You might also like
- Ayurveda MagicDocument154 pagesAyurveda MagicGabriel Lucrezio100% (2)
- Clinical Audit ReportDocument6 pagesClinical Audit Reportjhonron100% (1)
- Breast Cancer PDFDocument12 pagesBreast Cancer PDFGabriela Zubieta100% (2)
- 4) Epidemiology of Periodontal DiseasesDocument22 pages4) Epidemiology of Periodontal Diseaseswalaa75No ratings yet
- Periodontal Changes in Ortho Treatment / Orthodontic Courses by Indian Dental AcademyDocument81 pagesPeriodontal Changes in Ortho Treatment / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- NOSODESDocument5 pagesNOSODESnamkay_tenzynNo ratings yet
- A Guide To Managing Tooth Wear The Radboud PhilosphyDocument9 pagesA Guide To Managing Tooth Wear The Radboud PhilosphyNajeeb UllahNo ratings yet
- Articulo Hospitalaria 7 PDFDocument7 pagesArticulo Hospitalaria 7 PDFJulia Rodríguez VegaNo ratings yet
- Jurnal DentistDocument8 pagesJurnal DentistAnugrah AztriNo ratings yet
- Walter 2019Document3 pagesWalter 2019Diana Choiro WNo ratings yet
- New Perio ClassificationDocument8 pagesNew Perio ClassificationLauraNo ratings yet
- Other Journals in Brief: Research InsightsDocument1 pageOther Journals in Brief: Research InsightsBagis Emre GulNo ratings yet
- Comment: Clean Up Energy InnovationDocument3 pagesComment: Clean Up Energy InnovationCesar NietoNo ratings yet
- Banerjee 2017Document8 pagesBanerjee 2017FFDFNo ratings yet
- Gingival Overgrowth: Part 1: Aetiology and Clinical DiagnosisDocument7 pagesGingival Overgrowth: Part 1: Aetiology and Clinical Diagnosiswafiqah izzatul auliahNo ratings yet
- 10 1038@sj BDJ 2016 855Document8 pages10 1038@sj BDJ 2016 855Sofia PereiraNo ratings yet
- Jurnal 35Document7 pagesJurnal 35ihsansabridrNo ratings yet
- The Oral Health of Individuals With Dental Phobia: A Multivariate Analysis of The Adult Dental Health Survey, 2009Document10 pagesThe Oral Health of Individuals With Dental Phobia: A Multivariate Analysis of The Adult Dental Health Survey, 2009Sung Soon ChangNo ratings yet
- Antibiotics - Small Molecule - Not - B - Developed d41586-020-02884-3Document3 pagesAntibiotics - Small Molecule - Not - B - Developed d41586-020-02884-3SHINDY ARIESTA DEWIADJIENo ratings yet
- Cullingham 2017Document5 pagesCullingham 2017Khanh Vũ Phương LêNo ratings yet
- Coronavirus Pandemic: Impact On The Hospitality IndustryDocument11 pagesCoronavirus Pandemic: Impact On The Hospitality IndustryDianaNo ratings yet
- Eng - PDF JsessionidDocument6 pagesEng - PDF JsessionidMuhamad FadilahNo ratings yet
- Rubber Dam May Increase The Survival Time of Dental RestorationsDocument2 pagesRubber Dam May Increase The Survival Time of Dental Restorationsjhon valdiviezoNo ratings yet
- Epidemiology of Periodontal DiseasesDocument54 pagesEpidemiology of Periodontal DiseasesAmira RadwanNo ratings yet
- Tooth Bleaching Questions AnsweredDocument12 pagesTooth Bleaching Questions AnsweredleiddyNo ratings yet
- Tahrani 2016Document27 pagesTahrani 2016Henry Leroy Lewis BatresNo ratings yet
- Failure of Eruption Central IncisorDocument7 pagesFailure of Eruption Central Incisor9fxhktdqy8No ratings yet
- Could Obesity PDFDocument2 pagesCould Obesity PDFLivia Maria ConsoliNo ratings yet
- Ray 2017Document10 pagesRay 2017Chris MartinNo ratings yet
- Other Journals in Brief: Research InsightsDocument1 pageOther Journals in Brief: Research InsightsBagis Emre GulNo ratings yet
- Adj 12747Document7 pagesAdj 12747Irfan HussainNo ratings yet
- All ChaptersDocument33 pagesAll Chaptersq24rzsxbr8No ratings yet
- Orofacial Pain - An Update On Diagnosis and Management: PracticeDocument9 pagesOrofacial Pain - An Update On Diagnosis and Management: PracticeAlex GasnasNo ratings yet
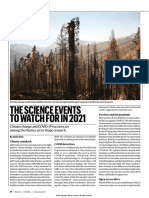
- The Science Events To Watch For in 2021Document2 pagesThe Science Events To Watch For in 2021BhumiNo ratings yet
- Articol Paro 1Document7 pagesArticol Paro 1Raluca ElenaNo ratings yet
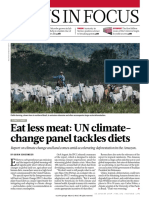
- News in Focus: Eat Less Meat: UN Climate-Change Panel Tackles DietsDocument2 pagesNews in Focus: Eat Less Meat: UN Climate-Change Panel Tackles DietsAufaNo ratings yet
- Poluarea Si BRCDocument12 pagesPoluarea Si BRCAlina Simona TeodoroviciNo ratings yet
- Potential New Therapy For OphthalmopathyDocument1 pagePotential New Therapy For OphthalmopathyEsteban Martin Chiotti KaneshimaNo ratings yet
- News in Focus: How Severe Are Omicron Infections?Document2 pagesNews in Focus: How Severe Are Omicron Infections?AMITANo ratings yet
- Why Did The Worlds Pandemic Warning System Fail When COVID 19 HitDocument2 pagesWhy Did The Worlds Pandemic Warning System Fail When COVID 19 HitGail HoadNo ratings yet
- Dens InvaginatusDocument5 pagesDens InvaginatusFatima AliNo ratings yet
- Article15 Paris Agreement Nature 2016Document9 pagesArticle15 Paris Agreement Nature 2016nzhiti20No ratings yet
- Nature - 2020 04 02Document453 pagesNature - 2020 04 02WiguelMRNo ratings yet
- Dental Practicality IndexDocument4 pagesDental Practicality Indexdorasani99No ratings yet
- (2016) Robert O. Keohane and David G. Victor - Cooperation and Discord in Global Climate PolicyDocument6 pages(2016) Robert O. Keohane and David G. Victor - Cooperation and Discord in Global Climate Policyfirmansyahmuhamad903No ratings yet
- UK Standards For Microbiology Investigations: Aesculin Hydrolysis TestDocument14 pagesUK Standards For Microbiology Investigations: Aesculin Hydrolysis TestBrendon MuriraNo ratings yet
- Atraumatic Restorative Treatment and Minimal Intervention DentistryDocument7 pagesAtraumatic Restorative Treatment and Minimal Intervention DentistryKalpanaNo ratings yet
- 2017 Systmatic ReviewDocument10 pages2017 Systmatic ReviewSara MoustafaNo ratings yet
- Research Article: Global Medical and Health CommunicationDocument5 pagesResearch Article: Global Medical and Health CommunicationPutri NoviyantiNo ratings yet
- Rafoxanide and Closantel Inhibit SPAK and OSR1 Kinases by Binding To A Highly Conserved Allosteric Site On Their C-Terminal DomainsDocument15 pagesRafoxanide and Closantel Inhibit SPAK and OSR1 Kinases by Binding To A Highly Conserved Allosteric Site On Their C-Terminal DomainsLaOde AdinNo ratings yet
- Galloway 2017Document8 pagesGalloway 2017AngelaNo ratings yet
- Impact of Electronic Cigarettes On Oral Health: A Review: Mahmoud Rouabhia, PHDDocument8 pagesImpact of Electronic Cigarettes On Oral Health: A Review: Mahmoud Rouabhia, PHDاحمد الزهرانيNo ratings yet
- 4 6016838316534531560Document373 pages4 6016838316534531560Sidarth ANo ratings yet
- 3 20Esthetic20Rehab20Ant20conoidDocument16 pages3 20Esthetic20Rehab20Ant20conoidValentinaNo ratings yet
- 2 Climate Change Through A Poverty LensDocument7 pages2 Climate Change Through A Poverty LensAngku AnazmyNo ratings yet
- Evaluation of Chlorhexidine Gluconate Mouthrinse-Induced Staining Using A Digital Colorimeter: An in Vivo StudyDocument11 pagesEvaluation of Chlorhexidine Gluconate Mouthrinse-Induced Staining Using A Digital Colorimeter: An in Vivo StudyFrontiersNo ratings yet
- Mehta, 2018Document9 pagesMehta, 2018GOOSI666No ratings yet
- B DJ Team 2018199654297Document3 pagesB DJ Team 2018199654297abhinavNo ratings yet
- Comment: How Social Media Affects Teen Mental Health: A Missing LinkDocument3 pagesComment: How Social Media Affects Teen Mental Health: A Missing LinkWilliam Hernandez GonzalezNo ratings yet
- The Hall Technique 10 Years On: Questions and Answers: GeneralDocument6 pagesThe Hall Technique 10 Years On: Questions and Answers: GeneralamilescoNo ratings yet
- Chapter 14 Lecture Notes: Nucleic Acids: Educational GoalsDocument48 pagesChapter 14 Lecture Notes: Nucleic Acids: Educational GoalsZahid Gul AsceticNo ratings yet
- Pakistan's Air Pollution ChallengeDocument8 pagesPakistan's Air Pollution ChallengeMahnoor baqaiNo ratings yet
- Glickman 2009Document8 pagesGlickman 2009Liv A. TorresNo ratings yet
- Glickman (1) - Ethical and Scientific Implications of The Globalization of Clinical Research NEJMDocument8 pagesGlickman (1) - Ethical and Scientific Implications of The Globalization of Clinical Research NEJMMaria BernalNo ratings yet
- The Biologic Width: - A Concept in Periodontics and Restorative DentistryDocument8 pagesThe Biologic Width: - A Concept in Periodontics and Restorative DentistryDrKrishna DasNo ratings yet
- Nursing Management of Oral HygieneDocument40 pagesNursing Management of Oral HygieneGrace Shabrina HapsariNo ratings yet
- Radiology SLE-770-QuestionsDocument88 pagesRadiology SLE-770-QuestionsAsif NewazNo ratings yet
- Grade 6 Health PPT WK1Document21 pagesGrade 6 Health PPT WK1Martina SantoyoNo ratings yet
- Review of The Oral Disease-Systemic Disease Link. Part I: Heart Disease, DiabetesDocument10 pagesReview of The Oral Disease-Systemic Disease Link. Part I: Heart Disease, DiabetesAristya Julianto SidhartaNo ratings yet
- Dentalcariesandpregnantwomen PDFDocument5 pagesDentalcariesandpregnantwomen PDFandreamariefdjNo ratings yet
- BP ClassperiodiseasesDocument15 pagesBP ClassperiodiseasesTikaZyka16No ratings yet
- Mouthwashes and Their Use in Different Oral ConditionsDocument6 pagesMouthwashes and Their Use in Different Oral ConditionsBagus RahmawanNo ratings yet
- Jcad 13 6 48Document6 pagesJcad 13 6 48neetika guptaNo ratings yet
- A Comparative Evaluation of An Ultrasonic and A Manual Toothbrush On The Oral Hygiene Status and Stain Removing EfficacyDocument3 pagesA Comparative Evaluation of An Ultrasonic and A Manual Toothbrush On The Oral Hygiene Status and Stain Removing EfficacyMayurNo ratings yet
- Controversies in Periodontogy. Rama. NikhatDocument121 pagesControversies in Periodontogy. Rama. NikhatDpartment of Periodontology100% (1)
- New Form PalaroDocument10 pagesNew Form PalaroRainier DoctoleroNo ratings yet
- Prevalence of Overhang Margins in Posterior Amalgam Restorations and Alveolar Bone ResorptionDocument3 pagesPrevalence of Overhang Margins in Posterior Amalgam Restorations and Alveolar Bone ResorptionNaji Z. ArandiNo ratings yet
- Laser CurettageDocument13 pagesLaser Curettageluncat2anNo ratings yet
- Chlorhexidine - An Antiseptic in PeriodonticsDocument4 pagesChlorhexidine - An Antiseptic in PeriodonticsInternational Organization of Scientific Research (IOSR)No ratings yet
- Dental Certificate 2018Document1 pageDental Certificate 2018Yrrech LaneNo ratings yet
- Clinical Evaluation of Removable Partial Dentures On The Periodontal Health of Abutment Teeth: A Retrospective StudyDocument8 pagesClinical Evaluation of Removable Partial Dentures On The Periodontal Health of Abutment Teeth: A Retrospective StudyEduard Gabriel GavrilăNo ratings yet
- Canine Periodontitis: The Dog As An Important Model For Periodontal Studies PDFDocument7 pagesCanine Periodontitis: The Dog As An Important Model For Periodontal Studies PDFludiegues752No ratings yet
- Jar Perio PedoDocument3 pagesJar Perio PedoginadrismayasariNo ratings yet
- Periodontal Disease in ChildrenDocument47 pagesPeriodontal Disease in ChildrenShahid HameedNo ratings yet
- Dental Health Record: Region XII Division of Sultan Kudarat Latest 1 1/2 X 1 1/2 PictureDocument2 pagesDental Health Record: Region XII Division of Sultan Kudarat Latest 1 1/2 X 1 1/2 PictureLimwil Dela RaizNo ratings yet
- Periodontal Diseases and Risk of Oral Cancer in Southern India: Results From The Hence Life StudyDocument8 pagesPeriodontal Diseases and Risk of Oral Cancer in Southern India: Results From The Hence Life Studyمحمد العراقيNo ratings yet
- 1.structure of The TeethDocument5 pages1.structure of The TeethCălin PavelNo ratings yet
- 2.2 Common Childhood Ailments & Taking Care of The Sense OrgansDocument18 pages2.2 Common Childhood Ailments & Taking Care of The Sense OrgansMary Christine RagueroNo ratings yet
- Epidemiology of Oral DiseasesDocument38 pagesEpidemiology of Oral DiseasesZainab MohammadNo ratings yet