You might also like
- SOAP NoteDocument8 pagesSOAP NoteAnonymous p0y5mmLQNo ratings yet
- Obstetric Nursing Study GuideDocument69 pagesObstetric Nursing Study GuideValerie100% (3)
- Chest CaseDocument19 pagesChest CaseNesma AdelNo ratings yet
- CASE 3 MEDICINE JULY 10 2019 AcutePyeloDocument15 pagesCASE 3 MEDICINE JULY 10 2019 AcutePyeloTrisNo ratings yet
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- Final Assessment Soap NoteDocument13 pagesFinal Assessment Soap Noteapi-494643478100% (3)
- Case Report VI Internal MedicineDocument13 pagesCase Report VI Internal MedicineGidu SaidNo ratings yet
- 14th Century - Black DeathDocument16 pages14th Century - Black DeathJean-pierre NegreNo ratings yet
- Constitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofDocument10 pagesConstitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofRichard ObinwankwoNo ratings yet
- Breastfeeding and Down SyndromeDocument239 pagesBreastfeeding and Down SyndromeSim M ChangNo ratings yet
- Health Assessment Project: Name: Ena Lewis Tutor: Sis Francis Group: 15Document27 pagesHealth Assessment Project: Name: Ena Lewis Tutor: Sis Francis Group: 15Blake KamminNo ratings yet
- Case Write-Up 1 Obstructive Jaundice With Cholecystitis Secondary To Ampullary TumorDocument21 pagesCase Write-Up 1 Obstructive Jaundice With Cholecystitis Secondary To Ampullary TumorwhosenahNo ratings yet
- Low Back PainDocument9 pagesLow Back PainDoc AchondoNo ratings yet
- Mrs - Lakshmi Aged 54 Years Who Is A Flower Seller Residing atDocument5 pagesMrs - Lakshmi Aged 54 Years Who Is A Flower Seller Residing atHariNo ratings yet
- Cwu Surgery Y5 AsyikinDocument21 pagesCwu Surgery Y5 AsyikinNurulasyikin MAANo ratings yet
- Chief ComplaintDocument7 pagesChief ComplaintyohannesNo ratings yet
- Pmls Finals ReviewerDocument72 pagesPmls Finals ReviewerIsiwjsbnwhshz Hshshzhbshs100% (1)
- Soap Note 4Document8 pagesSoap Note 4api-282129457100% (8)
- List of Diseases and Ailments With UrduDocument7 pagesList of Diseases and Ailments With Urduaik hindustaniNo ratings yet
- Case Clerking ApendicDocument15 pagesCase Clerking ApendicChen Cheng0% (1)
- Vagus Nerve: The Step By Step Guide To Understand The Power Of The Vagus Nerve. Self-Help Exercises For Chronic Illness, PTSD, Inflammation, Anxiety, Depression and Lots MoreFrom EverandVagus Nerve: The Step By Step Guide To Understand The Power Of The Vagus Nerve. Self-Help Exercises For Chronic Illness, PTSD, Inflammation, Anxiety, Depression and Lots MoreRating: 1 out of 5 stars1/5 (2)
- Case Write Up (Peadiatrics) SangariDocument11 pagesCase Write Up (Peadiatrics) SangariAmbhi GanaNo ratings yet
- Cwu SurgeryDocument16 pagesCwu SurgeryAslah NabilahNo ratings yet
- Write Up Surgery 1 TambahDocument22 pagesWrite Up Surgery 1 Tambahazizi abd rahmanNo ratings yet
- AbortionDocument16 pagesAbortionKim Lompot100% (1)
- Breast CarcinomaDocument13 pagesBreast Carcinomamegat120288100% (1)
- WeBSurg Winners 42 1Document129 pagesWeBSurg Winners 42 1Ana Adam100% (1)
- Addis Ababa University School of Medicine Department of Gynecology & ObstetricsDocument13 pagesAddis Ababa University School of Medicine Department of Gynecology & Obstetricspilual tongyikNo ratings yet
- Template Gyn Lo Abd PainDocument18 pagesTemplate Gyn Lo Abd PainHassan HarirNo ratings yet
- Case Report 1Document12 pagesCase Report 1mike sharewNo ratings yet
- HIVCase Report II Internal MedicineDocument12 pagesHIVCase Report II Internal Medicineaxmedfare138No ratings yet
- Case ReportDocument9 pagesCase ReportBerhanu DigamoNo ratings yet
- Case Report II Internal MedicineDocument11 pagesCase Report II Internal MedicineGidu SaidNo ratings yet
- History 1Document11 pagesHistory 1KaleabNo ratings yet
- Case Report IV Internal MedicineDocument11 pagesCase Report IV Internal MedicineGidu Said100% (1)
- Case Report III Internal MedicineDocument12 pagesCase Report III Internal MedicineGidu Said0% (1)
- Type The Document Title: Department of Surgery Case Report-IiDocument10 pagesType The Document Title: Department of Surgery Case Report-IiEyosiyas AbiyNo ratings yet
- SOAP Note 1 - Breast CADocument4 pagesSOAP Note 1 - Breast CAacvalvarioNo ratings yet
- Addis Ababa University Faculty of MedicineDocument12 pagesAddis Ababa University Faculty of MedicinedenekeNo ratings yet
- Acute PancreatitisDocument7 pagesAcute PancreatitisPatrick DycocoNo ratings yet
- Cwu Breast AbscessDocument10 pagesCwu Breast AbscessfarahmazlanNo ratings yet
- CRVHD Percipitated by IEDocument14 pagesCRVHD Percipitated by IEKemotherapy LifesucksNo ratings yet
- Personal Details: Past Medical HistoryDocument8 pagesPersonal Details: Past Medical HistoryKemotherapy LifesucksNo ratings yet
- Gynecology and Obstetrics Ward Case Report - 1: Balesew Enawgaw (C-1) Id: Medr 24/05Document10 pagesGynecology and Obstetrics Ward Case Report - 1: Balesew Enawgaw (C-1) Id: Medr 24/05denekeNo ratings yet
- BPH Sample To Case ReportDocument12 pagesBPH Sample To Case ReportBirhanu ShiferawNo ratings yet
- Case Report: Tikur Anbesa Specialized HospitalDocument11 pagesCase Report: Tikur Anbesa Specialized HospitalTefera LeteboNo ratings yet
- Case ReportDocument17 pagesCase ReportdenekeNo ratings yet
- HSP Case Presentation PDFDocument71 pagesHSP Case Presentation PDFJoan Luis100% (1)
- Surgery Long Cases PrintDocument49 pagesSurgery Long Cases Printdrroshanshaji786No ratings yet
- Clinical Case: Section A - Group 8Document68 pagesClinical Case: Section A - Group 8madison Deli100% (1)
- PCD Case ReproductiveDocument8 pagesPCD Case ReproductivedenekeNo ratings yet
- Jiefang Rvenue, Hankou, Hubei. Tel: 857307523 and WifeDocument4 pagesJiefang Rvenue, Hankou, Hubei. Tel: 857307523 and WifeAmit GoswamiNo ratings yet
- Ent Case Report Acute Otitis Media Stage IIIDocument12 pagesEnt Case Report Acute Otitis Media Stage IIIRem Alfelor100% (1)
- Week 3 Case - DOBDocument3 pagesWeek 3 Case - DOBKirk Matthew ZhuNo ratings yet
- Gynecology and Obstetrics Ward Case: SUBMITTED TO: - Dr. Samuel (Gynecologist & Obstetrician)Document8 pagesGynecology and Obstetrics Ward Case: SUBMITTED TO: - Dr. Samuel (Gynecologist & Obstetrician)denekeNo ratings yet
- Pedia - History Taking and Physical Exam - PGI Leira BarbosaDocument6 pagesPedia - History Taking and Physical Exam - PGI Leira BarbosaLeira BarbosaNo ratings yet
- Form Health History Documentation: Biographical DataDocument7 pagesForm Health History Documentation: Biographical DataSandra SanonNo ratings yet
- Final HX and Physical Dec 2022Document5 pagesFinal HX and Physical Dec 2022Mallory ZaborNo ratings yet
- ObGyn CWU 3Document16 pagesObGyn CWU 3ppmmttkkccNo ratings yet
- Name: Wong Wai Kheong Matrix No: BMS12081154Document13 pagesName: Wong Wai Kheong Matrix No: BMS12081154myolie wuNo ratings yet
- Duran, Kayllien - Group 7 Sec ADocument5 pagesDuran, Kayllien - Group 7 Sec AKAYLLIEN DURANNo ratings yet
- CASE STUDY Lung Ca With Pleural EffDocument8 pagesCASE STUDY Lung Ca With Pleural EffL4 CLERK - UY, Rhea Andrea F.No ratings yet
- Vita Listia Setya Dewi (P1337424117010) 2. Erni Fadhlina (P1337424117027)Document5 pagesVita Listia Setya Dewi (P1337424117010) 2. Erni Fadhlina (P1337424117027)LabibaNo ratings yet
- IM Gastro FinalDocument10 pagesIM Gastro FinalIzzyMaxinoNo ratings yet
- History: O Identifying DataDocument10 pagesHistory: O Identifying DataJofen Ann Hisoler TangpuzNo ratings yet
- Intestinal and Colonic Physiology and Biochemistry (Part 2 - Secretion, Digestion, Absorption) (Slides With Notes)Document69 pagesIntestinal and Colonic Physiology and Biochemistry (Part 2 - Secretion, Digestion, Absorption) (Slides With Notes)kuchipuchi12No ratings yet
- Asepsis and Infection ControlDocument24 pagesAsepsis and Infection Controlabdisalaan hassanNo ratings yet
- EBMDocument6 pagesEBMjoyce_garcia_10No ratings yet
- Somatic RecombinationDocument5 pagesSomatic RecombinationNoor Ul NaeemNo ratings yet
- Interstitial Lung Diseases Radiology 22222Document26 pagesInterstitial Lung Diseases Radiology 22222Daniel AshooriNo ratings yet
- EMS Airflow BrochureDocument2 pagesEMS Airflow BrochureMELHEM_J8008No ratings yet
- Drug Name Mechanism of Action Indication Contraindication Side Effects/Adverse Reaction Nursing Responsibility CNS-malaiseDocument3 pagesDrug Name Mechanism of Action Indication Contraindication Side Effects/Adverse Reaction Nursing Responsibility CNS-malaisekristel_nicole18yahoNo ratings yet
- Nama: Khoirus Viestaria NIM: 135130101111035 Kelas: 2013/CDocument2 pagesNama: Khoirus Viestaria NIM: 135130101111035 Kelas: 2013/CDina SahmirandaNo ratings yet
- ANC ModuleDocument103 pagesANC ModulePreeti ChouhanNo ratings yet
- All Your Advanced Analysis Needs One Comprehensive Solution: StartDocument185 pagesAll Your Advanced Analysis Needs One Comprehensive Solution: StartMitra MedistraNo ratings yet
- Strickland PresentationDocument1 pageStrickland Presentationmariopi2495No ratings yet
- Resistance Is Futile ... or Is It?: The Immune System and HIV InfectionDocument28 pagesResistance Is Futile ... or Is It?: The Immune System and HIV InfectionRachel Mwale MwazigheNo ratings yet
- Disentri AmubaDocument8 pagesDisentri AmubaVivi DeviyanaNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Nic - (Https://Covid19Cc - Nic.In) Page 1/18 27-04-2021 13:49:04Document18 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Nic - (Https://Covid19Cc - Nic.In) Page 1/18 27-04-2021 13:49:04Sumit PatelNo ratings yet
- Journal of Medicinal Plants Research VolDocument19 pagesJournal of Medicinal Plants Research VolAtheena Jin Anjelle SeveroNo ratings yet
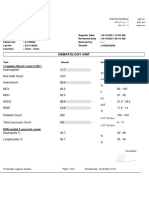
- Hematology Unit: Complete Blood Count (CBC)Document2 pagesHematology Unit: Complete Blood Count (CBC)Rasha ElbannaNo ratings yet
- Filosofi Kesehatan MasyarakatDocument4 pagesFilosofi Kesehatan MasyarakatJennilynn YusameNo ratings yet
- Appendix 1: Chemotherapy ProtocolsDocument3 pagesAppendix 1: Chemotherapy ProtocolsImam Hakim SuryonoNo ratings yet
- BIOLOGYDocument5 pagesBIOLOGYDiana NurulNo ratings yet
- Publication 2022Document21 pagesPublication 2022zuraNo ratings yet
- Congenital Anomalies and Variations of The Bile and Pancreatic Ducts - Magnetic Resonance Cholangiopancreatography Findings, Epidemiology and Clinical SignificanceDocument19 pagesCongenital Anomalies and Variations of The Bile and Pancreatic Ducts - Magnetic Resonance Cholangiopancreatography Findings, Epidemiology and Clinical SignificanceRoberto HernandezNo ratings yet
- Bone Tumors in Children and Adolescents-FDocument76 pagesBone Tumors in Children and Adolescents-Fkara_korumNo ratings yet
- Icd 10Document3 pagesIcd 10ghinaNo ratings yet
- Gastric GavageDocument3 pagesGastric GavageRico Delgado of WorldbexNo ratings yet