You might also like
- Liberty Income Protector Claim FormDocument18 pagesLiberty Income Protector Claim FormMuniba DienieNo ratings yet
- New Patient Information Form 2Document2 pagesNew Patient Information Form 2Marcela CamposNo ratings yet
- Vetting Request FormDocument4 pagesVetting Request Formjafari100% (1)
- Ip Application Form and Consents Jan 2019Document5 pagesIp Application Form and Consents Jan 2019hajimuktar66No ratings yet
- Registering As A Dentist With The General Dental Council (EU/EEA/Switzerland)Document14 pagesRegistering As A Dentist With The General Dental Council (EU/EEA/Switzerland)Georgia SkopelitiNo ratings yet
- Uapom-Fs Brokerage Kyc FormDocument7 pagesUapom-Fs Brokerage Kyc FormMugabi EltonbenNo ratings yet
- Allianz claim formDocument2 pagesAllianz claim formCarlo_Sturlese_4203No ratings yet
- Claim Form en Nov 08Document4 pagesClaim Form en Nov 08Juju FernsNo ratings yet
- International Student Application Form: Section 1: Membership DetailsDocument3 pagesInternational Student Application Form: Section 1: Membership DetailsBrilliant MycriNo ratings yet
- Guide to British Naturalisation ApplicationDocument44 pagesGuide to British Naturalisation ApplicationadobiNo ratings yet
- OCC Complaint FormDocument5 pagesOCC Complaint FormTim BryantNo ratings yet
- Deedpol Form UKDocument10 pagesDeedpol Form UKmwananzambi1850No ratings yet
- Inter Global Claim Form 2010Document4 pagesInter Global Claim Form 2010ywa00No ratings yet
- OneFamily - Claim FormDocument4 pagesOneFamily - Claim FormBell-Winn-Cal- Victoria-londonNo ratings yet
- Beltinge & District Funeral Services Booklet 2017Document9 pagesBeltinge & District Funeral Services Booklet 2017Anonymous kuAyJ6mNo ratings yet
- Unit Trust Account Opening Form 13.12.2019 1Document4 pagesUnit Trust Account Opening Form 13.12.2019 1henrykibe01No ratings yet
- Questionnaire 2013Document8 pagesQuestionnaire 2013api-207389485No ratings yet
- GMHP Claim Form - Online PDFDocument4 pagesGMHP Claim Form - Online PDFSalem AmraneNo ratings yet
- Notice of Appeal - Form SSCS1Document16 pagesNotice of Appeal - Form SSCS1AmbroseNo ratings yet
- CORADocument3 pagesCORANaveenNo ratings yet
- Self Certifications PDFDocument2 pagesSelf Certifications PDFAhmed Issah100% (1)
- ReligareDocument2 pagesReligareAnonymous nx6TUjNP4No ratings yet
- Health Statement FormDocument2 pagesHealth Statement FormRose Ann DuqueNo ratings yet
- 3S Claimant'S Statement Form (Death Claims) : (Mandatory)Document4 pages3S Claimant'S Statement Form (Death Claims) : (Mandatory)Sachin ShingoteNo ratings yet
- Ann18743 (717) 68706Document10 pagesAnn18743 (717) 68706GustaveFlaubertNo ratings yet
- BAH Bupa Global Claim Form EN APR21 0027975Document8 pagesBAH Bupa Global Claim Form EN APR21 0027975ALJABERNo ratings yet
- Claim form submission made simpleDocument7 pagesClaim form submission made simpleEduskill Learning CentreNo ratings yet
- 2902467-Guide AN v1 0Document27 pages2902467-Guide AN v1 0vidhyaa1011No ratings yet
- Pple Group - Application Form Care Workers Ver202107Document16 pagesPple Group - Application Form Care Workers Ver202107Thobeka NtuliNo ratings yet
- Treasury Bond Claim Form Sav1048Document7 pagesTreasury Bond Claim Form Sav1048aplaw100% (1)
- Ableliving Application FormDocument5 pagesAbleliving Application FormBezimeni BezimenovicNo ratings yet
- SBCAOpenForm Karnatka BankDocument7 pagesSBCAOpenForm Karnatka BankMirtunjay KumarNo ratings yet
- Patient's Details (To Be Completed by The Patient) : This Form Allows Us ToDocument3 pagesPatient's Details (To Be Completed by The Patient) : This Form Allows Us ToVivek Jung HamalNo ratings yet
- One Account Application DocumentsDocument7 pagesOne Account Application DocumentsjsinnNo ratings yet
- Bupa International Claim Form: 1 Patient'S DetailsDocument4 pagesBupa International Claim Form: 1 Patient'S DetailsRealty SolutionsNo ratings yet
- Revctel Smi (Ed)Document3 pagesRevctel Smi (Ed)bobriley070No ratings yet
- AUS Bupa Global Claim Form EN APR21 0028299Document8 pagesAUS Bupa Global Claim Form EN APR21 0028299ALJABERNo ratings yet
- Complaint Form - 2016Document6 pagesComplaint Form - 2016muhammed kurtNo ratings yet
- Will Planning GuideDocument30 pagesWill Planning GuiderajivermaNo ratings yet
- When A Loved One DiesDocument20 pagesWhen A Loved One Diesrates4termNo ratings yet
- Part A - To Be Completed by Applicant (Or Authorized Third Party Representative)Document2 pagesPart A - To Be Completed by Applicant (Or Authorized Third Party Representative)malcolm grantNo ratings yet
- Form - Bupa Claim FormDocument2 pagesForm - Bupa Claim FormJoe Sayavongsa100% (3)
- Application To File For A Islamic Divorce (Talaq) : Possible - "Save" and Email Back To UsDocument4 pagesApplication To File For A Islamic Divorce (Talaq) : Possible - "Save" and Email Back To UsMuhammad IrfanNo ratings yet
- Request For Marriage Certifi Cate: (For Marriages Which Took Place in Ontario Only)Document4 pagesRequest For Marriage Certifi Cate: (For Marriages Which Took Place in Ontario Only)alexandraNo ratings yet
- Hgc Leased Ktt Mt103 Oneway (1)Document25 pagesHgc Leased Ktt Mt103 Oneway (1)xps.fpsNo ratings yet
- Comptroller of The Currency - ComplaintDocument5 pagesComptroller of The Currency - ComplaintMaster ChiefNo ratings yet
- Singapore Dental Claim Form Interactive M003 60E 010115Document5 pagesSingapore Dental Claim Form Interactive M003 60E 010115Nazim SalehNo ratings yet
- Form BUPADocument4 pagesForm BUPAterusunduhNo ratings yet
- 11076EDocument0 pages11076EDilpreet SinghNo ratings yet
- THAS - Referral Form 2022Document2 pagesTHAS - Referral Form 2022NemesisNo ratings yet
- SGP Generic Claim FormDocument5 pagesSGP Generic Claim FormSanny HamdaniNo ratings yet
- Basic no-frills banking Visa debit accountDocument9 pagesBasic no-frills banking Visa debit accountJason ReadNo ratings yet
- DS2444 A PrintDocument10 pagesDS2444 A PrintstatchuroseNo ratings yet
- D StatmentDocument8 pagesD StatmentHihiNo ratings yet
- Khula Application FormDocument8 pagesKhula Application FormSubhan AzadNo ratings yet
- Application For Payment of Housing Benefit Direct To Landlord Safeguard Referral FormDocument2 pagesApplication For Payment of Housing Benefit Direct To Landlord Safeguard Referral FormAlpamisNo ratings yet
- Disability Claim Form 7days Waiting EngDocument3 pagesDisability Claim Form 7days Waiting EngJonathan BorleyNo ratings yet
- ApointeeDocument8 pagesApointeeaymanNo ratings yet
- Probate Made Simple: The essential guide to saving money and getting the most out of your solicitorFrom EverandProbate Made Simple: The essential guide to saving money and getting the most out of your solicitorNo ratings yet
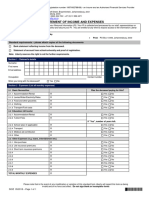
- Statement of Income and ExpensesDocument2 pagesStatement of Income and ExpensestcdieselsolutionsrsaNo ratings yet
- Reg_28_Asset_Allocation_CalculatorDocument5 pagesReg_28_Asset_Allocation_CalculatortcdieselsolutionsrsaNo ratings yet
- Affidavit - Confirmation as to whom deceased was living with at time of death in a sworn affidavitDocument1 pageAffidavit - Confirmation as to whom deceased was living with at time of death in a sworn affidavittcdieselsolutionsrsaNo ratings yet
- Affidavit - Confirmation as to whom deceased was living with at time of death in a sworn affidavitDocument1 pageAffidavit - Confirmation as to whom deceased was living with at time of death in a sworn affidavittcdieselsolutionsrsaNo ratings yet
- German Truck CheatDocument3 pagesGerman Truck Cheatdukagold11No ratings yet
- 5 Schedule Timetable FLIFODocument8 pages5 Schedule Timetable FLIFOAlba FernándezNo ratings yet
- Week 7Document68 pagesWeek 7Swapnil Sen100% (1)
- R.J. Reynolds Internation FinancingDocument2 pagesR.J. Reynolds Internation FinancingUmair ShaikhNo ratings yet
- ENGINE OVERHAUL 2.6 4cylDocument24 pagesENGINE OVERHAUL 2.6 4cylalbertoNo ratings yet
- Assign Controlling Areas and Company Codes for Optimal Cost AccountingDocument4 pagesAssign Controlling Areas and Company Codes for Optimal Cost Accountingatsc68No ratings yet
- Tor Analysis Hidden ServicesDocument4 pagesTor Analysis Hidden ServicesResearch GuyNo ratings yet
- Swat Modflow TutorialDocument56 pagesSwat Modflow TutorialfrenkiNo ratings yet
- Circuit Breaker GalilioDocument34 pagesCircuit Breaker GalilioMoaz KhursheedNo ratings yet
- 1920s Irish Crochet Lace Edging OriginalDocument8 pages1920s Irish Crochet Lace Edging OriginalLaura HortopanuNo ratings yet
- The Effective Length of Columns in MultiDocument12 pagesThe Effective Length of Columns in MulticoolkaisyNo ratings yet
- Free Fall LabDocument1 pageFree Fall Labapi-276596299No ratings yet
- Schoonebeek Kivi 09 AprilDocument25 pagesSchoonebeek Kivi 09 AprilmeloszNo ratings yet
- New Position Performance Evaluation FormDocument4 pagesNew Position Performance Evaluation FormRomero SanvisionairNo ratings yet
- Chapter.4 Creativity - And.business - IdeaDocument22 pagesChapter.4 Creativity - And.business - IdeaAjsa MulicNo ratings yet
- United International University: Post Graduate Diploma in Human Resource Management Course TitleDocument20 pagesUnited International University: Post Graduate Diploma in Human Resource Management Course TitleArpon Kumer DasNo ratings yet
- Courts CP, XO CP, Circumvention - DDI 2015 SWSDocument311 pagesCourts CP, XO CP, Circumvention - DDI 2015 SWSdavidsi325No ratings yet
- Boston Scientific Corporation v. Mabey, 10th Cir. (2011)Document8 pagesBoston Scientific Corporation v. Mabey, 10th Cir. (2011)Scribd Government DocsNo ratings yet
- Bibicoff Ic Resume 2022 09 For WebsiteDocument3 pagesBibicoff Ic Resume 2022 09 For Websiteapi-633250343No ratings yet
- 8200.47 Transponder Landing SystemDocument28 pages8200.47 Transponder Landing SystemLê Khánh DuyNo ratings yet
- Business Finance Week 2 2Document14 pagesBusiness Finance Week 2 2Phoebe Rafunsel Sumbongan Juyad100% (1)
- Sample Whistle Blower PolicyDocument2 pagesSample Whistle Blower Policy4geniecivilNo ratings yet
- Section 18 AASHTODocument5 pagesSection 18 AASHTOoscarpetroflexNo ratings yet
- CV Raho 2020 PDFDocument5 pagesCV Raho 2020 PDFraholiveiraNo ratings yet
- KemmyDocument22 pagesKemmyKemi HamzatNo ratings yet
- RollingDocument54 pagesRollingavutu_kunduru100% (1)
- Roadmap, Iquame, Ched Rquat and Others: Corazon M. NeraDocument27 pagesRoadmap, Iquame, Ched Rquat and Others: Corazon M. NeraJhun LeabresNo ratings yet
- GEC 6 Lesson 12Document19 pagesGEC 6 Lesson 12Annie CabugNo ratings yet
- Final Project Capital BudgetingDocument52 pagesFinal Project Capital BudgetingYugendra Babu K100% (2)
- Nokia Help PDFDocument101 pagesNokia Help PDFTim GargNo ratings yet