You might also like
- Arduino Programming Step by Step Guide To Mastering Arduino Hardware and SoftwareDocument109 pagesArduino Programming Step by Step Guide To Mastering Arduino Hardware and SoftwareMohan100% (3)
- X-Ray Generator Communication User's Manual - V1.80 L-IE-4211Document66 pagesX-Ray Generator Communication User's Manual - V1.80 L-IE-4211Marcos Peñaranda TintayaNo ratings yet
- Map Project Rubric 2018Document2 pagesMap Project Rubric 2018api-292774341No ratings yet
- D41P-6 Kepb002901Document387 pagesD41P-6 Kepb002901LuzioNeto100% (1)
- Public OpinionDocument7 pagesPublic OpinionSona Grewal100% (1)
- IT-02 Residential StatusDocument26 pagesIT-02 Residential StatusAkshat GoyalNo ratings yet
- Social Determinants of HealthDocument27 pagesSocial Determinants of HealthDensearn Seo100% (5)
- Why it's important to guard your free timeDocument2 pagesWhy it's important to guard your free timeLaura Camila Garzón Cantor100% (1)
- Ed Brown CatalogDocument44 pagesEd Brown CatalogssnvetNo ratings yet
- 7 - NIBL - G.R. No. L-15380 Wan V Kim - DigestDocument1 page7 - NIBL - G.R. No. L-15380 Wan V Kim - DigestOjie SantillanNo ratings yet
- Health Care ProjectDocument69 pagesHealth Care ProjectAvtaar SinghNo ratings yet
- Primary Healthcare in India: Coverage and Quality Issues: September 2015Document40 pagesPrimary Healthcare in India: Coverage and Quality Issues: September 2015ALEN AUGUSTINENo ratings yet
- Financing Health Improvements in IndiaDocument13 pagesFinancing Health Improvements in IndiaBhavesh JainNo ratings yet
- 4-Public - Health - Expenditure - and - Health NigeriaDocument7 pages4-Public - Health - Expenditure - and - Health NigeriaMohsin RazaNo ratings yet
- Feb 19-Lumping of Health PolicyDocument12 pagesFeb 19-Lumping of Health PolicyAnagha LokhandeNo ratings yet
- A Study On Public Expenditure On Health Sector in IndiaDocument8 pagesA Study On Public Expenditure On Health Sector in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- PH7017 Theories and Principles of Public HealthDocument26 pagesPH7017 Theories and Principles of Public HealthAndy WinchesterNo ratings yet
- The Importance of Healthy Human Life On Economic DevelopmentDocument6 pagesThe Importance of Healthy Human Life On Economic DevelopmentRahul TambiNo ratings yet
- Pakistan's Health Care Under Structural Adjustment Nina GeraDocument23 pagesPakistan's Health Care Under Structural Adjustment Nina GeraSuman ValeechaNo ratings yet
- Rajiv Mishra 3Document32 pagesRajiv Mishra 3Mayank GandhiNo ratings yet
- Health and Economic Development: Linkage and ImpactDocument21 pagesHealth and Economic Development: Linkage and ImpactDora SimmonsNo ratings yet
- National Health Policy, 2017: Revealing Public Health ChicaneryDocument12 pagesNational Health Policy, 2017: Revealing Public Health ChicaneryRohan RegiNo ratings yet
- Arun Kumar MalikDocument20 pagesArun Kumar MalikBla BlaNo ratings yet
- Key Issues in Bangladesh's Health GovernanceDocument15 pagesKey Issues in Bangladesh's Health GovernanceAhmad RonyNo ratings yet
- Investigating The Effect of Government Health Expenditure On HDI in IranDocument13 pagesInvestigating The Effect of Government Health Expenditure On HDI in IranFatria AkbarNo ratings yet
- Health Care Status in IndiaDocument46 pagesHealth Care Status in Indialucky prajapatiNo ratings yet
- Gha 6 19650Document10 pagesGha 6 19650Betric HanNo ratings yet
- Governance Frameworks for Gender Mainstreaming in Public HealthDocument10 pagesGovernance Frameworks for Gender Mainstreaming in Public HealthFika Nur FadhilahNo ratings yet
- Health Infrastucture in IndiaDocument8 pagesHealth Infrastucture in IndiaBinit kumarNo ratings yet
- The Trend of Health Expenditure in India and Odisha and Its Relationship With Health StatusDocument5 pagesThe Trend of Health Expenditure in India and Odisha and Its Relationship With Health Statusकुमार सौरभNo ratings yet
- Literature Review of Quality of Healthcare Services in IndiaDocument27 pagesLiterature Review of Quality of Healthcare Services in IndiaMunnangi NagendrareddyNo ratings yet
- Medical-Tourism in IndiaDocument103 pagesMedical-Tourism in IndiaSunil KulkarniNo ratings yet
- Health Status of IndiaDocument10 pagesHealth Status of IndiaSutapa PawarNo ratings yet
- Government's Policy on Public HealthDocument30 pagesGovernment's Policy on Public HealthKrittika PatelNo ratings yet
- Community Health Insurance Schemes Improve Access for PoorDocument10 pagesCommunity Health Insurance Schemes Improve Access for PoorMridul PantNo ratings yet
- Public Health Care System in IndiaDocument5 pagesPublic Health Care System in IndiaPela KqbcgrlaNo ratings yet
- Mgejwa's Final ResearchDocument53 pagesMgejwa's Final ResearchJohn Samson MgejwaNo ratings yet
- Health Care Guide Provides Overview of Systems and ForecastsDocument203 pagesHealth Care Guide Provides Overview of Systems and ForecastsNiro ThakurNo ratings yet
- FICCI EY Report Healthcare ReportDocument72 pagesFICCI EY Report Healthcare Reportsh_niravNo ratings yet
- Need of Public Health For Sustainable DevelopmentDocument2 pagesNeed of Public Health For Sustainable DevelopmentAdvanced Research PublicationsNo ratings yet
- Reasons For Development of Health Care in IndiaDocument5 pagesReasons For Development of Health Care in IndiasnehapriyaNo ratings yet
- Challenges For Health Care Services in Bangladesh: An OverviewDocument12 pagesChallenges For Health Care Services in Bangladesh: An OverviewAsora Yasmin snehaNo ratings yet
- Amartya Sen - Art of MedicineDocument2 pagesAmartya Sen - Art of MedicineHaalumNo ratings yet
- Health Care and EquityDocument11 pagesHealth Care and Equityprateek_10No ratings yet
- Global HealthDocument3 pagesGlobal HealthDinda ElahmadiNo ratings yet
- India's National Health Policy and National Rural Health MissionDocument4 pagesIndia's National Health Policy and National Rural Health MissionrajatsgrNo ratings yet
- Health Insurance in IndiaDocument11 pagesHealth Insurance in IndiaUpender DhullNo ratings yet
- Demand For HealthDocument12 pagesDemand For HealthJoe MuzururaNo ratings yet
- Health Care Services in India: Problems and Prospects: B. S. Ghuman Akshat MehtaDocument15 pagesHealth Care Services in India: Problems and Prospects: B. S. Ghuman Akshat MehtaPaul PriyarajNo ratings yet
- The Impacts of Health and Education Components of Human Resources Development On Poverty Level in Nigeria, 1980-2013.Document6 pagesThe Impacts of Health and Education Components of Human Resources Development On Poverty Level in Nigeria, 1980-2013.IOSRjournalNo ratings yet
- Comparative Study of Public and Private Health Services in Mumbai RegionDocument18 pagesComparative Study of Public and Private Health Services in Mumbai RegionJobin BabuNo ratings yet
- Chapter - 1 Nature, Scope, Objectives and Methodology of ResearchDocument18 pagesChapter - 1 Nature, Scope, Objectives and Methodology of ResearchJobin BabuNo ratings yet
- Chapter - 1 Nature, Scope, Objectives and Methodology of ResearchDocument18 pagesChapter - 1 Nature, Scope, Objectives and Methodology of ResearchMohammad MudasirNo ratings yet
- Chapter - 1 Nature, Scope, Objectives and Methodology of ResearchDocument18 pagesChapter - 1 Nature, Scope, Objectives and Methodology of ResearchJobin BabuNo ratings yet
- Chapter - 1 Nature, Scope, Objectives and Methodology of ResearchDocument18 pagesChapter - 1 Nature, Scope, Objectives and Methodology of ResearchJobin BabuNo ratings yet
- 04-Health Insurance in India - What Do We Know and Why Is Ethnographic Research NeededDocument24 pages04-Health Insurance in India - What Do We Know and Why Is Ethnographic Research Neededmeljo johnNo ratings yet
- Healthcare Financing in South-East Asia: Does Fiscal Capacity Matter?Document11 pagesHealthcare Financing in South-East Asia: Does Fiscal Capacity Matter?DoctorRonZ7No ratings yet
- Health Care Expenditure, Health Status and National Productivity in Nigeria (1999-2012)Document15 pagesHealth Care Expenditure, Health Status and National Productivity in Nigeria (1999-2012)Samson SeiduNo ratings yet
- Public and Private Expenditures On Health in A Growth Model JSDDocument17 pagesPublic and Private Expenditures On Health in A Growth Model JSDAnonymous qfU34ZNo ratings yet
- Public Health-Its RegulationDocument12 pagesPublic Health-Its RegulationAreeb AhmadNo ratings yet
- Uzbekistan and Philippines Healthcare Systems ComparedDocument8 pagesUzbekistan and Philippines Healthcare Systems ComparedbnvjNo ratings yet
- Health Insurance in India What Do We Know and Why Is Ethnographic Research NeededDocument24 pagesHealth Insurance in India What Do We Know and Why Is Ethnographic Research Neededankita2004nishadNo ratings yet
- Reviewv 2 I 1Document4 pagesReviewv 2 I 1Asim MahatoNo ratings yet
- Social Determinants of Health and Theories - EditedDocument5 pagesSocial Determinants of Health and Theories - EditedSamuel WachochoNo ratings yet
- Health Systems 2009 20aug ADocument74 pagesHealth Systems 2009 20aug ANational Child Health Resource Centre (NCHRC)No ratings yet
- ENG102 ProjectDocument4 pagesENG102 Project2221634No ratings yet
- Efficacy, Effectiveness And Efficiency In The Management Of Health SystemsFrom EverandEfficacy, Effectiveness And Efficiency In The Management Of Health SystemsNo ratings yet
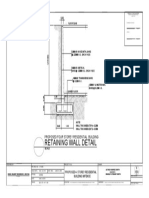
- Retaining Wall DetailsDocument1 pageRetaining Wall DetailsWilbert ReuyanNo ratings yet
- INSYS - EBW Serie EbookDocument4 pagesINSYS - EBW Serie EbookJorge_Andril_5370No ratings yet
- Basic Facts in EventDocument1 pageBasic Facts in EventAllan AgpaloNo ratings yet
- St. Anthony College Calapan City Syllabus: Course DescriptionDocument6 pagesSt. Anthony College Calapan City Syllabus: Course DescriptionAce HorladorNo ratings yet
- MFC-L2710DW 2Document8 pagesMFC-L2710DW 2Pinto ModakNo ratings yet
- Cisco Series SWCFG Xe 16 12 XDocument416 pagesCisco Series SWCFG Xe 16 12 XWagner SantiagoNo ratings yet
- MKTG 2126 - Assignment 3Document2 pagesMKTG 2126 - Assignment 3omar mcintoshNo ratings yet
- CB4 BBC Interviews EXTRA UnitDocument1 pageCB4 BBC Interviews EXTRA UnitCristianNo ratings yet
- Lesson 2Document10 pagesLesson 2angeliquefaithemnaceNo ratings yet
- Transformers Obj Questions PDFDocument8 pagesTransformers Obj Questions PDFphaniputta100% (2)
- Design and Analysis of Buck ConverterDocument18 pagesDesign and Analysis of Buck Converterk rajendraNo ratings yet
- DataSheet IMA18-10BE1ZC0K 6041793 enDocument8 pagesDataSheet IMA18-10BE1ZC0K 6041793 enRuben Hernandez TrejoNo ratings yet
- JMPRTraininga I5545e PDFDocument500 pagesJMPRTraininga I5545e PDFmvptoxNo ratings yet
- TLM4ALL@1 Number System (EM)Document32 pagesTLM4ALL@1 Number System (EM)jkc collegeNo ratings yet
- YlideDocument13 pagesYlidePharaoh talk to youNo ratings yet
- Etherpad Text-Based TutorialDocument5 pagesEtherpad Text-Based Tutorialapi-437836861No ratings yet
- Classification of AnimalsDocument6 pagesClassification of Animalsapi-282695651No ratings yet
- Manual PDFDocument9 pagesManual PDFRuth ResuelloNo ratings yet
- All Creatures Great and SmallDocument4 pagesAll Creatures Great and SmallsaanviranjanNo ratings yet
- Power System Analysis and Design, SI EditionDocument5 pagesPower System Analysis and Design, SI EditionAkimeNo ratings yet
- IBM TS2900 Tape Autoloader RBDocument11 pagesIBM TS2900 Tape Autoloader RBLeonNo ratings yet