDocument38 pagesApproach To Parapharyngeal SpaceZaid Rafi AlzobaidyNo ratings yet
- Parapharyngeal Space TumorsDocument60 pagesParapharyngeal Space TumorsHossam ThabetNo ratings yet
- Tumor Ganas Mata: Alfa SylvestrisDocument53 pagesTumor Ganas Mata: Alfa SylvestrisAzilu FalaNo ratings yet
- TMP C814Document51 pagesTMP C814Frontiers100% (1)
- Malignant Tumors: Dr.N.Govindrajkumar Reader Dept - Oral &maxillo Facial PathologyDocument50 pagesMalignant Tumors: Dr.N.Govindrajkumar Reader Dept - Oral &maxillo Facial PathologypriyaNo ratings yet
- Meningomas: DR - Md.Humayun RashidDocument42 pagesMeningomas: DR - Md.Humayun RashidDr.Humayun Rashid SagorNo ratings yet
- Discuss - 1) Aetiology 2) Pathology 3) Diagnosis 4) ManagementDocument14 pagesDiscuss - 1) Aetiology 2) Pathology 3) Diagnosis 4) ManagementAzizan HannyNo ratings yet
- Seminar Omfs BDSDocument17 pagesSeminar Omfs BDSHarshal AbdullaNo ratings yet
- Neck LumpDocument18 pagesNeck LumpJosh BurkeNo ratings yet
- Salivary GlandsDocument58 pagesSalivary GlandsApollo DentalNo ratings yet
- Shibini Seminar OmfsDocument17 pagesShibini Seminar OmfsHarshal AbdullaNo ratings yet
- Parotidectomy: Presenter: DR Prashanth L Moderator: DR R M LalithaDocument98 pagesParotidectomy: Presenter: DR Prashanth L Moderator: DR R M LalithanasimNo ratings yet
- Salivary GlandtumorsDocument20 pagesSalivary Glandtumorssamys2ndemailNo ratings yet
- Journal ReadingDocument41 pagesJournal ReadingEndorfin AdrenalinNo ratings yet
- Benign Salivary Gland Tumors - Dr. Nermine El Bahey (2019-2020)Document13 pagesBenign Salivary Gland Tumors - Dr. Nermine El Bahey (2019-2020)MOHAMED AMINNo ratings yet
- Schwannoma of The Lumbar SpineDocument35 pagesSchwannoma of The Lumbar SpinekurniaNo ratings yet
- Malignant Parotid Tumors: Introduction and AnatomyDocument1 pageMalignant Parotid Tumors: Introduction and AnatomyCeriaindriasariNo ratings yet
- Oral Neoplasma III SoundDocument53 pagesOral Neoplasma III SoundJi ChuNo ratings yet
- Nasal TumorDocument20 pagesNasal TumorMahmoud ElsherbenyNo ratings yet
- Parotid EctomyDocument33 pagesParotid EctomyAgung Anom Arie WiradanaNo ratings yet
- Superficial ParotidectomyDocument7 pagesSuperficial ParotidectomySajid Hussain ShahNo ratings yet
- Surgical Management of Oropharyngeal CarcinomaDocument15 pagesSurgical Management of Oropharyngeal CarcinomaGleamine PaulrajNo ratings yet
- Oral Cancer and ManagementDocument148 pagesOral Cancer and ManagementFadilaNo ratings yet
- Sinus CholesteatomaDocument3 pagesSinus CholesteatomaAdham YounesNo ratings yet
- Pediatric Cysts &tumors: Presented By: Supervised byDocument117 pagesPediatric Cysts &tumors: Presented By: Supervised byDorina MalanceaNo ratings yet
- Middle Ear Tumors - Dr. Shivendra PandeyDocument60 pagesMiddle Ear Tumors - Dr. Shivendra PandeyNupur GargNo ratings yet
- Disorders of The Salivary Glands 2Document109 pagesDisorders of The Salivary Glands 2ningappaNo ratings yet
- Glandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.Document2 pagesGlandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.juanrangoneNo ratings yet
- Management of Oral Cavity Bhans-1Document91 pagesManagement of Oral Cavity Bhans-1BhanuNo ratings yet
- Oral Cavity Malignancy-SurgeryDocument62 pagesOral Cavity Malignancy-SurgeryAsif AbbasNo ratings yet
- Benign Salivary Gland TumoursDocument7 pagesBenign Salivary Gland TumoursSathiyamoorthy KarunakaranNo ratings yet
- Parapharyngeal Space Compatibility ModeDocument66 pagesParapharyngeal Space Compatibility ModeDrsiya MedfriendNo ratings yet
- Carcinoma Penis: Pravin NarkhedeDocument36 pagesCarcinoma Penis: Pravin Narkhedepravin narkhede100% (1)
- Salivary Gland Tumors: Marka Crittenden M.D. PH.DDocument54 pagesSalivary Gland Tumors: Marka Crittenden M.D. PH.DNeeti JainNo ratings yet
- BSD Sellar Region - HADocument19 pagesBSD Sellar Region - HAHafiz ArqursoyNo ratings yet
- Surgical Excision of Congenital Dermoid Cysts in The OrbitDocument10 pagesSurgical Excision of Congenital Dermoid Cysts in The OrbitIOSRjournal100% (1)
- Benign Tumors of Nose and NasopharynxDocument39 pagesBenign Tumors of Nose and Nasopharynxmanoj kumarNo ratings yet
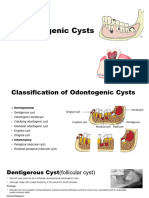
- Odontogenic CystDocument16 pagesOdontogenic CystMahsaNo ratings yet
- Salivary Gland Neoplasm: Dr. Saad Al-Muhayawi. M.D., FRCSC Associate Professor & Consultant ORL Head & Neck SurgeryDocument43 pagesSalivary Gland Neoplasm: Dr. Saad Al-Muhayawi. M.D., FRCSC Associate Professor & Consultant ORL Head & Neck Surgeryraishern5475No ratings yet
- Odontogenic CystDocument16 pagesOdontogenic CystMahsaNo ratings yet
- 15.oral Premalignant and Malignant ConditionDocument31 pages15.oral Premalignant and Malignant Conditionabhishek chaudharyNo ratings yet
- Debulking Surgery On Recurrent Dermal Neck Tumor Above Stoma After Total LaryngectomyDocument9 pagesDebulking Surgery On Recurrent Dermal Neck Tumor Above Stoma After Total LaryngectomyTeuku Ahmad HasanyNo ratings yet
- Management of Sinonasal Tumors: Prognostic Factors and Outcomes: A 10 Year Experience at A Tertiary Care HospitalDocument67 pagesManagement of Sinonasal Tumors: Prognostic Factors and Outcomes: A 10 Year Experience at A Tertiary Care HospitalDinaNihayatiNo ratings yet
- Imaging Radiologi Klinis Pada Sistem Indokrin Dan Metabolik-1Document25 pagesImaging Radiologi Klinis Pada Sistem Indokrin Dan Metabolik-1Angelia Saveq Liria LaiaNo ratings yet
- Salivary Gland Cancer: From Diagnosis to Tailored TreatmentFrom EverandSalivary Gland Cancer: From Diagnosis to Tailored TreatmentLisa LicitraNo ratings yet
- Penis Cancer, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPenis Cancer, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- SPINAL NERVE Presentation Completed-2Document51 pagesSPINAL NERVE Presentation Completed-2Sheikh Muhammad MuhallilNo ratings yet
- FCA 2 Trials MindmapDocument1 pageFCA 2 Trials MindmapameenallyNo ratings yet
- 1.psychiatric Neuroscience - Incorporating Pathophysiology Into Clinical Case Formulation - ClinicalKeyDocument43 pages1.psychiatric Neuroscience - Incorporating Pathophysiology Into Clinical Case Formulation - ClinicalKeyClaudia0% (1)
- Derm StuffDocument7 pagesDerm StuffSudesna Roy ChowdhuryNo ratings yet
- Cns MCQDocument11 pagesCns MCQAjay YadavNo ratings yet
- Management of Hypersensitivity ReactionDocument6 pagesManagement of Hypersensitivity Reactionmbeng bessonganyiNo ratings yet
- Kamal KV 500 Q CollectionsDocument13 pagesKamal KV 500 Q CollectionsBeta ReaderNo ratings yet
- DR Eva Detko Why You Can T Have A Healthy Gut Without Good Vagus FunctionDocument16 pagesDR Eva Detko Why You Can T Have A Healthy Gut Without Good Vagus Functioncharanmann9165100% (1)
- Types of Cataract: RabagoDocument17 pagesTypes of Cataract: RabagoNuhu BankwhotNo ratings yet
- NP4 Recalls7Document11 pagesNP4 Recalls7AhrisJeannine EscuadroNo ratings yet
- A Magnetic Resonance Imaging DEFINITIONDocument22 pagesA Magnetic Resonance Imaging DEFINITIONYosie Yulanda PutraNo ratings yet
- Full Download Book Surgery Pretest Self Assessment and Review 14E PDFDocument41 pagesFull Download Book Surgery Pretest Self Assessment and Review 14E PDFemilio.elliott723100% (16)
- Chapter 38: Care of Patients With Diabetes and Hypoglycemia: Multiple ChoiceDocument13 pagesChapter 38: Care of Patients With Diabetes and Hypoglycemia: Multiple ChoiceNurse UtopiaNo ratings yet
- Study Claims Agatha Christie Had AlzheimerDocument4 pagesStudy Claims Agatha Christie Had AlzheimerLuciana SilvaNo ratings yet
- Antidepressants, Antihistamines, General Anesthetics, MAO Inhibitors, OpioidsDocument3 pagesAntidepressants, Antihistamines, General Anesthetics, MAO Inhibitors, Opioidskaycelyn jimenezNo ratings yet
- The Gynecologic History and Pelvic Examination Up To Date 2016Document14 pagesThe Gynecologic History and Pelvic Examination Up To Date 2016Mateo GlNo ratings yet
- Pato Sakit Kritis PDFDocument44 pagesPato Sakit Kritis PDFrsia fatimahNo ratings yet
- Presentation 1Document12 pagesPresentation 1Maryam KhanNo ratings yet
- Par QPlus 2022Document7 pagesPar QPlus 2022MARIKA BALONDONo ratings yet
- Amenorrhea: Definition - This Is The Symptom of Absence of MenstruationDocument10 pagesAmenorrhea: Definition - This Is The Symptom of Absence of MenstruationSuhas IngaleNo ratings yet
- Oral CandidiasisDocument4 pagesOral CandidiasisAnish RajNo ratings yet
- Evaluation of Dysuria in AdultsDocument8 pagesEvaluation of Dysuria in AdultspapermintNo ratings yet
- Acute Myeloid Leukemia With Myelodysplasia RelatedDocument6 pagesAcute Myeloid Leukemia With Myelodysplasia RelatedAgus WiniNo ratings yet
- Skin LMRP 2019Document21 pagesSkin LMRP 2019skNo ratings yet
- Deep Vein ThrombosisDocument19 pagesDeep Vein ThrombosisDoctor MusicNo ratings yet
- Handout - Urine and Kidney CytopathologyDocument11 pagesHandout - Urine and Kidney Cytopathologylavisha.s.punjabiNo ratings yet
- Kitsap Co (WA) Protocols (2004)Document149 pagesKitsap Co (WA) Protocols (2004)Anthony James-HartwellNo ratings yet
- Anemia NotesDocument8 pagesAnemia Notesalin malekNo ratings yet
- Drug Analysis and NCP Ob Ward PoldoDocument9 pagesDrug Analysis and NCP Ob Ward PoldosatruetalagaNo ratings yet
- Clinical Manifestations, Differential Diagnosis, and Initial Management of Psychosis in Adults - UpToDateDocument12 pagesClinical Manifestations, Differential Diagnosis, and Initial Management of Psychosis in Adults - UpToDateImja94No ratings yet