You might also like
- 2021 - 1st Sem - INTRODUCTION TO ANATOMY AND PHYSIOLOGY TRANSDocument7 pages2021 - 1st Sem - INTRODUCTION TO ANATOMY AND PHYSIOLOGY TRANSMaria Emmaculada ConcepcionNo ratings yet
- Mechanisms That Produce Change in PopulationsDocument44 pagesMechanisms That Produce Change in PopulationsEvangelene Esquillo SanaNo ratings yet
- 2019-Circulating Tumor DNA For Early Cancer DetectionDocument14 pages2019-Circulating Tumor DNA For Early Cancer Detectionvivitri.dewiNo ratings yet
- Physical SelfDocument15 pagesPhysical SelfJay FortunadoNo ratings yet
- ELS Q2 M4 How-Representative... 15pDocument15 pagesELS Q2 M4 How-Representative... 15pRachel Ann Canlas100% (1)
- Test Bank For Microbiology A Systems Approach 3rd Edition by CowanDocument25 pagesTest Bank For Microbiology A Systems Approach 3rd Edition by CowanJoseph Williams100% (1)
- SCIENCE MELCs Grade 7Document4 pagesSCIENCE MELCs Grade 7Gisela CapiliNo ratings yet
- S6 - Q2 - DLPS - Week 1 To 5Document302 pagesS6 - Q2 - DLPS - Week 1 To 5Yhanlouise Bermillo100% (2)
- Comparison of Cell Stabilizing Blood Collection Tubes For Circulating Plasma Tumor DNADocument15 pagesComparison of Cell Stabilizing Blood Collection Tubes For Circulating Plasma Tumor DNAxcvbnbNo ratings yet
- Performance of Streck cfDNA Blood Collection Tubes For Liquid Biopsy TestingDocument18 pagesPerformance of Streck cfDNA Blood Collection Tubes For Liquid Biopsy TestingxcvbnbNo ratings yet
- Diurnal Stability of Cell Free Dna and Cell Free Rna in Human Plasma SamplesDocument8 pagesDiurnal Stability of Cell Free Dna and Cell Free Rna in Human Plasma SamplesRaees EbrahimNo ratings yet
- Polymerase Chain ReactionDocument9 pagesPolymerase Chain ReactionHadiyan PutraNo ratings yet
- Liquid Biopsy: Is There An Advantage To Analyzing Circulating Exosomal Dna Compared To Cfdna or Are They The Same?Document4 pagesLiquid Biopsy: Is There An Advantage To Analyzing Circulating Exosomal Dna Compared To Cfdna or Are They The Same?Muhammad Javed GabaNo ratings yet
- KrasDocument14 pagesKrasHà QuảnNo ratings yet
- Diagnostic Accuracy of Cerebrospinal Fluid ProteinDocument14 pagesDiagnostic Accuracy of Cerebrospinal Fluid ProteinTarigNo ratings yet
- Jiang 2016Document12 pagesJiang 2016Madalina FoteaNo ratings yet
- PCR 短序列插入 PDFDocument7 pagesPCR 短序列插入 PDFTianliang GuoNo ratings yet
- Research Paper On Real Time PCRDocument4 pagesResearch Paper On Real Time PCRuzmlivznd100% (1)
- 1 s2.0 S0021967320311225 MainDocument8 pages1 s2.0 S0021967320311225 MainMida H. MayelNo ratings yet
- A Bumpy Ride On The Diagnostic Bench of Massive Parallel Sequencing, The Case of The Mitochondrial GenomeDocument9 pagesA Bumpy Ride On The Diagnostic Bench of Massive Parallel Sequencing, The Case of The Mitochondrial GenomeMayra EduardoffNo ratings yet
- Comparison of Customized Spin-Column and Salt-Precipitation Finger-Prick Blood DNA ExtractionDocument6 pagesComparison of Customized Spin-Column and Salt-Precipitation Finger-Prick Blood DNA ExtractionIndah Maulidya IriantiNo ratings yet
- Bio Paper TestingDocument3 pagesBio Paper Testingapi-284761165No ratings yet
- Research Paper On PCRDocument6 pagesResearch Paper On PCRcajzsqp2100% (1)
- JurnalDocument6 pagesJurnalAnonymous bYYJdvXhlNNo ratings yet
- PHD Thesis On Dna BarcodingDocument5 pagesPHD Thesis On Dna BarcodingStephen Faucher100% (2)
- Editorial: Quality and Safety of Blood ProductsDocument3 pagesEditorial: Quality and Safety of Blood ProductsBhumiNo ratings yet
- Clement I 2015Document7 pagesClement I 2015Felipe MNo ratings yet
- The Research of The Application of A New Urinary BDocument7 pagesThe Research of The Application of A New Urinary BNealNo ratings yet
- Biochemistry, Polymerase Chain Reaction (PCR) - StatPearls - NCBI BookshelfDocument4 pagesBiochemistry, Polymerase Chain Reaction (PCR) - StatPearls - NCBI BookshelfsasaNo ratings yet
- MethodMolebiol V1039published PDFDocument313 pagesMethodMolebiol V1039published PDFМ.К. МариNo ratings yet
- 1 s2.0 S1556086422019086 MainDocument15 pages1 s2.0 S1556086422019086 MainJesus Miguel Lazaro LeonNo ratings yet
- 10 1016@j Urolonc 2019 03 007Document10 pages10 1016@j Urolonc 2019 03 007Marijana KnezovicNo ratings yet
- Isolation of Cell-Free DNA From Seminal FluidDocument7 pagesIsolation of Cell-Free DNA From Seminal FluidSabrina JonesNo ratings yet
- Identification of A 14-Lncrna Signature and Construction of A Prognostic Nomogram Predicting Overall Survival of Gastric CancerDocument14 pagesIdentification of A 14-Lncrna Signature and Construction of A Prognostic Nomogram Predicting Overall Survival of Gastric CancerAriani ArinNo ratings yet
- PIIS1525157816302215Document7 pagesPIIS1525157816302215Madalina FoteaNo ratings yet
- MinIon 2022Document6 pagesMinIon 2022wajnat tounsiNo ratings yet
- Van Schie RC Wilson ME: J Immunol MethodsDocument9 pagesVan Schie RC Wilson ME: J Immunol MethodsGAURAVNo ratings yet
- A Diagnostic Study Comparing Conventional and Real-Time PCR For Strongyloides Stercoralis On Urine and On Faecal SamplesDocument4 pagesA Diagnostic Study Comparing Conventional and Real-Time PCR For Strongyloides Stercoralis On Urine and On Faecal SamplesSamuel VergaraNo ratings yet
- Pum1 and Rnase P Genes As Potential Cell-Free Dna Markers inDocument10 pagesPum1 and Rnase P Genes As Potential Cell-Free Dna Markers inArissa KohataNo ratings yet
- Cell Free DNA Plasma Lung Cancer Application NoteDocument4 pagesCell Free DNA Plasma Lung Cancer Application NoteLucas MarianoNo ratings yet
- Surface Plasmon Resonance Application in Prostate Cancer Biomarker ResearchDocument8 pagesSurface Plasmon Resonance Application in Prostate Cancer Biomarker ResearchZarrin TasnimNo ratings yet
- Brca 2011 HelicosDocument7 pagesBrca 2011 Helicosthumita kumiNo ratings yet
- W Biod05Document13 pagesW Biod05Эма СэмNo ratings yet
- Review PCRDocument3 pagesReview PCRwilma_angelaNo ratings yet
- Stojkovic 2012Document5 pagesStojkovic 2012Marko StojkovicNo ratings yet
- Journal Pone 0270710Document34 pagesJournal Pone 0270710ThanasisNo ratings yet
- Group2 - Gabriel - Journal Written Report 1Document19 pagesGroup2 - Gabriel - Journal Written Report 1andengphotoshere4No ratings yet
- Brief Communication: Saudi Journal of Kidney Diseases and TransplantationDocument5 pagesBrief Communication: Saudi Journal of Kidney Diseases and TransplantationAbigail Cueva PuellesNo ratings yet
- J Fsigen 2016 07 019Document32 pagesJ Fsigen 2016 07 019juliamorhunNo ratings yet
- Rna Extraction ThesisDocument5 pagesRna Extraction Thesisangelawilliamssavannah100% (2)
- Dna Biosensor ThesisDocument7 pagesDna Biosensor ThesisBuyEssaysTulsa100% (2)
- FP HeptitisDocument6 pagesFP HeptitisRiskaAnisaNo ratings yet
- Large Scale Real-Time PCR ValidationDocument17 pagesLarge Scale Real-Time PCR ValidationTarigNo ratings yet
- Kanker HatiDocument13 pagesKanker HatiAyhu Meelhy SusanthyNo ratings yet
- Clinical Laboratory Analysis - 2012 - Hashad - Free Circulating Tumor DNA As A Diagnostic Marker For Breast CancerDocument6 pagesClinical Laboratory Analysis - 2012 - Hashad - Free Circulating Tumor DNA As A Diagnostic Marker For Breast Cancerfaraz.mirza1No ratings yet
- J JFLM 2017 01 003Document26 pagesJ JFLM 2017 01 003MylenaNo ratings yet
- AP1 AP2 PCR Method For AHPND Detection - Flegel 2013Document6 pagesAP1 AP2 PCR Method For AHPND Detection - Flegel 2013Alden ReynaNo ratings yet
- Polymerase Chain Reaction-Based Detection of Lymphatic FilariasisDocument6 pagesPolymerase Chain Reaction-Based Detection of Lymphatic FilariasisDewi WulansariNo ratings yet
- Flowcytometry Dna Analysis in CancerDocument36 pagesFlowcytometry Dna Analysis in CancerAstri Arri FebriantiNo ratings yet
- Biomolecular Detection and Quantification: SciencedirectDocument23 pagesBiomolecular Detection and Quantification: SciencedirectSYED MAAZ TARIQNo ratings yet
- Real-Time PCR Detection of Plasmodium Directly From Whole Blood and Filter Paper SamplesDocument8 pagesReal-Time PCR Detection of Plasmodium Directly From Whole Blood and Filter Paper SamplesIca LatifahNo ratings yet
- Jiang 2019Document5 pagesJiang 2019Ali Halim YILMAZNo ratings yet
- Litrature and DesignDocument17 pagesLitrature and Designshruthi gNo ratings yet
- Performance of CellaVision DM96 in Leukocyte ClassificationDocument5 pagesPerformance of CellaVision DM96 in Leukocyte ClassificationarielNo ratings yet
- Recent Research Paper On PCRDocument4 pagesRecent Research Paper On PCRgz8zw71w100% (1)
- in House Production Method For Dna Ladde 036095bbDocument5 pagesin House Production Method For Dna Ladde 036095bbAlessandroNo ratings yet
- 6 CCF 1 DDocument1 page6 CCF 1 DEdsel SiababaNo ratings yet
- MCGILL Updated PL Jan. 032023Document31 pagesMCGILL Updated PL Jan. 032023Edsel SiababaNo ratings yet
- Test Task - TemplateDocument3 pagesTest Task - TemplateEdsel SiababaNo ratings yet
- LANDLITE Brochure 2023 SEPTDocument32 pagesLANDLITE Brochure 2023 SEPTEdsel SiababaNo ratings yet
- fG10 Evidence of Evolution, Evolutionary Pattern, Population DynamicsDocument6 pagesfG10 Evidence of Evolution, Evolutionary Pattern, Population DynamicsSecond BooksNo ratings yet
- Edible Portion Dan Kandungan Kimia Ikan Gabus (Channa Striata)Document6 pagesEdible Portion Dan Kandungan Kimia Ikan Gabus (Channa Striata)Nur Azzatul AmaliyahNo ratings yet
- (BMED66) HUMAN ANATOMY & PHYSIOLOGY WITH PATHOPHYSIOLOGY Laboratory - Lecture - The Language of Anatomy Lesson 1Document4 pages(BMED66) HUMAN ANATOMY & PHYSIOLOGY WITH PATHOPHYSIOLOGY Laboratory - Lecture - The Language of Anatomy Lesson 1Abcd ReyesNo ratings yet
- Cell OrgenellesDocument10 pagesCell OrgenellesShruti TiwariNo ratings yet
- #1 Intro Animal BehaviourDocument24 pages#1 Intro Animal BehaviourTroy WilliamsNo ratings yet
- Studies On Fruit-Bud Differentiation in MangoDocument3 pagesStudies On Fruit-Bud Differentiation in MangoShailendra RajanNo ratings yet
- 18 Importance of Y ChromosomeDocument3 pages18 Importance of Y Chromosomeahsen fazaldadNo ratings yet
- 4 International A LevelDocument14 pages4 International A LevelJavaria MajidNo ratings yet
- Sexing in Guinea Fowls (Numida Meleagris)Document2 pagesSexing in Guinea Fowls (Numida Meleagris)Nisrina ZhafirahNo ratings yet
- Kami Export - Worksheet 14 Central DogmaDocument2 pagesKami Export - Worksheet 14 Central DogmaLindsey TamlinNo ratings yet
- Allometric Equations For Estimating Biomass of Bamboo - BaharuddinDocument9 pagesAllometric Equations For Estimating Biomass of Bamboo - Baharuddinaifie.ainiNo ratings yet
- Flashcards Bio PDFDocument59 pagesFlashcards Bio PDFmakanaka mukwairaNo ratings yet
- Yes No Not Given Practice 2Document2 pagesYes No Not Given Practice 2Gaming is not a crimeNo ratings yet
- Els Q2 W1Document2 pagesEls Q2 W1Lani GomezNo ratings yet
- Heinz 1977Document247 pagesHeinz 1977Ionut Costache100% (1)
- Muscle System kd13Document46 pagesMuscle System kd13Side PoorNo ratings yet
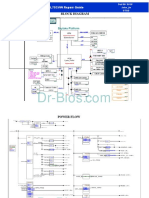
- Block Diagram: GL752VW Repair GuideDocument7 pagesBlock Diagram: GL752VW Repair GuideAidilNo ratings yet
- Issue7 MobileDocument44 pagesIssue7 MobileBhakti rautNo ratings yet
- Nervous System - Life Sciences Questions and Answers - SanfoundryDocument6 pagesNervous System - Life Sciences Questions and Answers - SanfoundryHUAWEI HUAWEINo ratings yet
- Drives and The CNSDocument12 pagesDrives and The CNSAndrewsNo ratings yet
- Scientific Report of The Stages of Prophase of A GrasshopperDocument4 pagesScientific Report of The Stages of Prophase of A GrasshopperVimson AlastraNo ratings yet
- Yds 5 Deneme Sinavi Ve Detayli Cevaplar Ve Aciklamalar 92928Document262 pagesYds 5 Deneme Sinavi Ve Detayli Cevaplar Ve Aciklamalar 92928Giray AlpaydinNo ratings yet
- Twenty-Five Thousand-Year-Old Triple Burial From Dolni Vestonice: An Ice-Age Family?Document9 pagesTwenty-Five Thousand-Year-Old Triple Burial From Dolni Vestonice: An Ice-Age Family?Aloysius RipariusNo ratings yet