You might also like
- Methods in iPSC TechnologyFrom EverandMethods in iPSC TechnologyAlexander BirbrairNo ratings yet
- Comprehensive Healthcare Simulation: NeurosurgeryFrom EverandComprehensive Healthcare Simulation: NeurosurgeryAli AlarajNo ratings yet
- Fetal Birth Weight Estimation in High-Risk Pregnancies Through Machine Learning TechniquesDocument6 pagesFetal Birth Weight Estimation in High-Risk Pregnancies Through Machine Learning TechniquesGabriel Ferreira MassonNo ratings yet
- MD ThesisDocument4 pagesMD Thesisrebeccabordescambridge100% (2)
- Ensemble Deep Learning For Cervix Image SelectionDocument13 pagesEnsemble Deep Learning For Cervix Image SelectionFatihani NurqolbiahNo ratings yet
- Fetal Surgery XDocument11 pagesFetal Surgery XIoannis ValioulisNo ratings yet
- Jimaging 07 00111Document19 pagesJimaging 07 00111okuwobiNo ratings yet
- (IJCST-V10I5P47) :mrs. B. Vijaya, Bogini Naveen KumarDocument8 pages(IJCST-V10I5P47) :mrs. B. Vijaya, Bogini Naveen KumarEighthSenseGroupNo ratings yet
- 1 s2.0 S0169260722002759 MainDocument12 pages1 s2.0 S0169260722002759 MainMartaNo ratings yet
- Artificial Intelligence in Paediatric RadiologyDocument9 pagesArtificial Intelligence in Paediatric RadiologysamiaikhlefNo ratings yet
- Jurnal 3Document13 pagesJurnal 3Atikah AbayNo ratings yet
- Journal Pone 0269323Document13 pagesJournal Pone 0269323sowmiNo ratings yet
- (IJCST-V11I3P17) :yash Vishwakarma, Akhilesh A. WaooDocument8 pages(IJCST-V11I3P17) :yash Vishwakarma, Akhilesh A. WaooEighthSenseGroupNo ratings yet
- Expert-Augmented Machine Learning: SignificanceDocument7 pagesExpert-Augmented Machine Learning: SignificanceseddikNo ratings yet
- Novel Ordered SteppedWedge Cluster Trial Designs For Detecting Ebola Vaccine Efficacy Using A Spatially Structured Mathematical ModelPLoS Neglected Tropical DiseasesDocument22 pagesNovel Ordered SteppedWedge Cluster Trial Designs For Detecting Ebola Vaccine Efficacy Using A Spatially Structured Mathematical ModelPLoS Neglected Tropical Diseasescarla laureanoNo ratings yet
- An Annotated Human Blastocyst Dataset To Benchmark Deep Learning Architectures For in Vitro FertilizationDocument8 pagesAn Annotated Human Blastocyst Dataset To Benchmark Deep Learning Architectures For in Vitro Fertilizationdakc.cseNo ratings yet
- Breast CadsancersdsadsfDocument23 pagesBreast CadsancersdsadsfjohnnyNo ratings yet
- Fetal Ultrasound PlaneDocument9 pagesFetal Ultrasound Plane20D214 - IMRANA ANo ratings yet
- Literature Review On Obstetric FistulaDocument7 pagesLiterature Review On Obstetric Fistulaikofdvbnd100% (1)
- 1471-0528 15884 PDFDocument10 pages1471-0528 15884 PDFJTNo ratings yet
- Meyer 2020Document8 pagesMeyer 2020tomniucNo ratings yet
- Breast Cancer Molecular Subtype Prediction On Pathological Images With Discriminative Patch Selection and Multi-Instance LearningDocument11 pagesBreast Cancer Molecular Subtype Prediction On Pathological Images With Discriminative Patch Selection and Multi-Instance LearningPengajaran 2022No ratings yet
- Breast Cancer Diagnosis Using Artificial Neural Networks With Extreme Learning TechniquesDocument5 pagesBreast Cancer Diagnosis Using Artificial Neural Networks With Extreme Learning TechniquesfaisalNo ratings yet
- García Emilio Lymphocyte Detection Gastric Cancer PDFDocument7 pagesGarcía Emilio Lymphocyte Detection Gastric Cancer PDFFranco Roberto Lopez FernandezNo ratings yet
- JOURNALDocument4 pagesJOURNALANGELIE CRISTINE POMADONo ratings yet
- Campen EllaDocument21 pagesCampen EllaWhy BotherNo ratings yet
- Automated Early Detection of Obstetric Complications: Theoretical and Methodological ConsiderationsDocument40 pagesAutomated Early Detection of Obstetric Complications: Theoretical and Methodological ConsiderationsPenugasan PerpanjanganNo ratings yet
- Develop Med Child Neuro - 2022 - Graham - Assisted Reproductive Technology Short and Long Term OutcomesDocument12 pagesDevelop Med Child Neuro - 2022 - Graham - Assisted Reproductive Technology Short and Long Term Outcomeskadupt123No ratings yet
- Cranial Ultrasound Findings in Late Preterm Infants and Correlation With Perinatal Risk FactorsDocument7 pagesCranial Ultrasound Findings in Late Preterm Infants and Correlation With Perinatal Risk FactorsM Ibnu Rahman SyahNo ratings yet
- AI Final AssignmentDocument27 pagesAI Final AssignmentUddhav ChaliseNo ratings yet
- Prepectoralvssubpector 2023Document11 pagesPrepectoralvssubpector 2023salyouhaNo ratings yet
- (IJCST-V10I5P51) :dr. K Sailaja, T Chennakesava ReddyDocument7 pages(IJCST-V10I5P51) :dr. K Sailaja, T Chennakesava ReddyEighthSenseGroupNo ratings yet
- Applied Soft ComputingDocument21 pagesApplied Soft ComputingJuan Esteban VanegasNo ratings yet
- Prediction of Breast Cancer Using Data Mining TechniquesDocument10 pagesPrediction of Breast Cancer Using Data Mining TechniquesIAEME PublicationNo ratings yet
- Research Review of Expert Systems For Newborns: Mrs. M. K. Patkar, Dr. R.V. KulkarniDocument3 pagesResearch Review of Expert Systems For Newborns: Mrs. M. K. Patkar, Dr. R.V. KulkarniAnonymous gF0DJW10yNo ratings yet
- Pneumonia Detection Using Convolutional Neural Networks (CNNS)Document14 pagesPneumonia Detection Using Convolutional Neural Networks (CNNS)shekhar1405No ratings yet
- For Onda 2016Document8 pagesFor Onda 2016putu juniNo ratings yet
- Thesis On Breast Cancer DetectionDocument4 pagesThesis On Breast Cancer Detectionafkodkedr100% (2)
- An Approach of Cervical Cancer Diagnosis Using Class Weighting and Oversampling With KerasDocument8 pagesAn Approach of Cervical Cancer Diagnosis Using Class Weighting and Oversampling With KerasTELKOMNIKANo ratings yet
- Minor Project AnkitDocument9 pagesMinor Project Ankitankit jatNo ratings yet
- Maternal Demography and Neonatal Outcomes in Term Pre Labour Rupture of Membranes Versus Spontaneous Labour Preceding Ruptured Membranes in Lagos, Nigeria A Comparative StudyDocument6 pagesMaternal Demography and Neonatal Outcomes in Term Pre Labour Rupture of Membranes Versus Spontaneous Labour Preceding Ruptured Membranes in Lagos, Nigeria A Comparative StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- What Is The Diagnostic Value of The Babygram?: Poster No.: Congress: Type: Authors: KeywordsDocument20 pagesWhat Is The Diagnostic Value of The Babygram?: Poster No.: Congress: Type: Authors: KeywordskrisnoNo ratings yet
- Thomson Reuters Indexing JournalsDocument7 pagesThomson Reuters Indexing JournalssanaNo ratings yet
- Journal Research Paper On Reproductive PhysiologyDocument4 pagesJournal Research Paper On Reproductive Physiologygz8y0espNo ratings yet
- Deep LearningDocument6 pagesDeep Learningragou100% (1)
- Artificial Intelligence - INFORMSDocument5 pagesArtificial Intelligence - INFORMSMiguel GarcíaNo ratings yet
- Women's Critical Experiences With The Pap Smear For The Development of Cervical Cancer Screening DevicesDocument9 pagesWomen's Critical Experiences With The Pap Smear For The Development of Cervical Cancer Screening Devicesevita.irmayantiNo ratings yet
- Applying Deep Learning For Adverse Pregnancy OutcoDocument6 pagesApplying Deep Learning For Adverse Pregnancy OutcoLuck NabyiNo ratings yet
- Ariadne Report FinalDocument68 pagesAriadne Report Finalsaba.balaieNo ratings yet
- Plantilla Revista Licenciatura en F Sica UDGDocument7 pagesPlantilla Revista Licenciatura en F Sica UDGOtmane El ouardiNo ratings yet
- Breast Cancer Prediction Using Machine LearningDocument11 pagesBreast Cancer Prediction Using Machine LearningIJRASETPublicationsNo ratings yet
- Placenta y FarmacosDocument26 pagesPlacenta y FarmacosReyna HernándezNo ratings yet
- Journal Pre-Proof: Expert Systems With ApplicationsDocument42 pagesJournal Pre-Proof: Expert Systems With ApplicationsejigsonNo ratings yet
- (The Clinics - Radiology) Noam Lazebnik-Advanced Obstetrical Ultrasound - Fetal Brain, Spine, and Limb Abnormalities, An Issue of Ultrasound Clinics-Saunders (2008) PDFDocument122 pages(The Clinics - Radiology) Noam Lazebnik-Advanced Obstetrical Ultrasound - Fetal Brain, Spine, and Limb Abnormalities, An Issue of Ultrasound Clinics-Saunders (2008) PDFAndres PengNo ratings yet
- Pisa No 2007Document18 pagesPisa No 2007Daniel FerieNo ratings yet
- Inbreast PDFDocument13 pagesInbreast PDFPriyanka DattaNo ratings yet
- Breast Cancer Prediction Model With Decision Tree and Adaptive BoostingDocument7 pagesBreast Cancer Prediction Model With Decision Tree and Adaptive BoostingIAES IJAINo ratings yet
- Breast Cancer DiagnosticsDocument30 pagesBreast Cancer DiagnosticscaldevillaNo ratings yet
- Applsci 13 03211Document14 pagesApplsci 13 03211Kovid AggarwalNo ratings yet
- Imaging in Pediatric OncologyFrom EverandImaging in Pediatric OncologyStephan D. VossNo ratings yet
- Developer - RavishankarDocument5 pagesDeveloper - RavishankarmenonshyaminiNo ratings yet
- Logo Designers - 8 Best Logo Designer Gigs On FiverrDocument5 pagesLogo Designers - 8 Best Logo Designer Gigs On FiverrMien HunNo ratings yet
- ML Number PlateDocument21 pagesML Number PlateSyeda Heena KousarNo ratings yet
- Paper One: WANTED - Sale Assistant To Help in Children's Book DepartmentDocument12 pagesPaper One: WANTED - Sale Assistant To Help in Children's Book DepartmentTran LienNo ratings yet
- 55 Class (54.6 Diagonal) 1080p Smart 3D Curved OLED TVDocument52 pages55 Class (54.6 Diagonal) 1080p Smart 3D Curved OLED TVmaka153No ratings yet
- Interactive Family FeudDocument12 pagesInteractive Family FeudG04- Buatis, Ricka JeanNo ratings yet
- Creating and Managing Active Directory Groups and Organizational Units (Ous)Document16 pagesCreating and Managing Active Directory Groups and Organizational Units (Ous)Spacer GazerNo ratings yet
- Coupa Supplier Portal Admin and User GuideDocument145 pagesCoupa Supplier Portal Admin and User GuideSwarna sekhar duttaNo ratings yet
- Aminu Abdusalam: EducationDocument3 pagesAminu Abdusalam: EducationAminu AbdusalamNo ratings yet
- Spreadsheet Modeling & Decision Analysis: A Practical Introduction To Management ScienceDocument30 pagesSpreadsheet Modeling & Decision Analysis: A Practical Introduction To Management ScienceBalasubramanian GurunathanNo ratings yet
- Report On VHDL ProjectDocument47 pagesReport On VHDL ProjectVandana JainNo ratings yet
- Four Metaphors We Need To Understand Assessment: Robert J. MislevyDocument36 pagesFour Metaphors We Need To Understand Assessment: Robert J. MislevyErven Jay EscobilloNo ratings yet
- Why Are DA Files ImportantDocument3 pagesWhy Are DA Files ImportantHaftom AbadiNo ratings yet
- Upendra Reddy 2019 IOP Conf. Ser. Mater. Sci. Eng. 590 012036Document7 pagesUpendra Reddy 2019 IOP Conf. Ser. Mater. Sci. Eng. 590 012036Hastavaram Dinesh Kumar ReddyNo ratings yet
- Downloadly - Free Software DownloadDocument21 pagesDownloadly - Free Software DownloadsdsdNo ratings yet
- MX6000 Pro LED Display Controller User Manual V1.1.1Document76 pagesMX6000 Pro LED Display Controller User Manual V1.1.1Erick RiveraNo ratings yet
- Fortinet Security Fabric: Tomislav TucibatDocument31 pagesFortinet Security Fabric: Tomislav TucibatimperiaNo ratings yet
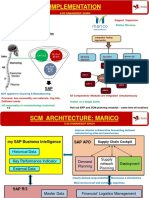
- S-55 Implementation RamandeepMarico SCMDocument2 pagesS-55 Implementation RamandeepMarico SCMSandeep KhatriNo ratings yet
- Bizhub4750 4050ServiceManual Oct.-18Document520 pagesBizhub4750 4050ServiceManual Oct.-18Luis H Real100% (3)
- Python Project Data Analysis-1Document27 pagesPython Project Data Analysis-1ripunjay080808No ratings yet
- Darkiptv - Co MACs-HitsDocument3 pagesDarkiptv - Co MACs-HitsAntónio LourençoNo ratings yet
- 10E-5 Status Signals XLRTEH4300G033850Document1 page10E-5 Status Signals XLRTEH4300G033850Miller Andres ArocaNo ratings yet
- Test Strategy: For Home Page Hotincontri - ItDocument6 pagesTest Strategy: For Home Page Hotincontri - ItAleksandar BrandicNo ratings yet
- WPL-Lab-Manual-fatima 13084Document17 pagesWPL-Lab-Manual-fatima 13084HABIBA -No ratings yet
- Blessing Komponen 29 September 2022Document251 pagesBlessing Komponen 29 September 2022dicka komsellNo ratings yet
- Replacement of Parts GantryDocument350 pagesReplacement of Parts GantryJairo Manzaneda100% (1)
- NEO 2000 /4000 Library: User GuideDocument150 pagesNEO 2000 /4000 Library: User GuideMunteanu MarianNo ratings yet
- 4 UNIT-4 Introduction To HadoopDocument154 pages4 UNIT-4 Introduction To HadoopPrakashRameshGadekarNo ratings yet
- MELNG XC-268L (ML9020814) 220V50Hz EOMDocument20 pagesMELNG XC-268L (ML9020814) 220V50Hz EOMRichard FernandezNo ratings yet