You might also like
- Validation Letter For ThesisDocument1 pageValidation Letter For ThesisDoc Albert Nito LopezNo ratings yet
- Home-Visitation&Counseling Referral FormDocument2 pagesHome-Visitation&Counseling Referral FormCHARISSE TERRADONo ratings yet
- Amado M. Quirit Sr. National High SchoolDocument1 pageAmado M. Quirit Sr. National High SchoolIlyn Domingo NupatNo ratings yet
- Anecdotal NewDocument1 pageAnecdotal NewMarlyn P LavadorNo ratings yet
- Sampaloc Elementary School: May I Go Home SlipDocument1 pageSampaloc Elementary School: May I Go Home SlipNora De Guzman HerreraNo ratings yet
- Equivalent FractionsDocument2 pagesEquivalent FractionsJoma BuluranNo ratings yet
- Department of Education: Home Visitation FormDocument2 pagesDepartment of Education: Home Visitation Formrussel silvestreNo ratings yet
- TLE Grade 7 2nd WW Week 1-2Document2 pagesTLE Grade 7 2nd WW Week 1-2Jhomari Mollejon DiazNo ratings yet
- Department of Education: Republic of The PhilippinesDocument8 pagesDepartment of Education: Republic of The PhilippineslawrenceNo ratings yet
- Dropping FormDocument1 pageDropping FormDeorina CagdasNo ratings yet
- Art Activity 1.2 Direction A. On The Box Below, Fill The Arm With Your Own Tattoo Design. Use Only Black Ink To Fill That TattooDocument1 pageArt Activity 1.2 Direction A. On The Box Below, Fill The Arm With Your Own Tattoo Design. Use Only Black Ink To Fill That TattooCezar John SantosNo ratings yet
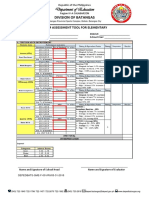
- School Form Early Grade Reading Assessment Component 1 4Document10 pagesSchool Form Early Grade Reading Assessment Component 1 4Mina Emmanuelle IngalNo ratings yet
- Student's Anecdotal RecordDocument1 pageStudent's Anecdotal RecordAilyn Gail AsueloNo ratings yet
- Sta Ursula Elementary School: Attendance General Pta Meeting Month of SeptemberDocument2 pagesSta Ursula Elementary School: Attendance General Pta Meeting Month of SeptemberKinn GarciaNo ratings yet
- Feedback Form TemplateDocument1 pageFeedback Form TemplateMERCY PABALANNo ratings yet
- Republic of The Philippines Region III-Central Luzon Department of Education Schools Division of Tarlac Province Sapang High SchoolDocument1 pageRepublic of The Philippines Region III-Central Luzon Department of Education Schools Division of Tarlac Province Sapang High SchoolEden CabarrubiasNo ratings yet
- Schools Division of Imus CityDocument1 pageSchools Division of Imus CityMalagasang-three IONo ratings yet
- In Take SheetDocument2 pagesIn Take SheetAdrienne HernandoNo ratings yet
- Counseling Referral Acknowledgement FormDocument1 pageCounseling Referral Acknowledgement FormcelestinoptrixieNo ratings yet
- Guidance FormDocument2 pagesGuidance Formronna ordinadoNo ratings yet
- Q2 ACR KamustahanDocument3 pagesQ2 ACR KamustahanCATHERINE MAGATNo ratings yet
- Drop Out FormDocument1 pageDrop Out FormManalang HenryNo ratings yet
- Potrero National High School: Schools Division Office of PampangaDocument3 pagesPotrero National High School: Schools Division Office of PampangaCherryl GatchalianNo ratings yet
- Department of Education: Republic of The PhilippinesDocument1 pageDepartment of Education: Republic of The PhilippinesAnn Raganas FonteNo ratings yet
- Annex 1 NLC Registration FormDocument2 pagesAnnex 1 NLC Registration FormJuLie Ann DeGuzman GeslaniNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesAida BellonNo ratings yet
- Math LAS Q2 M1Document2 pagesMath LAS Q2 M1JEMIMA BERNARDONo ratings yet
- Template For Collage MOVsDocument1 pageTemplate For Collage MOVsCha MirandaNo ratings yet
- Activity 8Document1 pageActivity 8Joma BuluranNo ratings yet
- Abm Pre Immersion Worksheets1Document9 pagesAbm Pre Immersion Worksheets1Rachel SantosNo ratings yet
- Anectodal ReportDocument2 pagesAnectodal Reportlailanie.cervantes002No ratings yet
- Grade 7 - Aquarius: Sto. Cristo Integrated SchoolDocument2 pagesGrade 7 - Aquarius: Sto. Cristo Integrated SchoolChelle PanganNo ratings yet
- Letter For Honor PupilsDocument3 pagesLetter For Honor PupilsErika Mae Tor TismoNo ratings yet
- Q3 ACR DistributionDocument6 pagesQ3 ACR DistributionCATHERINE MAGATNo ratings yet
- Sining Tanghalan Parental ConsentDocument1 pageSining Tanghalan Parental ConsentSapangMaisac ElementarySchoolNo ratings yet
- Smea SBMDocument1 pageSmea SBMHaidi MoralesNo ratings yet
- Intake SheetDocument2 pagesIntake SheetEleanor GelacioNo ratings yet
- 2 Application FormDocument3 pages2 Application FormJarish NatinoNo ratings yet
- Parents ConsentDocument1 pageParents ConsentRandy Evangelista CalayagNo ratings yet
- TVL - Information, Communication and Technology: Republic of The Philippines Region III-Central LuzonDocument1 pageTVL - Information, Communication and Technology: Republic of The Philippines Region III-Central LuzonJonald Grace Cesar ZafraNo ratings yet
- WHLP FormatDocument2 pagesWHLP FormatAngelica BackianNo ratings yet
- Anecdotal Record Form 1Document1 pageAnecdotal Record Form 1Quel Evangelista100% (1)
- Dropping FormDocument1 pageDropping FormKing Constantine DamasoNo ratings yet
- Department of Education: Activity SheetDocument3 pagesDepartment of Education: Activity SheetRubenNo ratings yet
- FIELDTRIP Consent FormDocument1 pageFIELDTRIP Consent FormGabrielle Anne San Gabriel100% (1)
- Home Visitation FormDocument1 pageHome Visitation FormcelestinoptrixieNo ratings yet
- 3RD Quarter-G5Document32 pages3RD Quarter-G5Louie De PedroNo ratings yet
- Certificate of EnrollmentDocument1 pageCertificate of EnrollmentJeff MedinaNo ratings yet
- Progress Chart in ReadingDocument1 pageProgress Chart in ReadingJOY TUYORNo ratings yet
- Acr Virtual Moving UpDocument9 pagesAcr Virtual Moving UpIrene MagatNo ratings yet
- JHENSON Actvityy Sheet For Academic TextDocument2 pagesJHENSON Actvityy Sheet For Academic TextJAMES HENSONNo ratings yet
- Engr. Guideon L. Taban: Suarez Central SchoolDocument5 pagesEngr. Guideon L. Taban: Suarez Central Schoolana timoganNo ratings yet
- Department of Education: I. Write Your Answer On The Space ProvidedDocument2 pagesDepartment of Education: I. Write Your Answer On The Space ProvidedAlexis De LeonNo ratings yet
- Reading Comprehension WorksheetsDocument11 pagesReading Comprehension WorksheetsJecyll Dajang WaminalNo ratings yet
- SHS-summer Class Parent Consent SY 2021-2022Document4 pagesSHS-summer Class Parent Consent SY 2021-2022merryjubilant menesesNo ratings yet
- Entrepreneurship: The 4Ms of Production in Relation To The Business Opportunity Quarter 3 - Module 1-Lesson 1Document1 pageEntrepreneurship: The 4Ms of Production in Relation To The Business Opportunity Quarter 3 - Module 1-Lesson 1Jay Dela Rama JovenNo ratings yet
- Reflection and Journal of TraineesDocument3 pagesReflection and Journal of TraineesReign Angela Abcidee TembliqueNo ratings yet
- Anecdotal RecordDocument1 pageAnecdotal RecordZol MendozaNo ratings yet
- Parental or Guardian Consent For Work Immersion 1Document1 pageParental or Guardian Consent For Work Immersion 1Kathrine Jane LunaNo ratings yet
- Education and Training: Delegate Information Pack (Handouts and Activities)From EverandEducation and Training: Delegate Information Pack (Handouts and Activities)No ratings yet