You might also like
- Solution Manual For Massage Therapy Principles and Practice 6th Edition Susan SalvoDocument37 pagesSolution Manual For Massage Therapy Principles and Practice 6th Edition Susan Salvobeastlyfulberj6gkg97% (33)
- Perioperative of ORIFDocument27 pagesPerioperative of ORIFSometwo C. Hangal91% (11)
- DX TX Iliocostal Friction Syndrome PDFDocument6 pagesDX TX Iliocostal Friction Syndrome PDFMohammad GhaniNo ratings yet
- Weir Et Al. (2019) - Approaching Groin Pain in Athletics 'The Falcon's Perspective'Document8 pagesWeir Et Al. (2019) - Approaching Groin Pain in Athletics 'The Falcon's Perspective'Tom StevensNo ratings yet
- Applied Anatomy of Joints BY DR Iram Iqbal, PG Trainee, M Phill, AnatomyDocument89 pagesApplied Anatomy of Joints BY DR Iram Iqbal, PG Trainee, M Phill, Anatomyimmmi100% (3)
- Coccydynia - An Overview of The Anatomy, Etiology, and Treatment of Coccyx PainDocument4 pagesCoccydynia - An Overview of The Anatomy, Etiology, and Treatment of Coccyx PainJose Luis Pimentel RosarioNo ratings yet
- Case Based Learning: I Hate AnatomyDocument9 pagesCase Based Learning: I Hate AnatomyHamza AhmedNo ratings yet
- 27 FullDocument8 pages27 FullTumusiime AndrewNo ratings yet
- CoccydiniaDocument9 pagesCoccydiniasamboNo ratings yet
- Clinical Examination of The Shoulder: Chapter Contents Referred PainDocument13 pagesClinical Examination of The Shoulder: Chapter Contents Referred Painvein94No ratings yet
- Maigne Jean-Yves - Management of Common Coccygodynia PDFDocument11 pagesMaigne Jean-Yves - Management of Common Coccygodynia PDFmartin jaime corralesNo ratings yet
- Lecture 4 Medical TerminologyDocument38 pagesLecture 4 Medical TerminologyAhmed KhaledNo ratings yet
- Trauma of The Coccyx and CoccygodyniaDocument4 pagesTrauma of The Coccyx and CoccygodyniaTefera LeteboNo ratings yet
- Conservative Management of Selected Shoulder ProblemsDocument8 pagesConservative Management of Selected Shoulder ProblemsDr Franklin Shoenholtz100% (3)
- ORTHODocument3 pagesORTHO24 PAULINO ALDRIN MUJARNo ratings yet
- 563 1119 1 SMDocument1 page563 1119 1 SMlukadonlicregistriranjeNo ratings yet
- LaminectomyDocument16 pagesLaminectomyNicole John C. BolanteNo ratings yet
- Diagnostic Imaging - 11 - Regional Pathologies and Evaluation - Shoulder - Elbow - Wrist - Hand - Prof - Dr.i̇smet TAMERDocument34 pagesDiagnostic Imaging - 11 - Regional Pathologies and Evaluation - Shoulder - Elbow - Wrist - Hand - Prof - Dr.i̇smet TAMERAly MssreNo ratings yet
- Research FinalDocument36 pagesResearch FinalSabaina RazaNo ratings yet
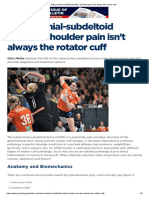
- Subacromial-Subdeltoid Bursitis - Shoulder Pain Isn't Always The Rotator CuffDocument8 pagesSubacromial-Subdeltoid Bursitis - Shoulder Pain Isn't Always The Rotator CuffAri SantosNo ratings yet
- Subacromial BursitisDocument28 pagesSubacromial BursitisRonak PatelNo ratings yet
- Shoulder Impingement SyndromeDocument37 pagesShoulder Impingement SyndromeDADDYGUS100% (1)
- Loose Bodies Tips PearlsDocument10 pagesLoose Bodies Tips PearlsGus AbellaNo ratings yet
- Help Primarysurgery32chapterthirtytwoDocument55 pagesHelp Primarysurgery32chapterthirtytwoDanisin BonzerNo ratings yet
- The Acumoxa Treatment of Shoulder Impingement SyndromeDocument8 pagesThe Acumoxa Treatment of Shoulder Impingement SyndromeAngela PagliusoNo ratings yet
- Epidemiology of Shoulder PainDocument58 pagesEpidemiology of Shoulder PainniekoNo ratings yet
- International Journal of Surgery Case ReportsDocument4 pagesInternational Journal of Surgery Case Reportsanasofia.vargas22No ratings yet
- Lecture 4 Medical Terminology PDFDocument38 pagesLecture 4 Medical Terminology PDFAhmed KhaledNo ratings yet
- Traumas of Spine and Pelvis. Done By:moldir Akynbay 17-40-01Document25 pagesTraumas of Spine and Pelvis. Done By:moldir Akynbay 17-40-01Moldir AkynbayNo ratings yet
- 4 Shoulder JointDocument50 pages4 Shoulder Jointq77gkyhzs4No ratings yet
- DISLOKASIDocument31 pagesDISLOKASIWistha MiyakiNo ratings yet
- Translate Apley SebagianDocument13 pagesTranslate Apley Sebagianstudywith kyaNo ratings yet
- Protocoale de Recuperare UmarDocument21 pagesProtocoale de Recuperare UmarKingGeorgeVIINo ratings yet
- Lesiones Del Globo OcularDocument10 pagesLesiones Del Globo OcularRulo LugoNo ratings yet
- Ankylosing SpondylitisDocument19 pagesAnkylosing SpondylitisZulhida YuniNo ratings yet
- Shoulder JointDocument30 pagesShoulder JointbalsaNo ratings yet
- Thinning Disc TMJDocument7 pagesThinning Disc TMJoktarinadyaNo ratings yet
- Seminar On Upper Limb FractureDocument166 pagesSeminar On Upper Limb FractureArko dutta100% (1)
- Myositis Ossificans (Commonly Referred To Simply As "MyositisDocument1 pageMyositis Ossificans (Commonly Referred To Simply As "MyositisMalueth AnguiNo ratings yet
- ScoliosisDocument2 pagesScoliosisZai CruzNo ratings yet
- Pott'S Disease?Document19 pagesPott'S Disease?Syarif MaulanaNo ratings yet
- 3 2 29 568 PDFDocument4 pages3 2 29 568 PDFvandraNo ratings yet
- Kuliah Kelainan PeriartikulerDocument20 pagesKuliah Kelainan PeriartikulerRoby KieranNo ratings yet
- Wrist Ganglion Cysts - Radsource PDFDocument1 pageWrist Ganglion Cysts - Radsource PDFKhalid Al maneiNo ratings yet
- Disorders of The Ankle and Subtalar JointsDocument30 pagesDisorders of The Ankle and Subtalar JointsAnonymous GzRz4H50FNo ratings yet
- "Hip Dislocation": Short CaseDocument38 pages"Hip Dislocation": Short CaseGusty BahyNo ratings yet
- HNP ReportDocument31 pagesHNP ReportChris Tine CaccamNo ratings yet
- Ankylosing SpondylitisDocument17 pagesAnkylosing Spondylitislesliejose1995No ratings yet
- دكتور ايوب OrthopaedicDocument14 pagesدكتور ايوب OrthopaedicDrAyyoub AbboodNo ratings yet
- Shoulder JointDocument37 pagesShoulder JointsandeepNo ratings yet
- Orthopedic Surgery ReviewerDocument7 pagesOrthopedic Surgery ReviewerAzria John DemetriNo ratings yet
- Problem of SpineDocument99 pagesProblem of SpineSashwini Dhevi100% (1)
- Evaluation of The Athlete With Buttock Pain: Pine OnditionsDocument8 pagesEvaluation of The Athlete With Buttock Pain: Pine OnditionsKinjal SharmaNo ratings yet
- 2014 DAY1 Shoulder BulletsDocument8 pages2014 DAY1 Shoulder Bulletsazuma12345No ratings yet
- For Reporting HNPDocument3 pagesFor Reporting HNPMicah TuringanNo ratings yet
- Gadline PrsentationDocument12 pagesGadline PrsentationsumardiNo ratings yet
- 22-Shoulder JointDocument24 pages22-Shoulder Jointnemo shNo ratings yet
- Mohd Afiq Izzuddin Bin Rossli (1001336000) (Soft Tissue Swelling) 543. 15-16Document23 pagesMohd Afiq Izzuddin Bin Rossli (1001336000) (Soft Tissue Swelling) 543. 15-16Star CruiseNo ratings yet
- Anterior Labral (Bankart) RepairsDocument13 pagesAnterior Labral (Bankart) RepairsChris CarmenNo ratings yet
- Meniscus Injury & ACL - Ligament InjuryDocument11 pagesMeniscus Injury & ACL - Ligament Injuryya shoNo ratings yet
- Coccygeal Injury, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCoccygeal Injury, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Utilization of Concurrent Dorsal Root Ganglion Stimulation and Dorsal Column Spinal Cord Stimulation in Complex Regional Pain SyndromeDocument5 pagesUtilization of Concurrent Dorsal Root Ganglion Stimulation and Dorsal Column Spinal Cord Stimulation in Complex Regional Pain Syndromemarcus moraisNo ratings yet
- Ultrasound-Guided Nerve Blocks in The Head and Neck For Chronic Pain Management - The Anatomy, Sonoanatomy, and ProcedureDocument16 pagesUltrasound-Guided Nerve Blocks in The Head and Neck For Chronic Pain Management - The Anatomy, Sonoanatomy, and Proceduremarcus moraisNo ratings yet
- Ultrasound-Guided Suprazygomatic Nerve Blocks To The Pterygopalatine Fossa - A Safe ProcedureDocument9 pagesUltrasound-Guided Suprazygomatic Nerve Blocks To The Pterygopalatine Fossa - A Safe Proceduremarcus moraisNo ratings yet
- Bilateral L1 and L2 Dorsal Root Ganglion Blocks For Discogenic Low-Back PainDocument4 pagesBilateral L1 and L2 Dorsal Root Ganglion Blocks For Discogenic Low-Back Painmarcus moraisNo ratings yet
- Anterior Cingulate Implant For Alcohol Dependence - Case ReportDocument11 pagesAnterior Cingulate Implant For Alcohol Dependence - Case Reportmarcus moraisNo ratings yet
- NDR Series Rotor PackDocument7 pagesNDR Series Rotor PackJustinNo ratings yet
- OECD in Figures - 2005 Edition - ISBN 9264013059: Economic Growth and PerformanceDocument4 pagesOECD in Figures - 2005 Edition - ISBN 9264013059: Economic Growth and PerformanceAayush ChoudhuryNo ratings yet
- Masculinity in Crisis and The Rise of ExtremismDocument3 pagesMasculinity in Crisis and The Rise of ExtremismNahida AkterNo ratings yet
- Quantum Theory of The Development of Science, Economic and Society.Document41 pagesQuantum Theory of The Development of Science, Economic and Society.Bezverkhniy VolodymyrNo ratings yet
- Trends in Computer ArchitectureDocument30 pagesTrends in Computer ArchitectureDileep KarpurNo ratings yet
- Artificial Intelligence and Cybersecurity ResearchDocument40 pagesArtificial Intelligence and Cybersecurity ResearchsaiafNo ratings yet
- Pascual CO2 PositionPaper2Document2 pagesPascual CO2 PositionPaper2Franchezcka PascualNo ratings yet
- Current Studies in Italian SyntaxDocument339 pagesCurrent Studies in Italian SyntaxGuglielmo Cinque100% (1)
- Retail Outlet Inspection Report: A. Sales & Stock 1. Totalizer ReadingsDocument6 pagesRetail Outlet Inspection Report: A. Sales & Stock 1. Totalizer ReadingsRajneesh JhoradNo ratings yet
- Driving Pressure and Survival in ARDS-Amato-ESM-NEJM 2015Document57 pagesDriving Pressure and Survival in ARDS-Amato-ESM-NEJM 2015SumroachNo ratings yet
- Start Up SOP and Check ListDocument3 pagesStart Up SOP and Check Listlets createNo ratings yet
- Bible Reading PlanDocument2 pagesBible Reading PlanbrandonsmithitNo ratings yet
- Steam Turbine Governing System: Prepared By: Nimesh GajjarDocument15 pagesSteam Turbine Governing System: Prepared By: Nimesh GajjarKr Santosh100% (1)
- Modulo FRSky FutabaFM para 2 4Document2 pagesModulo FRSky FutabaFM para 2 4AltemarFernandesdeOliveiraNo ratings yet
- Assignment Front SheetDocument17 pagesAssignment Front SheetQuynh Doan Nguyen XuanNo ratings yet
- 1-2 2002 Dec QDocument16 pages1-2 2002 Dec QSandhyaShresthaNo ratings yet
- Role of Self-Efficacy For Managing Conflict in Service SectorDocument15 pagesRole of Self-Efficacy For Managing Conflict in Service SectorSapna PremchandaniNo ratings yet
- ANTHE-2020 - (X Studying) - Code-ODocument16 pagesANTHE-2020 - (X Studying) - Code-OJiya MerjaNo ratings yet
- XII BST Case Studies-Ch-2Document12 pagesXII BST Case Studies-Ch-2Muhammad ZulqarnainNo ratings yet
- Q1Document6 pagesQ1HasanAbdullahNo ratings yet
- Klinger SealexDocument2 pagesKlinger Sealexdarsh2001patelNo ratings yet
- INTERCARGO Bulk Carrier Casualty Report - 2019Document28 pagesINTERCARGO Bulk Carrier Casualty Report - 2019Gaurav MaithilNo ratings yet
- Crystal Xp2i Manometro PatronDocument4 pagesCrystal Xp2i Manometro Patrondiana milena arredondo correaNo ratings yet
- Sun Shading DevicesDocument4 pagesSun Shading DevicesjabezNo ratings yet
- Physics Project: Poster Making On Safety Measures On LightiningDocument5 pagesPhysics Project: Poster Making On Safety Measures On LightiningRavichandran SekarNo ratings yet
- The Two Seasons of The PhilippinesDocument59 pagesThe Two Seasons of The PhilippinesZenobia Joy VillarbaNo ratings yet
- EY - How Blockchain Is Revolutionizing Supply Chain ManagementDocument8 pagesEY - How Blockchain Is Revolutionizing Supply Chain ManagementAidan Stevenson100% (1)
- Humvee 4L80 4L85 Transmission Parts Overhaul Repair NMWR 9 2520 582Document334 pagesHumvee 4L80 4L85 Transmission Parts Overhaul Repair NMWR 9 2520 582Jorge BolañosNo ratings yet
- Flange Ansi b16.5 Vs Iso 7005-2Document45 pagesFlange Ansi b16.5 Vs Iso 7005-2Allan EscobarNo ratings yet