You might also like
- BuiltLean Get Lean GuideDocument22 pagesBuiltLean Get Lean Guideirda100% (1)
- Vocal Cord DysfunctionDocument12 pagesVocal Cord DysfunctionAzmachamberAzmacareNo ratings yet
- The Effect of Playing A Wind Instrument or Singing On Risk of Sleep Apnea: A Systematic Review and Meta-AnalysisDocument11 pagesThe Effect of Playing A Wind Instrument or Singing On Risk of Sleep Apnea: A Systematic Review and Meta-AnalysisFawn100% (1)
- Diagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaFrom EverandDiagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaNo ratings yet
- OENDL3000007Document260 pagesOENDL3000007yoonsv100% (2)
- SJAJ ANTICKIH GRKA Keramicke Posude SlikeeDocument563 pagesSJAJ ANTICKIH GRKA Keramicke Posude SlikeeAjdin Arapović100% (1)
- The List of the Korean Companies in the UAE: Company Name 이름 Off. Tel Off. Fax P.O.BoxDocument34 pagesThe List of the Korean Companies in the UAE: Company Name 이름 Off. Tel Off. Fax P.O.Boxnguyen phuong anh100% (1)
- Raising CapitalDocument43 pagesRaising CapitalMuhammad AsifNo ratings yet
- Mark Magazine#64Document197 pagesMark Magazine#64Андрей КанищевNo ratings yet
- Potot Vs People DigestDocument1 pagePotot Vs People DigestMary Grace SevillaNo ratings yet
- Post Op LaryngospasmDocument2 pagesPost Op Laryngospasmbalab2311No ratings yet
- Adult LaryngomlaciaDocument3 pagesAdult LaryngomlaciamitaNo ratings yet
- Usg in CADocument3 pagesUsg in CAJasmine EffendiNo ratings yet
- The Nose, Upper Airway, and Obstructive Sleep ApneaDocument7 pagesThe Nose, Upper Airway, and Obstructive Sleep ApneaDaniel Celestino DiazNo ratings yet
- Obstructive Sleep Apnea: An Overview On Features, Diagnosis & Orthodontic ManagementDocument6 pagesObstructive Sleep Apnea: An Overview On Features, Diagnosis & Orthodontic Managementsajida khanNo ratings yet
- The History of Sleep Surgery: Kathleen Yaremchuk Laura Garcia-RodriguezDocument5 pagesThe History of Sleep Surgery: Kathleen Yaremchuk Laura Garcia-RodriguezRehab BassamNo ratings yet
- Empty Nose Syndrome Post Radical Turbinate Surgery: Case ReportDocument2 pagesEmpty Nose Syndrome Post Radical Turbinate Surgery: Case ReportAlwi Qatsir AlyaNo ratings yet
- The Role of Oral Myofunctional Therapy in Managing Patients WithDocument7 pagesThe Role of Oral Myofunctional Therapy in Managing Patients Withpj.krzeszewskaNo ratings yet
- Obstructive Apneas During Sleep in Patients With Seasonal Allergic RhinitisDocument4 pagesObstructive Apneas During Sleep in Patients With Seasonal Allergic RhinitisIRENENo ratings yet
- Uvulo Palatal Flap PIIS1043181015000342Document7 pagesUvulo Palatal Flap PIIS1043181015000342barbiemeNo ratings yet
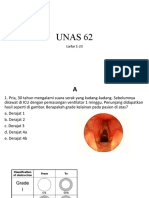
- UNAS 2022 Juni (Ke-62) Larfar 1-23, Al-Im 1-4Document51 pagesUNAS 2022 Juni (Ke-62) Larfar 1-23, Al-Im 1-4abubakar rizviNo ratings yet
- Three Axes in Sniffing PositionDocument2 pagesThree Axes in Sniffing PositionRose Ann Tambanillo AlvarezNo ratings yet
- OralmyofuncttherapyDocument7 pagesOralmyofuncttherapyagung anugrahNo ratings yet
- Bhalla 2011Document4 pagesBhalla 2011Fadlu ManafNo ratings yet
- Surgical Treatment of A Pattern I Obstructive Sleep Apnea Syndrome Individual - Clinical Case ReportDocument6 pagesSurgical Treatment of A Pattern I Obstructive Sleep Apnea Syndrome Individual - Clinical Case ReportMatheus CorreaNo ratings yet
- 2015 Effects of Oropharyngeal Exercises On SnoringDocument9 pages2015 Effects of Oropharyngeal Exercises On Snoringjuan pabloNo ratings yet
- Nazari An 2018Document16 pagesNazari An 2018Zakia DrajatNo ratings yet
- 2003, Vol.24. Issues 2, Sleep DisordersDocument189 pages2003, Vol.24. Issues 2, Sleep Disorderssantiago_auteriNo ratings yet
- Enfermedad de MeniereDocument3 pagesEnfermedad de MeniereJessica M ChNo ratings yet
- ETT Vs LMADocument33 pagesETT Vs LMAitaindrianiNo ratings yet
- Surgicaloptionsforthe Treatmentofobstructive Sleepapnea: Jon-Erik C. Holty,, Christian GuilleminaultDocument37 pagesSurgicaloptionsforthe Treatmentofobstructive Sleepapnea: Jon-Erik C. Holty,, Christian GuilleminaultJuan Pablo Mejia BarbosaNo ratings yet
- Tonsillectomy and Pharyngoplasty: Tissue-Preserving TechniquesDocument6 pagesTonsillectomy and Pharyngoplasty: Tissue-Preserving Techniqueslaljadeff12No ratings yet
- 2010 First-Night-Effect On PSG Respiratory Sleep Parameters in Patients With Sleep-Disordered Breathing and Upper Airway PathologyDocument5 pages2010 First-Night-Effect On PSG Respiratory Sleep Parameters in Patients With Sleep-Disordered Breathing and Upper Airway PathologyPsic ClinicaNo ratings yet
- Anestesi Pada Fraktur MandibulaDocument11 pagesAnestesi Pada Fraktur MandibulaCredo AriefNo ratings yet
- Short-Term Results of Upper Airway Stimulation in Obstructive Sleep Apnoea Patients: The Amsterdam ExperienceDocument6 pagesShort-Term Results of Upper Airway Stimulation in Obstructive Sleep Apnoea Patients: The Amsterdam ExperienceHamzeh AlsalhiNo ratings yet
- NIH Public Access: Author ManuscriptDocument9 pagesNIH Public Access: Author ManuscriptLaura Paola UrquizoNo ratings yet
- Postmedj00029 0051Document2 pagesPostmedj00029 0051balakrishna GolusuNo ratings yet
- MenereDocument11 pagesMenereJauhari JoNo ratings yet
- A Large Vocal Fold Polyp Causing Dyspnea HmeBDocument2 pagesA Large Vocal Fold Polyp Causing Dyspnea HmeBfanisaNo ratings yet
- 1998 Electrodiagnostic Methods For Neurogenic DysphagiaDocument10 pages1998 Electrodiagnostic Methods For Neurogenic DysphagiaSultan TarlacıNo ratings yet
- Tracheal StenosisDocument4 pagesTracheal StenosisJessica MarianoNo ratings yet
- DISEDocument4 pagesDISEMichael ANo ratings yet
- Association Between Breathing Route, Oxygen Desaturation, and Upper Airway MorphologyDocument6 pagesAssociation Between Breathing Route, Oxygen Desaturation, and Upper Airway MorphologyMark Burhenne DDSNo ratings yet
- PAPER (ENG) - (Shanahan T., Logemann J., Et Al., 1992 USA) Chin-Down Posture Effect On Aspiration in Dysphagic PatientsDocument5 pagesPAPER (ENG) - (Shanahan T., Logemann J., Et Al., 1992 USA) Chin-Down Posture Effect On Aspiration in Dysphagic PatientsAldo Hip NaranjoNo ratings yet
- Κουτσουρελάκης ΩΡΛDocument5 pagesΚουτσουρελάκης ΩΡΛΚουτσουρελακης ΩΡΛNo ratings yet
- Obstructive Sleep ApneaDocument9 pagesObstructive Sleep Apneasavvy_as_98No ratings yet
- The Effect of A Modified Functional Appliance On Obstructive Sleep ApneaDocument9 pagesThe Effect of A Modified Functional Appliance On Obstructive Sleep ApneaKishore Babu ParvathaneniNo ratings yet
- DIFFICULT EXTUBATION A Case Report.10Document2 pagesDIFFICULT EXTUBATION A Case Report.10Martin ValderramaNo ratings yet
- 498 FullDocument3 pages498 FullIndah D. RahmahNo ratings yet
- Burns 2008Document3 pagesBurns 2008Elok Chintya JaniseNo ratings yet
- 617 08 16 ArticleDocument8 pages617 08 16 Articlewilliam lozaNo ratings yet
- Br. J. Anaesth. 2013 Lamperti 888 91Document4 pagesBr. J. Anaesth. 2013 Lamperti 888 91rfr vfrvfrfNo ratings yet
- Obstructive Sleep ApneaDocument49 pagesObstructive Sleep ApnearuthNo ratings yet
- Effects of Respiratory Muscle Therapy On Obstructive Sleep Apnea: A Systematic Review and Meta-AnalysisDocument17 pagesEffects of Respiratory Muscle Therapy On Obstructive Sleep Apnea: A Systematic Review and Meta-AnalysisDavid SoaresNo ratings yet
- Lary 23467Document8 pagesLary 23467Dwi juliana DewiNo ratings yet
- Reporte de Un Caso - Pruebas Funcionales para Debilidad DiafragmáticaDocument4 pagesReporte de Un Caso - Pruebas Funcionales para Debilidad DiafragmáticaEzeBorjesNo ratings yet
- Epiglotitis DCHDocument6 pagesEpiglotitis DCHLu BfNo ratings yet
- J Ijporl 2012 07 023Document3 pagesJ Ijporl 2012 07 023Nida Fariza MaulanisaNo ratings yet
- Andrew Et Al.,2003Document4 pagesAndrew Et Al.,2003CaioSelaimenNo ratings yet
- Breathing Patterns in Children With Craniofacial Dysostosis and Hindbrain HerniationDocument7 pagesBreathing Patterns in Children With Craniofacial Dysostosis and Hindbrain HerniationDr.M.H. PatelNo ratings yet
- Eosinophilic Bronchitis, Eosinophilic GranulomaDocument10 pagesEosinophilic Bronchitis, Eosinophilic GranulomaAlejandro Estrada RiosNo ratings yet
- Conference Proceedings: Obstructive Sleep Apnea: Diagnosis, Epidemiology, and EconomicsDocument13 pagesConference Proceedings: Obstructive Sleep Apnea: Diagnosis, Epidemiology, and EconomicsMihaela-Alexandra PopNo ratings yet
- Failed Fiberoptic Intubation and Surgical Tracheostomy in A Case of Down's Syndrome With GoiterDocument3 pagesFailed Fiberoptic Intubation and Surgical Tracheostomy in A Case of Down's Syndrome With GoiterxkrautNo ratings yet
- Article PR 2Document4 pagesArticle PR 2Malak Al SayedNo ratings yet
- Word Post Extubation CareDocument19 pagesWord Post Extubation CareKanika BillaNo ratings yet
- ALS1Document4 pagesALS1Jhoana Rose Joaquin SantosNo ratings yet
- Snoring, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSnoring, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- 2016 Maxillary Arch Width and Buccal Corridor Changes With Damon andDocument6 pages2016 Maxillary Arch Width and Buccal Corridor Changes With Damon andRabia MekamchaNo ratings yet
- 2011 Effect of Extraction of First Four Premolars On Smile AestheticsDocument5 pages2011 Effect of Extraction of First Four Premolars On Smile AestheticsRabia MekamchaNo ratings yet
- 2014 Aesthetic-And-Functional-Rehabilitation-Of-Child-Using-Mock-Up-Combined-With-Stratified-TechniqueDocument4 pages2014 Aesthetic-And-Functional-Rehabilitation-Of-Child-Using-Mock-Up-Combined-With-Stratified-TechniqueRabia MekamchaNo ratings yet
- 2013 An Innovative Approach For Correction of Pseudo Class III Malocclusion With The Use of Planas Direct TracksDocument7 pages2013 An Innovative Approach For Correction of Pseudo Class III Malocclusion With The Use of Planas Direct TracksRabia MekamchaNo ratings yet
- Sharp Lc-26sb25e S Ru Lc-32sb25e Lc-42sb55s e RuDocument172 pagesSharp Lc-26sb25e S Ru Lc-32sb25e Lc-42sb55s e RuПетя СтойчеваNo ratings yet
- Gesc 112Document10 pagesGesc 112Kalpavriksha1974No ratings yet
- Defence Services Staff College, Wellington: (To Be Filled in Capital Letters As Per Matriculation (Or) X STD Mark Sheet)Document3 pagesDefence Services Staff College, Wellington: (To Be Filled in Capital Letters As Per Matriculation (Or) X STD Mark Sheet)Siddharth MuthukumarNo ratings yet
- Comprehension QuestionsDocument6 pagesComprehension Questionsapi-245567970No ratings yet
- Arnold Böcklin Was Born in Basel, Switzerland inDocument6 pagesArnold Böcklin Was Born in Basel, Switzerland inDragos PlopNo ratings yet
- Oracle E-Business Suite TechnicalDocument7 pagesOracle E-Business Suite Technicalmadhugover123No ratings yet
- SlumsDocument6 pagesSlumsRidhima Ganotra100% (1)
- Site Induction PresentationDocument17 pagesSite Induction PresentationalisyalalaNo ratings yet
- Unit 2 - Chapter 2Document20 pagesUnit 2 - Chapter 2Dennise Kate CabiedesNo ratings yet
- Design and Construction of A Variable Frequency Drive Industrial ApplicationsDocument9 pagesDesign and Construction of A Variable Frequency Drive Industrial ApplicationsMarc TcheukabaNo ratings yet
- GE1451 NotesDocument18 pagesGE1451 NotessathishNo ratings yet
- Tugas Lk7 Dan 10 Garuda PancasilaDocument5 pagesTugas Lk7 Dan 10 Garuda PancasilaarifuddinNo ratings yet
- PET ScanDocument3 pagesPET ScanChim PalmarioNo ratings yet
- Finance Management Individual AssDocument33 pagesFinance Management Individual AssDevan MoroganNo ratings yet
- Atty. SungaDocument22 pagesAtty. SungaKris MercadoNo ratings yet
- HarshadDocument61 pagesHarshadsaurabh deshmukhNo ratings yet
- 2021 Community ReportDocument28 pages2021 Community Reportapi-309161587No ratings yet
- Of Delhi in Criminal Appeal No. - of 2018)Document18 pagesOf Delhi in Criminal Appeal No. - of 2018)AnukritiNo ratings yet
- Manonmaniam Sundaranar University: B.B.A. - Ii YearDocument61 pagesManonmaniam Sundaranar University: B.B.A. - Ii YearLovely Dhanaa4848No ratings yet
- Email 1Document4 pagesEmail 1Ali AmarNo ratings yet
- Tatanka Oyate 2 EngDocument3 pagesTatanka Oyate 2 EngdesiNo ratings yet
- Operating BudgetDocument38 pagesOperating BudgetRidwan O'connerNo ratings yet
- Torres v. People (2011)Document2 pagesTorres v. People (2011)Gigi LucilleNo ratings yet