You might also like
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- Macrolides: Presented by Maimoona Siddique, Mahrukh EhteshamDocument13 pagesMacrolides: Presented by Maimoona Siddique, Mahrukh EhteshamRamla NawabNo ratings yet
- Aminophylline GuidelinesDocument2 pagesAminophylline GuidelinesChristian Reza100% (1)
- Pharma URO MacrolidesDocument6 pagesPharma URO MacrolidesHussein AlhaddadNo ratings yet
- Unit:-3: Presented By: - Deepak Chandra JoshiDocument24 pagesUnit:-3: Presented By: - Deepak Chandra JoshiRahul PalsNo ratings yet
- Macrolides: Erythromycin, Clarithromycin, Azithromycin (38Document28 pagesMacrolides: Erythromycin, Clarithromycin, Azithromycin (38Shahid IqbalNo ratings yet
- MacrolidesDocument27 pagesMacrolidesAuthor Nauman Shad100% (1)
- Dr. Salman August 2004Document27 pagesDr. Salman August 2004PROF DR SHAHMURADNo ratings yet
- Macrolides: Jagir R. Patel Asst Professor Dept of PharmacologyDocument15 pagesMacrolides: Jagir R. Patel Asst Professor Dept of PharmacologyJagirNo ratings yet
- AMINOGLYCOSIDES AND MACROLIDES: MECHANISMS AND CLINICAL USESDocument45 pagesAMINOGLYCOSIDES AND MACROLIDES: MECHANISMS AND CLINICAL USESAbdullah EmadNo ratings yet
- Impact of Azithromycin on Wild Duck PlasmaDocument4 pagesImpact of Azithromycin on Wild Duck Plasmasomen mojumderNo ratings yet
- Antibiotics-2 Cology 2Document25 pagesAntibiotics-2 Cology 2Manthan ChauhanNo ratings yet
- Classification and Mechanism of Macrolides, Tetracyclines and FluoroquinolonesDocument28 pagesClassification and Mechanism of Macrolides, Tetracyclines and FluoroquinolonesH.M. PiashNo ratings yet
- Tetra, Makrolid, AminoglikosidDocument30 pagesTetra, Makrolid, AminoglikosidSarah AvecienaNo ratings yet
- MacrolidesDocument9 pagesMacrolidesAnish Kumar ANo ratings yet
- Macrolides and LincosamidesDocument22 pagesMacrolides and LincosamidesSunilNo ratings yet
- Tetracycline's: Jagir R. Patel Asst Prof Dept. Pharmacology Anand Pharmacy CollegeDocument21 pagesTetracycline's: Jagir R. Patel Asst Prof Dept. Pharmacology Anand Pharmacy CollegeJagirNo ratings yet
- Protein Synthesis InhibitorsDocument25 pagesProtein Synthesis InhibitorsSawsan Z. JwaiedNo ratings yet
- Linosamides: Jagir R. Patel Asst Prof Dept. Pharmacology Anand Pharmacy CollegeDocument9 pagesLinosamides: Jagir R. Patel Asst Prof Dept. Pharmacology Anand Pharmacy CollegeJagirNo ratings yet
- 30.IndustrialMicrobiology 102008 105579Document32 pages30.IndustrialMicrobiology 102008 105579Asif IqbalNo ratings yet
- Anti-Parasitic: Anti-Inflammatory and Anti-Infective Agents: Mechanism of Drug ActionDocument12 pagesAnti-Parasitic: Anti-Inflammatory and Anti-Infective Agents: Mechanism of Drug ActionMIKAELA DAVIDNo ratings yet
- Aminoglycosides 23099Document27 pagesAminoglycosides 23099TES SENNo ratings yet
- Antibiotics 2Document34 pagesAntibiotics 2Uzea Cezar-DanNo ratings yet
- Pharmacology I Lecture 2 (Antibiotics) : Protein Synthesis InhibitorsDocument40 pagesPharmacology I Lecture 2 (Antibiotics) : Protein Synthesis Inhibitorsعلي الفواديNo ratings yet
- NotesDocument9 pagesNotesVivianNo ratings yet
- Antibacterial Drugs: B.K. SatriyasaDocument56 pagesAntibacterial Drugs: B.K. SatriyasaVicNo ratings yet
- Drug StudyDocument5 pagesDrug StudyMadsNo ratings yet
- The Macrolide Antibiotics 1 1Document6 pagesThe Macrolide Antibiotics 1 1John PaulNo ratings yet
- Drugs Used To Treat: TuberculosisDocument46 pagesDrugs Used To Treat: TuberculosisDR AbidNo ratings yet
- MACROLIDESDocument51 pagesMACROLIDESKasturiRangan SrivatsaNo ratings yet
- Anti Protozoal P1Document5 pagesAnti Protozoal P1N Gv FcNo ratings yet
- ANTELMINTIKDocument44 pagesANTELMINTIKnovi_linggaNo ratings yet
- Tranexamic AcidDocument18 pagesTranexamic AcidFatima Love Ariate-ArcasetasNo ratings yet
- AminoglycosidesDocument36 pagesAminoglycosidesIqbal V MohammadNo ratings yet
- Newer Antibiotics: Guide: DR Saroja A ODocument51 pagesNewer Antibiotics: Guide: DR Saroja A OparahulNo ratings yet
- Azimor - 250 TabletsDocument1 pageAzimor - 250 TabletsRakesh PalNo ratings yet
- Azithromycin NMFv1.0 Full 20180620Document5 pagesAzithromycin NMFv1.0 Full 20180620Lütfiye ÖzlemNo ratings yet
- 44-45 Tetracyclines and Chloramphenicols-2023Document30 pages44-45 Tetracyclines and Chloramphenicols-2023deo okiaNo ratings yet
- ANTELMITIKDocument51 pagesANTELMITIKAsti NurjanahNo ratings yet
- Cology PageDocument4 pagesCology PageAbdulhakim ZekeriyaNo ratings yet
- All 2Document14 pagesAll 2Waseem HaiderNo ratings yet
- Farmakologi Obat Kusta Dan Antiparasit 2015Document84 pagesFarmakologi Obat Kusta Dan Antiparasit 2015Alex FerdinandNo ratings yet
- ClarithromycinDocument4 pagesClarithromycinGAYATHIRINo ratings yet
- Pyra TBDocument6 pagesPyra TBRaya Ibarra LumogdangNo ratings yet
- Macrolides and Clindamycin 2nd Year BdsDocument38 pagesMacrolides and Clindamycin 2nd Year BdsLaiba IkramNo ratings yet
- Use of Antibiotics in Periodontal TherapyDocument29 pagesUse of Antibiotics in Periodontal TherapyBibek RajNo ratings yet
- Erythromycin: Bacteriostatic, Protein-Synthesis Inhibitors That Target RibosomeDocument3 pagesErythromycin: Bacteriostatic, Protein-Synthesis Inhibitors That Target RibosomeJubelle Sipalay100% (1)
- Protein Synthesis InhibitorsDocument59 pagesProtein Synthesis InhibitorsApurba Sarker Apu100% (1)
- AminoglycosidesDocument41 pagesAminoglycosidesAshiqul IslamNo ratings yet
- Description:: Assignment On MifepristoneDocument5 pagesDescription:: Assignment On Mifepristonevenkata samyukthaNo ratings yet
- AMINOGLYCOSIDESDocument15 pagesAMINOGLYCOSIDESGareth BaleNo ratings yet
- Pharma URO AminoglycosidesDocument8 pagesPharma URO AminoglycosidesHussein AlhaddadNo ratings yet
- Antimalarial DrugsDocument45 pagesAntimalarial DrugsDeribe BekeleNo ratings yet
- Var TikaDocument16 pagesVar Tikamsbh19961995No ratings yet
- Chloramphenicol: Ayen University - Al College of PharmacyDocument7 pagesChloramphenicol: Ayen University - Al College of Pharmacyمحمد حميد عطيةNo ratings yet
- Pharmacology: Fast and Dirty Board ReviewDocument7 pagesPharmacology: Fast and Dirty Board ReviewRochelleth7278No ratings yet
- HandoutDocument17 pagesHandoutAlmalyn TimbayanNo ratings yet
- Antimalarial Drugs: Mechanisms of Action, Clinical Uses and Adverse EffectsDocument61 pagesAntimalarial Drugs: Mechanisms of Action, Clinical Uses and Adverse EffectsMewael TesfamichaelNo ratings yet
- Aminoglycosides (17.07.2017)Document44 pagesAminoglycosides (17.07.2017)Habibul Kowser (Rishat)No ratings yet
- Anti Malarial DrugsDocument42 pagesAnti Malarial DrugsSaurabh GautamNo ratings yet
- Alternative Second-Line Drugs For TuberculosisDocument42 pagesAlternative Second-Line Drugs For TuberculosisAlvin LaurenceNo ratings yet
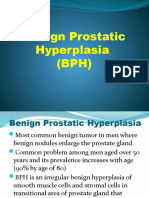
- Pharma URO BPHDocument23 pagesPharma URO BPHHussein AlhaddadNo ratings yet
- Pharma-URO-U IncontinenceDocument27 pagesPharma-URO-U IncontinenceHussein AlhaddadNo ratings yet
- Benign Prostatic Hyperplasia (BPH)Document88 pagesBenign Prostatic Hyperplasia (BPH)Hussein AlhaddadNo ratings yet
- Pharma URO MetronidazoleDocument3 pagesPharma URO MetronidazoleHussein AlhaddadNo ratings yet
- Monobactams & CarbapenemsDocument41 pagesMonobactams & CarbapenemsHussein AlhaddadNo ratings yet
- Pharma URO MetronidazoleDocument3 pagesPharma URO MetronidazoleHussein AlhaddadNo ratings yet
- Pharma URO CephalosporinsDocument20 pagesPharma URO CephalosporinsHussein AlhaddadNo ratings yet
- Pharma-URO-U IncontinenceDocument27 pagesPharma-URO-U IncontinenceHussein AlhaddadNo ratings yet
- Erythromycin: Christine Lachnit Doreen Könning Marie Liebig Patrick KlinkDocument8 pagesErythromycin: Christine Lachnit Doreen Könning Marie Liebig Patrick KlinkArnav Vikas GargNo ratings yet
- Overview of AntibioticsDocument5 pagesOverview of AntibioticsakshahinbdNo ratings yet
- Anti-Microbial Therapy Final With AlarmsDocument245 pagesAnti-Microbial Therapy Final With AlarmsMahmoud Ahmed MahmoudNo ratings yet
- BactericidalDocument15 pagesBactericidalAbdallah OmerNo ratings yet
- NCP - Drug Study - Peptic UlcerDocument18 pagesNCP - Drug Study - Peptic UlcerEmi EspinoNo ratings yet
- Esofag Kit Esomeprazole Magnesium Trihydrate Clarithromycin Amoxycillin Trihydrate - PilDocument4 pagesEsofag Kit Esomeprazole Magnesium Trihydrate Clarithromycin Amoxycillin Trihydrate - PiltseeckunNo ratings yet
- Abbott Rabeprazole PM e PDFDocument45 pagesAbbott Rabeprazole PM e PDFdonobacaNo ratings yet
- Quiz Pharmacology Part 2 of 2Document54 pagesQuiz Pharmacology Part 2 of 2MedShare92% (25)
- 1 QE Competency 1 Therapeutic MOCK Test 1 QA May 2013Document54 pages1 QE Competency 1 Therapeutic MOCK Test 1 QA May 2013Yathrika YathrikaNo ratings yet
- Drug Interactions With Antiretroviral MedicationsDocument41 pagesDrug Interactions With Antiretroviral MedicationsFajri RifaldiNo ratings yet
- Lansoprazole 15mg, 30mg Gastro-Resistant Capsules: Package Leaflet: Information For The PatientDocument2 pagesLansoprazole 15mg, 30mg Gastro-Resistant Capsules: Package Leaflet: Information For The PatientResa Eni Santi WulandariNo ratings yet
- Nursing Care Plan for a 4-Month-Old Baby with PneumoniaDocument30 pagesNursing Care Plan for a 4-Month-Old Baby with PneumoniaCharissa Magistrado De LeonNo ratings yet
- Cefuroxime, Levofloxacin, Esomeprazole, and Bismuth As First-Line Therapy For Eradicating Helicobacter Pylori in Patients Allergic To PenicillinDocument9 pagesCefuroxime, Levofloxacin, Esomeprazole, and Bismuth As First-Line Therapy For Eradicating Helicobacter Pylori in Patients Allergic To PenicillinjerryNo ratings yet
- Clarithromycin 2010 11 45 PdARDocument29 pagesClarithromycin 2010 11 45 PdARswabrijNo ratings yet
- University of Hargeisa GIT Pharmacology Review Questions: Name:aniisa Muse Ahmed Faculty:midwifery ID:1716642 Class:3ADocument4 pagesUniversity of Hargeisa GIT Pharmacology Review Questions: Name:aniisa Muse Ahmed Faculty:midwifery ID:1716642 Class:3AAniza Mouse100% (1)
- Lovastatin PDFDocument3 pagesLovastatin PDFHannaNo ratings yet
- Summary Antimicrobial Prescribing Guidance - July 21 For BNFDocument31 pagesSummary Antimicrobial Prescribing Guidance - July 21 For BNFbarcanbiancaNo ratings yet
- List of antibiotics: generic names, brands, classes and usesDocument9 pagesList of antibiotics: generic names, brands, classes and usesprince1500100% (1)
- Antibiotics ChartDocument10 pagesAntibiotics ChartTrina Si100% (6)
- Pae Emp PosterDocument1 pagePae Emp PostershaksnafeeNo ratings yet
- Last QU 24-8-2017Document21 pagesLast QU 24-8-2017ahmed masoudNo ratings yet
- ChemotherapyDocument253 pagesChemotherapyalmskein100% (1)
- Revised Drug IndexDocument76 pagesRevised Drug IndexMinette SantosNo ratings yet
- MacrolidesDocument9 pagesMacrolidesAnish Kumar ANo ratings yet
- 4-Protein Synthesis Inhibitor Antibiotics Oct 30 TH 2018Document37 pages4-Protein Synthesis Inhibitor Antibiotics Oct 30 TH 2018Leena AlateeqNo ratings yet
- Acifix: Description Drug Interactions Pharmaceutical PrecautionsDocument1 pageAcifix: Description Drug Interactions Pharmaceutical PrecautionsSaifur Rahman SuzonNo ratings yet
- Zocor Application ApprovalDocument216 pagesZocor Application ApprovalMohamed OmerNo ratings yet
- Terapie Secventiala 2Document6 pagesTerapie Secventiala 2Ionuț RusNo ratings yet
- Drug Interactions - Case StudiesDocument2 pagesDrug Interactions - Case StudiesAhmed Imran75% (4)