Professional Documents
Culture Documents
Admission Form
Uploaded by
andilia9245Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Admission Form
Uploaded by
andilia9245Copyright:
Available Formats
Next of Kin / Contacts
1) Contact Person Relationship
Number where staying
Address whilst you are in hospital
Phone Number Home Business Mobile
2) Contact Person Relationship
Address Number where staying
whilst you are in hospital
"Enhancing Health
Phone Number Home Business Mobile
Payment Details through clinical excellence"
Have your hospital costs been approved by:
"Kia Rangatira ai nga Huarahi Hauora"
Medical Insurance: Name of Company
Self
Policy Number
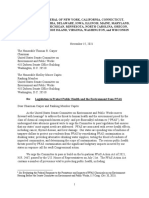
ADMISSION FORM
ACC ACC Claim No. App No.
Please complete and return seven days prior to admission to:
ACC Injury Date. . OP Code PO Box 8122, Kensington, Whangarei 0145
NDHB Personal Details
I agree that I am responsible and will pay for all costs incurred in connection with my treatment, that are not covered by
other parties (ie ACC, Medical Insurance). Overdue accounts will incur debt collection fees.
Surname First name(s) Evy
Are you on Weekly Compensation from ACC? YES NO
Preferred Name Evy Male Female Ethnicity
Date of birth Age Are you a NZ resident? YES NO
Health Information Privacy Explanation Physical Address Jl. Ir. H. Juanda No.7, Air Hitam, Kec. Samarinda Ulu, Kota Samarinda Postcode
Under the provisions of the Health Information Privacy Code 1994 there is a requirement to collect and store information about each patient to help
Postal Address Postcode
provide good and safe treatment. It is mandatory to send certain health information to other organisations such as the Ministry of Health.
Your medical records will be kept secure and will only be accessed by authorised personnel. You as a patient, have the right of access to your notes
Phone Number Home Business Mobile 081347429672
for as long as Kensington Hospital stores them. During this time, if you desire, you can update or correct your medical notes. Requests for access to
your notes should be made through our Privacy Officer. Email Address Your family Doctor
On the day of your operation until you are able to receive phone calls, our reception or nursing staff will provide callers with a general statement
regarding your health, unless advised otherwise.
If you do not wish to have any information disclosed about your stay - please inform us on admission.
Allergies/Medical Alert
If for any reason you require to be transferred to another hospital a copy of your notes from Kensington Hospital will accompany you. A copy of the
Health Information Privacy Code is available for further information if desired. Do you have allergies to medications, tablets, plasters, food, LATEX or any other substance? YES NO
If “YES” please list below.
I give permission to Kensington Hospital or any health professional involved in my care for this admission to Hospital, to access health information
about me (or my child) that is relevant to my current treatment, which may be help by Southern Cross Hospitals, other health professionals or other Substance Type of reaction Substance Type of reaction
health organisations.
If you have not received a pre-operative phone call 24 hours prior to your admission date, please contact Kensington Hospital at your
earliest convenience.
Sign here Date
Admission Details: (For office use only) Special Instructions:
Please print name Evy Hanisa Juliani Date of Operation Time : Number of Nights
NHI Number Surgeon Anaesthetist
The above details have been completed by: patient guardian relative other (specify)
Proposed surgery
LA/GA/SEDATION Day Case YES / NO IPS Bed Required YES / NO
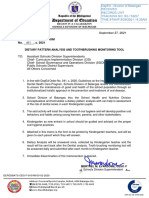
Health
Health
HealthQuestionnaire
Questionnaire
Questionnaire
Please
Please
Please
list
list
list
all
allall
previous
previous
previous
admissions
admissions
admissions
to
toto
hospital
hospital
hospital
//surgical
/surgical
surgicalprocedures:
procedures:
procedures:
Please
Please
Please
complete
complete
completethe
the
the
following
following
followingquestions.
questions.
questions.
They
They
Theyhelp
help
helpprovide
provide
provideour
our
our
staff
staff
staffwith
with
with
necessary
necessary
necessaryinformation
information
information
to
toto
assess
assess
assessyour
your
your
health
health
health
and
and
and
plan
plan
plan
your
your
yourcare.
care.
care.This
This
Thisinformation
information
informationwill
will
willremain
remain
remain
confidential
confidential
confidentialand
and
and
form
form
formpart
part
partof
ofofyour
your
your
medical
medical
medicalrecords.
records.
records.
Reason
Reason
Reasonfor
for
foradmission
admission
admission Hospital
Hospital
Hospital Year
Year
Year
Your
Your
Yourweight
weight
weight 54 kg
kg
kg Your
Your
Yourheight
height
height 1,56 metres
metres
metres
DO
DO
DOYOU
YOU
YOUHAVE
HAVE
HAVEOR
OR
ORHAVE
HAVE
HAVEYOU
YOU
YOUHAD
HAD
HADANY
ANY
ANYOF
OF
OFTHE
THE
THEFOLLOWING?
FOLLOWING?
FOLLOWING?Please
Please
Please
complete
complete
complete
all
all
all
questions
questions
questions
either
either
either
Yes
Yes
Yes
or
oror
No
NoNo
Yes
Yes
YesNo
No
No Yes
Yes
YesNo
No
No Yes
Yes
YesNo
No
No
High
High
Highblood
blood
blood
pressure
pressure
pressure Disease
Disease
Diseaseof
ofof
muscles
muscles
muscles
or
oror
nerves
nerves
nerves Have
Have
Haveyou
you
youhad
had
hadan
anan
anaesthetic
anaesthetic
anaesthetic
before?
before?
before?
Heart
Heart
Heartattack
attack
attack Malignant
Malignant
Malignanthyperthermia
hyperthermia
hyperthermia
Heart
Heart
Heartmurmurs
murmurs
murmurs Epilepsy
Epilepsy
Epilepsy General
General
Generalanaesthetic
anaesthetic
anaesthetic
Artificial
Artificial
Artificialheart
heart
heartvalve
valve
valve Blackouts/fainting
Blackouts/fainting
Blackouts/fainting Spinal/Epidural
Spinal/Epidural
Spinal/Epidural
Please
Please
Pleaselist
list all
allall
list medicines
medicines
medicines --tablets,
tablets,
- tablets,
inhalers,
inhalers,
inhalers,
patches,
patches,
patches,
etc.
etc.
etc.
prescribed
prescribed
prescribedby
byby
your
your
your
doctor
doctor
doctor
or over
over
oror over
the
the
thecounter
counter
counter(include
(include
(include
any
any
any
herbal
herbal
herbal
or
oror
natural
natural
natural
remedies
remedies
remediesor
oror
dietary
dietary
dietary
Pacemaker
Pacemaker
Pacemaker Medicines
Medicines
Medicinesfor
for
for
long
long
long
term
term
termpain
pain
pain Any
Any
Any
problems
problems
problems during
during
duringor
oror
after
after
after
supplements).
supplements).
supplements). IfIfIf
you
you
you
require
require
require more
more
more space,
space,
space, attach
attach
attach
an
anan
additional
additional
additionalsheet.
sheet.
sheet.
anaesthesia?
anaesthesia?
anaesthesia?
Chest
Chest
Chestpains
pains
pains Recreational
Recreational
Recreationaldrugs
drugs
drugs
Coronary
Coronary
Coronaryangioplasty
angioplasty
angioplasty
//stents
/stents
stents Do
DoDo
you
you
youhave
have
haveproblems
problems
problemsopening
opening
opening
Steriods
Steriods
Steriods Name
Name
Nameof
ofof
Drug
Drug
Drug Dose
Dose
Dose Frequency
Frequency
Frequency
your
your
your
mouth
mouth
mouthor
oror
with
with
with
neck
neck
neck
stiffness?
stiffness?
stiffness?
Rheumatic
Rheumatic
Rheumaticfever
fever
fever Joint
Joint
Jointimplants
implants
implants
Do
DoDo you
you
you
have
have
havedifficulty
difficulty
difficulty climbing
climbing
climbing
one
one
one
Stroke
Stroke
Stroke
//TIA
/TIA
TIA Arthritis
Arthritis
Arthritis or
oror
two
two
two
flights
flights
flights
of
ofof
stairs?
stairs?
stairs?
Irregular
Irregular
Irregular
Heart
Heart
Heart
Rate/AF
Rate/AF
Rate/AF Contact
Contact
Contactlens
lens
lens
IsIsIs
activity
activity
activity
restricted
restricted
restricted
by:
by:
by:
Hearing
Hearing
Hearingaid
aid
aid Shortness
Shortness
Shortness of
ofof
breath?
breath?
breath?
Asthma
Asthma
Asthma
Memory
Memory
MemoryProblems
Problems
Problems
eg.
eg.
eg.
dementia
dementia
dementia Chest
Chest
Chestpain?
pain?
pain?
Tuberculosis
Tuberculosis
Tuberculosis
Do
Do
Doyou
you
you
suffer
suffer
sufferfrom
from
from
anxiety?
anxiety?
anxiety? Joint
Joint
Jointpain?
pain?
pain?
Emphysema/Bronchitis
Emphysema/Bronchitis
Emphysema/Bronchitis
Do
Do
Doyou
you
you have
have
have
aahistory
ahistory
historyof
ofof
mental
mental
mental Muscle
Muscle
Musclepain?
pain?
pain?
Persistent
Persistent
Persistentcough
cough
cough health
health
healthillness?
illness?
illness?
IfIfyes,
Ifyes,
yes,please
please
please
explain
explain
explain
Does
Does
Doeslying
lying
lying
flat
flat
flat
make
make
make
you
you
you
breathless?
breathless?
breathless?
Shortness
Shortness
Shortnessof
ofof
breath
breath
breath ...............................................................................
...............................................................................
...............................................................................
Obstructive
Obstructive
Obstructivesleep
sleep
sleep
apnoea
apnoea
apnoea Do
Do Do you
you
yousmoke?
smoke?
smoke? Do
Do
Doyou
you
you
have
have
have
reflux/heartburn?
reflux/heartburn?
reflux/heartburn? Are
Are
Areyou
you
youtaking
taking
takingany
any
anyanticoagulants
anticoagulants
anticoagulantsor
oror
blood
blood
blood
thinning
thinning
thinningmedications?
medications?
medications?eg:
eg:
eg:Warfarin,
Warfarin,
Warfarin,Dabigatran,
Dabigatran,
Dabigatran,Clopidogrel,
Clopidogrel,
Clopidogrel,
Xareito,
Xareito,
Xareito,
Asprin
Asprin
Asprin
etc.
etc.
etc.
Do
Do
Doyou
you
you
have
have
have
aaCPAP
aCPAP
CPAPMachine
Machine
Machine IfIfyes,
Ifyes,
yes,how
how
howmany
many
many daily?
daily?
daily?.........................
.........................
......................... Are
Are
Areyou
you
you
or
oror
could
could
could
you
you
you
be
bebe
pregnant?
pregnant?
pregnant?
Anaemia
Anaemia
Anaemia Do
Do Do you
you
youdrink
drink
drinkalcohol?
alcohol?
alcohol? Yes
Yes
Yes No
No
No Type:
Type:
Type:.............................................................................................................................................................................................................................................
.............................................................................................................................................................................................................................................
.............................................................................................................................................................................................................................................
IfIfyes,
Ifyes,
yes,how
how
how much
much
much daily?
daily?
daily?.........................
.........................
......................... Dentures?
Dentures?
Dentures?
Bleeding
Bleeding
Bleeding
disorder
disorder
disorder Does
Does
Doesanyone
anyone
anyone
assist
assist
assist
you
you
you
with
with
with
administration
administration
administration
of
ofof
your
your
your
own
own
own
medication?
medication?
medication? Yes
Yes
Yes No
No
No
Do
Do Do you
you
youhave
have
haveany
any
anyhistory
history
historyof
ofof
falls?
falls?
falls? Have
Have
Haveyou
you
you been
been
beenin
ininaahospital
ahospital
hospital either
either
either
Blood
Blood
Blood
clots
clots
clots
IfIfyes,
Ifyes,
yes,when
when
whenwas
was
wasyour
your
yourlast
last
last
fall?
fall?
fall? in
inin
NZ
NZNZ
or
oror
overseas
overseas
overseas in
ininthe
the
thelast
last
last
66 6 IfIf‘yes’
If‘yes’
‘yes’
please
please
please
give
give
give
details:
details:
details:
..............................................................................................................................................................................................................................................................................................................
..............................................................................................................................................................................................................................................................................................................
..............................................................................................................................................................................................................................................................................................................
Blood
Blood
Blood
transfusion
transfusion
transfusion months?
months?
months?
...............................................................................
...............................................................................
............................................................................... IsIsIs
your
your
your
medication
medication
medication
packed
packed
packed
in
inin
“compliance”
“compliance”
“compliance”
(blister)
(blister)
(blister)packaging?
packaging?
packaging? Yes
Yes
Yes No
No
No
Hepatitis
Hepatitis
HepatitisAAA BB B CCC Do
Do Do you
youyou have
have
have any
anyany special
special
special ififif
YES:
YES:
YES: PLEASE
PLEASE
PLEASE
BRING
BRING
BRING
ALL
ALL
ALL
YOUR
YOUR
YOUR
MEDICATIONS,
MEDICATIONS,
MEDICATIONS,
IN
ININ
ORIGINAL
ORIGINAL
ORIGINAL
PACKETS,
PACKETS,
PACKETS,
WITH
WITH
WITH
YOU
YOU
YOU
TO
TOTO
HOSPITAL
HOSPITAL
HOSPITAL
IF
IFIF
YOU
YOU
YOU
ARE
ARE
ARE
STAYING
STAYING
STAYING
OVERNIGHT.
OVERNIGHT.
OVERNIGHT.
HIV/AIDS
HIV/AIDS
HIV/AIDS dietary
dietary
dietary requirements?
requirements?
requirements? When
When
When.....................................................................
.....................................................................
.....................................................................
Kidney/Renal
Kidney/Renal
Kidney/Renal
disease
disease
disease ...............................................................................
...............................................................................
............................................................................... Where
Where
Where...................................................................
...................................................................
................................................................... Social
Social
Social Yes
Yes
Yes No
No
No
...............................................................................
...............................................................................
............................................................................... How
How
Howlong
long
long
............................................................
............................................................
............................................................
Diabetes
Diabetes
DiabetesT1
T1T1 T2
T2T2 ...............................................................................
...............................................................................
............................................................................... Have
Have
Haveyou
you
you
ever
ever
everhad
had
hadMRSA,
MRSA,
MRSA,VRE
VRE
VREor
oror Do
Do
Doyou
you
you
use
use
use
any
any
any
mobility
mobility
mobility
aids,
aids,
aids,
ie.
ie.ie.
walking
walking
walking
frame
frame
frame
//wheelchair
/wheelchair
wheelchair//hoist?
/hoist?
hoist? TYPE:
TYPE:
TYPE:
...............................................................................................................
...............................................................................................................
...............................................................................................................
IfIfyou
Ifyou
youhave
have
havediabetes,
diabetes,
diabetes,
are
are
are
you...
you...
you... Do
DoDo
you
you
youcurrently
currently
currently have
have
have
any
any
any
skin
skin
skin ESBL
ESBL
ESBL
infection?
infection?
infection? Do
DoDo you
you
you
have
have
haveany
any
any
difficulties
difficulties
difficulties
with
with
with
any
any
any
activities
activities
activitiesof
ofof
daily
daily
daily
living
living
living
Yes
YesYesNoNoNo problems:
problems:
problems:rashes,
rashes,
rashes,
ulcers,
ulcers,
ulcers,wounds,
wounds,
wounds, Do
Do
Doyou
you
you
work
work
work
in
inin
aahealthcare
ahealthcare
healthcarefacility?
facility?
facility? e.g.
e.g.
e.g.
dressing/housework/showering?
dressing/housework/showering?
dressing/housework/showering? ififyes,
ifyes,
yes,please
please
please give
give
givefurther
further
further
details.
details.
details.
...taking
...taking
...taking
insulin?
insulin?
insulin? eczma
eczma
eczmaor
oror
boils.
boils.
boils. Have
Have
Haveyou
you
you
been
been
been in
inin
aarest
arest
rest
home
home
home or
oror ........................................................................................................................................................................................................................................................................................................................................................................
........................................................................................................................................................................................................................................................................................................................................................................
........................................................................................................................................................................................................................................................................................................................................................................
...taking
...taking
...taking
tablets?
tablets?
tablets? Has
HasHas your
your
your
doctor
doctor
doctorordered
ordered
ordered
any
any
any
tests?
tests?
tests? correctional
correctional
correctional
facility
facility
facilityin
inin
the
the
thelast
last
last
66 6 ........................................................................................................................................................................................................................................................................................................................................................................
........................................................................................................................................................................................................................................................................................................................................................................
........................................................................................................................................................................................................................................................................................................................................................................
IfIfyes,
Ifyes,
yes,what
what
what
tests?
tests?
tests? months?
months?
months?
...diet
...diet
...diet
controlled?
controlled?
controlled? Do
Do Do you
you
you currently
currently
currently
receive
receive
receive
any
any
any
community
community
community
services,
services,
services,ie.
ie.ie.
Homehelp?
Homehelp?
Homehelp?
...............................................................................
...............................................................................
............................................................................... IfIfyes,
Ifyes,
yes,please
please
please
give
give
givefurther
further
further
details.
details.
details.
IfIfyou
Ifyou
youhave
have
haveanswered
answered
answered
yes
yes
yes
to
toto
any
any
any
of
ofof
the
the
theabove,
above,
above,please
please
please
explain
explain
explain
(Details
(Details
(Detailsof
ofof
surgery/hospital
surgery/hospital
surgery/hospitaladmissions
admissions
admissionsoverleaf):
overleaf):
overleaf): ........................................................................................................................................................................................................................................................................................................................................................................
........................................................................................................................................................................................................................................................................................................................................................................
........................................................................................................................................................................................................................................................................................................................................................................
...............................................................................................................................................................................................................................................................................................................................................................
...............................................................................................................................................................................................................................................................................................................................................................
............................................................................................................................................................................................................................................................................................................................................................... Do
Do Do you
you
you have
have
have
any
any
anydependants
dependants
dependants that
that
that
need
need
need
assistance?
assistance?
assistance?
IfIfyes,
Ifyes,
yes,please
please
please
give
give
give
further
further
further
details.
details.
details.
...............................................................................................................................................................................................................................................................................................................................................................
...............................................................................................................................................................................................................................................................................................................................................................
...............................................................................................................................................................................................................................................................................................................................................................
........................................................................................................................................................................................................................................................................................................................................................................
........................................................................................................................................................................................................................................................................................................................................................................
........................................................................................................................................................................................................................................................................................................................................................................
...............................................................................................................................................................................................................................................................................................................................................................
...............................................................................................................................................................................................................................................................................................................................................................
...............................................................................................................................................................................................................................................................................................................................................................
Do
Do
Doyou
you
you
live
live
live
alone?
alone?
alone?
Do
Do
Doyou
you
you
suffer
suffer
sufferfrom
from
fromany
any
anyother
other
otherconditions
conditions
conditions not
not
notalready
already
alreadynoted,
noted,
noted,that
that
thatyou
you
you
think
think
think
we
weweshould
should
should know
know
know
about?
about?
about?Please
Please
Please
state
state
state
details
details
details
of
ofof
any
any
any
disability,
disability,
disability,
physical
physical
physical
or
oror Who
Who
Who will
will
will
care
care
care
for
for
for
you
you
you
on
onon
discharge
discharge
discharge
for
for
for
the
the
thefirst
first
first
24
2424
hours?
hours?
hours?
(must
(must
(mustbe
be
be16
1616
years
years
years
or
oror
over)
over)
over)
emotional
emotional
emotionalneeds,
needs,
needs, cultural
cultural
cultural
or
oror
spiritual
spiritual
spiritualneeds.
needs.
needs.Please
Please
Please
also
also
also
include
include
include
any
any
any
dietary
dietary
dietary
restrictions.
restrictions.
restrictions. Name:
Name:
Name:..................................................................................................................................................
..................................................................................................................................................
.................................................................................................................................................. Contact
Contact
Contactdetails:
details:
details:........................................................................................................................................................
........................................................................................................................................................
........................................................................................................................................................
...............................................................................................................................................................................................................................................................................................................................................................
...............................................................................................................................................................................................................................................................................................................................................................
...............................................................................................................................................................................................................................................................................................................................................................
Have
Have
Haveyou
you
you
arranged
arranged
arranged
someone
someone
someoneto
toto
take
take
takeyou
you
you
home
home
home
on
onon
discharge?
discharge?
discharge?
...............................................................................................................................................................................................................................................................................................................................................................
...............................................................................................................................................................................................................................................................................................................................................................
...............................................................................................................................................................................................................................................................................................................................................................
Name:
Name:
Name:..................................................................................................................................................
..................................................................................................................................................
.................................................................................................................................................. Contact
Contact
Contactdetails:
details:
details:........................................................................................................................................................
........................................................................................................................................................
........................................................................................................................................................
Do
Do
Doyou
you
you
require
require
requirean
anan
interpreter?:
interpreter?:
interpreter?:
........................................................................................................................................................................................................................................................................................
........................................................................................................................................................................................................................................................................................
........................................................................................................................................................................................................................................................................................
P.T.O
P.T.O
P.T.O
You might also like
- Claim Intimation Form: Insured InformationDocument1 pageClaim Intimation Form: Insured InformationpraveenNo ratings yet
- Health Pre-Authorization Claim FormDocument2 pagesHealth Pre-Authorization Claim Formsachin vermaNo ratings yet
- Claim Form GeneralDocument1 pageClaim Form GeneralTanya Rose-AppleNo ratings yet
- Critical Illness-Claimant's Statement - EnglishDocument2 pagesCritical Illness-Claimant's Statement - EnglishAnirudh SagaNo ratings yet
- Patient Data SheetDocument1 pagePatient Data SheetJJ LawleyNo ratings yet
- Anthem Medical Claim FormDocument2 pagesAnthem Medical Claim FormsaiprojectworkNo ratings yet
- HDFC ERGO General Insurance Company Limited: To, The Service ProviderDocument20 pagesHDFC ERGO General Insurance Company Limited: To, The Service ProviderDeepak KaushikNo ratings yet
- Pak Qatar Family Takaful Limited: Hospitalization Reimbursement Claim FormDocument1 pagePak Qatar Family Takaful Limited: Hospitalization Reimbursement Claim Formmastermind_asia9389No ratings yet
- Ci FormatDocument1 pageCi FormatGautam GogadaNo ratings yet
- Medical OpinionDocument1 pageMedical OpinionefmezahnNo ratings yet
- ENDOCRINODocument14 pagesENDOCRINOreogomezNo ratings yet
- Claim Intimation Form1307Document1 pageClaim Intimation Form1307Darbha ShaliniNo ratings yet
- Insurance Claim FormDocument9 pagesInsurance Claim FormRahmaNo ratings yet
- Patient Information SheetDocument2 pagesPatient Information SheetDavis JermacansNo ratings yet
- Mediprime: Claim FormDocument4 pagesMediprime: Claim FormMunna Bhai MbaNo ratings yet
- Registration Form PDFDocument1 pageRegistration Form PDFRaviraj PisheNo ratings yet
- Modulo Di Rimborso Spese Mediche ClaimForm-EnglishDocument2 pagesModulo Di Rimborso Spese Mediche ClaimForm-EnglishCarlo_Sturlese_4203No ratings yet
- Patient Registration 2016 NewportDocument4 pagesPatient Registration 2016 Newportapi-261541195No ratings yet
- Medical Examiner Qualifications: Please PRINT ClearlyDocument2 pagesMedical Examiner Qualifications: Please PRINT ClearlyMyedelle SeacorNo ratings yet
- Patient Admission FormDocument2 pagesPatient Admission Formelmore kakaNo ratings yet
- Patient RegistrationDocument1 pagePatient Registrationapi-547310864No ratings yet
- Medical Assistance Application Form: Office of The Vice PresidentDocument2 pagesMedical Assistance Application Form: Office of The Vice PresidentJaelieza Alejandro100% (2)
- Lucent Vis ClaimDocument2 pagesLucent Vis ClaimDanielNo ratings yet
- Attending Physician's Statement-Hospital Income BenefitDocument1 pageAttending Physician's Statement-Hospital Income BenefitVennus RacraquinNo ratings yet
- Family Health Questionnaire Form (FHQ) : Allianz EFU Health Insurance Limited Window Takaful OperationsDocument2 pagesFamily Health Questionnaire Form (FHQ) : Allianz EFU Health Insurance Limited Window Takaful OperationsnomiabbasiNo ratings yet
- Out-Patient Claim Form - ALC5894A 050717Document4 pagesOut-Patient Claim Form - ALC5894A 050717paijuanoNo ratings yet
- Reimbursement Claim FormDocument1 pageReimbursement Claim FormmoinuNo ratings yet
- Revised - Med Assistance Form - With CNDocument3 pagesRevised - Med Assistance Form - With CNchristine vizcondeNo ratings yet
- Admed Claimant'S Statement: A. Personal DetailsDocument2 pagesAdmed Claimant'S Statement: A. Personal Detailsshemina armorerNo ratings yet
- Invitae - TRF938 Invitae FVT VUS OrderFormDocument2 pagesInvitae - TRF938 Invitae FVT VUS OrderFormMs.BluMoon SageNo ratings yet
- Health Claim Form: Part A (To Be Filled by Insured)Document3 pagesHealth Claim Form: Part A (To Be Filled by Insured)Harshad DhodiNo ratings yet
- Case Questionnaire COVID-19 (Novel Coronavirus) - Part A: InformationDocument11 pagesCase Questionnaire COVID-19 (Novel Coronavirus) - Part A: InformationHenrietta CookNo ratings yet
- MCME ADM 396 0-Registration-Form-EditableDocument2 pagesMCME ADM 396 0-Registration-Form-EditableCheyma AitmansourNo ratings yet
- Commercial Prescription Drug Claim Form For Member Reimbursement Claim Form InstructionsDocument5 pagesCommercial Prescription Drug Claim Form For Member Reimbursement Claim Form InstructionsGUILLERMO CUETONo ratings yet
- Walters Shameka 46370 MedicaidrecertappDocument4 pagesWalters Shameka 46370 Medicaidrecertappdoenyka.lewisNo ratings yet
- Template Contoh Master DataDocument104 pagesTemplate Contoh Master DataHenny PurwasariNo ratings yet
- Pre Assessment Request Form 2021Document3 pagesPre Assessment Request Form 2021Joseph MogorosiNo ratings yet
- Patient Agency Agreement - Inservio Home (v2)Document3 pagesPatient Agency Agreement - Inservio Home (v2)AlcyoneSpiralNo ratings yet
- MET - Medical Claim Reimbursement Form in Patient - KWTDocument2 pagesMET - Medical Claim Reimbursement Form in Patient - KWTangeloriondo1217No ratings yet
- Blob ServerDocument2 pagesBlob Servermrraj69No ratings yet
- Insurance Form For HealthDocument2 pagesInsurance Form For Healthyaserkz1999No ratings yet
- Welcome Rev2Document2 pagesWelcome Rev2Adam C. Price100% (1)
- Inbound 2401892485776729288Document3 pagesInbound 2401892485776729288Elrym BanuaNo ratings yet
- Last Attending Physician Statement Death Claim Ver 2.0Document1 pageLast Attending Physician Statement Death Claim Ver 2.0creedlxdNo ratings yet
- Outpatient ClaimDocument1 pageOutpatient Claimtajuddin8No ratings yet
- Pediatric Patient Registration Form TemplateDocument5 pagesPediatric Patient Registration Form TemplateHasfi YakobNo ratings yet
- PatientDataSheet 08032017150005 292Document2 pagesPatientDataSheet 08032017150005 292Argel Hanzon NietesNo ratings yet
- Pre Authorization FormDocument1 pagePre Authorization FormKhuda BukshNo ratings yet
- Medicare Insurance Claim Form: PolicyholderDocument2 pagesMedicare Insurance Claim Form: PolicyholdertagashiiNo ratings yet
- Medical Insurance Hospitalization Surgical Claim FormDocument6 pagesMedical Insurance Hospitalization Surgical Claim FormMartin Stephan100% (1)
- Submission PDFDocument5 pagesSubmission PDFiete MartinsNo ratings yet
- C&a Consent FormsDocument28 pagesC&a Consent Formsjgcj477rh9No ratings yet
- Bupa Global Reimbursement FormDocument5 pagesBupa Global Reimbursement Formshena0% (1)
- Hospital-Bill-Form DDocument2 pagesHospital-Bill-Form Ddeharemmanuel64No ratings yet
- Crisis Cover Kids Claim FormDocument16 pagesCrisis Cover Kids Claim FormHihiNo ratings yet
- Reliancegeneral - Co.in 1800 3009 4890 3009: Health Claim FormDocument4 pagesReliancegeneral - Co.in 1800 3009 4890 3009: Health Claim FormSumit BhallaNo ratings yet
- Claim Form Regency For Expats PDFDocument2 pagesClaim Form Regency For Expats PDFChris DarkNo ratings yet
- Medicare ClaimDocument2 pagesMedicare Claimpimnattha2525No ratings yet
- What Your Doctor Wants You to Know to Crush Medical Debt: A Health System Insider's 3 Steps to Protect Yourself from America's #1 Cause of BankruptcyFrom EverandWhat Your Doctor Wants You to Know to Crush Medical Debt: A Health System Insider's 3 Steps to Protect Yourself from America's #1 Cause of BankruptcyNo ratings yet
- Covid-19 Vaccination Microplan Date - (06-05-2021) District: Kanpur NagarDocument4 pagesCovid-19 Vaccination Microplan Date - (06-05-2021) District: Kanpur NagarAditi GuptaNo ratings yet
- Pfas Letter To Epw 11.15.2021Document10 pagesPfas Letter To Epw 11.15.2021WXMINo ratings yet
- Lab Dept/Section: Microbiology/Virology Test Name: Sputum Culture and Gram StainDocument4 pagesLab Dept/Section: Microbiology/Virology Test Name: Sputum Culture and Gram StainAdn crnNo ratings yet
- Covid 19 Aerosol Generating ProceduresDocument4 pagesCovid 19 Aerosol Generating ProceduresAhmed Ben BellaNo ratings yet
- Division-Memorandum s2021 461Document3 pagesDivision-Memorandum s2021 461Jalene E. ObradorNo ratings yet
- Recent Advances in Orthognathic SurgeryDocument5 pagesRecent Advances in Orthognathic Surgerypedroalmeida37920No ratings yet
- TEJASWINIDocument8 pagesTEJASWINIAyush JamwalNo ratings yet
- GoodDocument7 pagesGoodana9filimonNo ratings yet
- Mo Sobhy Academy Procedures 2022 NoteDocument37 pagesMo Sobhy Academy Procedures 2022 NoteisraaobaidyNo ratings yet
- Deep Learning: COMP 5329Document32 pagesDeep Learning: COMP 5329朱宸烨No ratings yet
- Signs and Symptoms: Hyperthermia Is An Elevated Body Temperature Due To FailedDocument6 pagesSigns and Symptoms: Hyperthermia Is An Elevated Body Temperature Due To FailedbabykhoNo ratings yet
- Approach To The Adult With Nausea and Vomiting - UpToDateDocument20 pagesApproach To The Adult With Nausea and Vomiting - UpToDateJolien JobsNo ratings yet
- 10.1007@s43450 020 00090 WDocument15 pages10.1007@s43450 020 00090 WauriNo ratings yet
- Galmet Rustpaint Aerosol All Colours Except Silver - ITW Polymers & FluidsDocument9 pagesGalmet Rustpaint Aerosol All Colours Except Silver - ITW Polymers & FluidsBiju_PottayilNo ratings yet
- Learning More About Personal and Mental HealthDocument4 pagesLearning More About Personal and Mental HealthJoan VecillaNo ratings yet
- Article Bladder RetrainingDocument9 pagesArticle Bladder RetrainingRaenette DavidNo ratings yet
- 高等学校研究生英语系列教材 综合教程(上)主编熊海虹 教学课件 Unit 1Document129 pages高等学校研究生英语系列教材 综合教程(上)主编熊海虹 教学课件 Unit 1yvaineNo ratings yet
- Teeth SelectionDocument77 pagesTeeth SelectionAnurag AgarwalNo ratings yet
- Bahasa Inggris Kelompok SyahdanDocument11 pagesBahasa Inggris Kelompok SyahdanAji cupleeNo ratings yet
- Dental CariesDocument8 pagesDental CariesThe KittyNo ratings yet
- GHR Health and Nutrition Capacity Statement 2023Document5 pagesGHR Health and Nutrition Capacity Statement 2023Andre TorresNo ratings yet
- Zoonoses and Emerging Livestock Systems (ZELS) Supplementary Research Projects 2019-2021Document7 pagesZoonoses and Emerging Livestock Systems (ZELS) Supplementary Research Projects 2019-2021dukegarrikNo ratings yet
- Development and Preliminary Evaluation of PsychomeDocument11 pagesDevelopment and Preliminary Evaluation of Psychomerosa azizahNo ratings yet
- DrowningDocument9 pagesDrowningCarlos Alberto Torres LópezNo ratings yet
- A. Complete Blood Count (CBC)Document6 pagesA. Complete Blood Count (CBC)raul nino MoranNo ratings yet
- 2019 EMOP Diagnóstico y ManejoDocument8 pages2019 EMOP Diagnóstico y ManejoJeff Daniel Landauro PanayNo ratings yet
- CrisisDocument35 pagesCrisisPbNo ratings yet
- Be It Enacted by The Senate and House of Representatives of The Philippine Congress AssembledDocument4 pagesBe It Enacted by The Senate and House of Representatives of The Philippine Congress AssembledanonNo ratings yet
- Anatomy of Cardio Vascular System NotesDocument16 pagesAnatomy of Cardio Vascular System NotesAgleema AhmedNo ratings yet
- Prescription Potential ForDocument66 pagesPrescription Potential ForSuhas IngaleNo ratings yet