You might also like
- Diabetes Type I & II - Cure in 72 HrsFrom EverandDiabetes Type I & II - Cure in 72 HrsRating: 3 out of 5 stars3/5 (4)
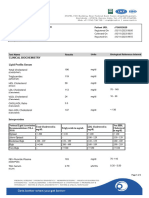
- Reference: DR - TAMIL VANNAN Mr. Sadakchar P VID: 64197775250: Lipid Profile-MiniDocument6 pagesReference: DR - TAMIL VANNAN Mr. Sadakchar P VID: 64197775250: Lipid Profile-MiniSadakchar PeriyiahNo ratings yet
- Haematology : Test Obtained Value Units Bio - Ref.IntervalsDocument3 pagesHaematology : Test Obtained Value Units Bio - Ref.Intervalsjoseph yagappanNo ratings yet
- نموذج انقاذ حياة الجديدDocument2 pagesنموذج انقاذ حياة الجديدraad_alghamdi_1No ratings yet
- Case SheetDocument9 pagesCase SheetmoghkadayanallurNo ratings yet
- Medical CertificateDocument1 pageMedical CertificateSupriyo GhoshNo ratings yet
- DownloadDocument4 pagesDownloadNemai Kumar biswasNo ratings yet
- Department of Biochemistry: Reg Number: Lab Code: Report Date: Bill DateDocument1 pageDepartment of Biochemistry: Reg Number: Lab Code: Report Date: Bill DateSudipta SahaNo ratings yet
- Format Pre EmploymentDocument10 pagesFormat Pre EmploymentNurman HidayatNo ratings yet
- Prashant Kumar MDocument3 pagesPrashant Kumar Mprashantp7819980No ratings yet
- Saras 20231105033954957Document3 pagesSaras 20231105033954957Miracle of HornbillsNo ratings yet
- Case Stud On CVADocument36 pagesCase Stud On CVAsanthyakunjumon50% (2)
- Glucose, Fasting (FBS) : Req. No: 031903144201Document17 pagesGlucose, Fasting (FBS) : Req. No: 031903144201SRIPERAMBHUDURI KRISHNANo ratings yet
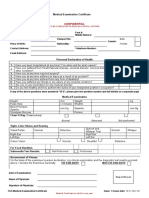
- Medical Examination Certificate: ConfidentialDocument2 pagesMedical Examination Certificate: ConfidentialVioleta100% (1)
- Pre - Employemnt Medical Test - Abhishek GurjarDocument1 pagePre - Employemnt Medical Test - Abhishek Gurjarsirohisagar0001No ratings yet
- If Claim Rejected Due To Justification Not SatisfiedDocument10 pagesIf Claim Rejected Due To Justification Not Satisfiedshivam.kumar1No ratings yet
- PHLB2047803128Document14 pagesPHLB2047803128srifbmailNo ratings yet
- 08 Jul 2023 Manipal LabReportDocument3 pages08 Jul 2023 Manipal LabReportMUKUL JANGIDNo ratings yet
- Laboratory Investigation Report::: Patient Name: Age/Sex:: Order Date Uhid: Ref. Doctor 2Document2 pagesLaboratory Investigation Report::: Patient Name: Age/Sex:: Order Date Uhid: Ref. Doctor 2tanmayNo ratings yet
- HM Medical Checkups at Project Sites Medical CampsDocument2 pagesHM Medical Checkups at Project Sites Medical Campsraj kumariNo ratings yet
- Haematology: Complete Haemogram (CBC)Document3 pagesHaematology: Complete Haemogram (CBC)Antony ThummaNo ratings yet
- General Application FormDocument2 pagesGeneral Application Formluniyayugal1No ratings yet
- Case Presentation On Coronary Artery Disease - 090908Document54 pagesCase Presentation On Coronary Artery Disease - 090908Parth Vasave100% (3)
- PPF Form Newly Edit Copy 1Document6 pagesPPF Form Newly Edit Copy 1Liana Vaal CierciNo ratings yet
- CASESHEETPHARMDDocument6 pagesCASESHEETPHARMDSai SharathNo ratings yet
- Urine Complete Examination: Colour Appearance PHDocument2 pagesUrine Complete Examination: Colour Appearance PHSeshagiri DeenadayaluNo ratings yet
- Case Study of Head Injury SijiDocument30 pagesCase Study of Head Injury SijiJinal PatelNo ratings yet
- Shailendra Tamanekar 06102022 Report-1Document2 pagesShailendra Tamanekar 06102022 Report-1Shailendra TamanekarNo ratings yet
- $ATUL SINGH01122023$10293 1 NondescriptiveDocument1 page$ATUL SINGH01122023$10293 1 Nondescriptiveaks.frf1No ratings yet
- Lipid Profile Oct 2019Document2 pagesLipid Profile Oct 2019PremNo ratings yet
- Ajab SinghDocument2 pagesAjab SinghapNo ratings yet
- Department of Haematology: Test Name Result Unit Bio. Ref. Range MethodDocument6 pagesDepartment of Haematology: Test Name Result Unit Bio. Ref. Range MethodJaya LakshmiNo ratings yet
- Medical Report Maria BenaliDocument2 pagesMedical Report Maria BenaliArisNo ratings yet
- Clinical Worksheet-Summer 08 REVISEDDocument17 pagesClinical Worksheet-Summer 08 REVISEDDaniJeanNo ratings yet
- Prashant Kumar-2Document3 pagesPrashant Kumar-2prashantp7819980No ratings yet
- Sid No. 002350: Name Mr. Suresh Kumar: Patient ID:0002148 PH: 9543278910Document1 pageSid No. 002350: Name Mr. Suresh Kumar: Patient ID:0002148 PH: 9543278910fawkesNo ratings yet
- Biochemistry: Laboratory ReportDocument4 pagesBiochemistry: Laboratory ReportChithraa KarthikNo ratings yet
- Patient Details Patient ID: Temp: BP: Weight: Height: Consultation ID: Date: Mode of Consult: Follow UpDocument1 pagePatient Details Patient ID: Temp: BP: Weight: Height: Consultation ID: Date: Mode of Consult: Follow UpSabari PramanikNo ratings yet
- PA 1 1 MergedDocument9 pagesPA 1 1 MergedMarc Mhel DalipeNo ratings yet
- BronchitisDocument24 pagesBronchitismeghana67% (3)
- Haematology: PT (Prothrombin Time)Document3 pagesHaematology: PT (Prothrombin Time)raviNo ratings yet
- DR RecordDocument10 pagesDR RecordAja Multispecialty DiagnosticNo ratings yet
- 102 MR Rajesh Kumar Nanavati: BiochemistryDocument2 pages102 MR Rajesh Kumar Nanavati: BiochemistryRajesh NanavatiNo ratings yet
- Patient Details Date: Ref No: Address: PH No.Document1 pagePatient Details Date: Ref No: Address: PH No.Rishirajsingh RathoreNo ratings yet
- Deborah BosinDocument1 pageDeborah BosinEbimoboere Teidei0% (1)
- Himalayas 2022: Medical FormDocument4 pagesHimalayas 2022: Medical FormDeepak WaradNo ratings yet
- HS Summary 1691247180118Document2 pagesHS Summary 1691247180118Siti MadihahNo ratings yet
- Preschool Health Assessment FormDocument2 pagesPreschool Health Assessment FormSammi GuptaNo ratings yet
- Medical Examination: Subang Polyclinic SDN BHDDocument5 pagesMedical Examination: Subang Polyclinic SDN BHDSubang polylinicNo ratings yet
- Medical Form Malaysian 1314Document6 pagesMedical Form Malaysian 1314A’ayisha SiddiqaNo ratings yet
- IISER Medical Report Format PDFDocument2 pagesIISER Medical Report Format PDFAnjanNo ratings yet
- Nursing Process 3Document10 pagesNursing Process 3Shubhra Sheoran100% (1)
- Medical Report Form: Weija/Gbawe Municipal Hospital Laboratory Report Sheet P.O Box ML 361 TEL. No: 0302-911965Document1 pageMedical Report Form: Weija/Gbawe Municipal Hospital Laboratory Report Sheet P.O Box ML 361 TEL. No: 0302-911965SAMMYNo ratings yet
- Interpretation: A24 - Mathura F PSC 13 C, Brij Enclave, Sonkh Adda, MATHURA, UP 281001 MathuraDocument3 pagesInterpretation: A24 - Mathura F PSC 13 C, Brij Enclave, Sonkh Adda, MATHURA, UP 281001 MathuraMohit PuriNo ratings yet
- Rekam MedisDocument44 pagesRekam Medisarfikha28No ratings yet
- 05062023MU7974RDocument2 pages05062023MU7974Rasad922No ratings yet
- Case Presentation On Coronary Artery DiseaseDocument50 pagesCase Presentation On Coronary Artery Diseasesnjv1102001No ratings yet
- Askep - Stroke Hemoragic - Ni Luh Putu Mey Ani - kdp2021Document24 pagesAskep - Stroke Hemoragic - Ni Luh Putu Mey Ani - kdp2021LuhSuandewiNo ratings yet
- Case StudyDocument21 pagesCase StudyKavi rajput100% (3)