0% found this document useful (0 votes)
690 views2 pages(2019.6) Fire Impairment Permit
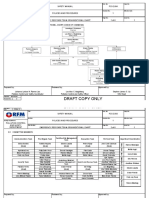
This document is a fire protection impairment permit form. It collects information about the location, system impaired, reason, dates of impairment and restoration. It also includes checklists for required actions during impairment and restoration to ensure safety precautions are followed.
Uploaded by
syamilCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
690 views2 pages(2019.6) Fire Impairment Permit
This document is a fire protection impairment permit form. It collects information about the location, system impaired, reason, dates of impairment and restoration. It also includes checklists for required actions during impairment and restoration to ensure safety precautions are followed.
Uploaded by
syamilCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd