You might also like
- 3 Manacsa&Tan 2012 Strong Republic SidetrackedDocument41 pages3 Manacsa&Tan 2012 Strong Republic SidetrackedGil Osila JaradalNo ratings yet
- Finding The Answers To The Research Questions (Qualitative) : Quarter 4 - Module 5Document39 pagesFinding The Answers To The Research Questions (Qualitative) : Quarter 4 - Module 5Jernel Raymundo80% (5)
- Aka GMP Audit FormDocument8 pagesAka GMP Audit FormAlpian BosixNo ratings yet
- Construction Materials and Testing: "WOOD"Document31 pagesConstruction Materials and Testing: "WOOD"Aira Joy AnyayahanNo ratings yet
- BJR 20140542Document8 pagesBJR 20140542Sava Marius ConstantinNo ratings yet
- Evaluating Intervertebral Foramen MeasurDocument7 pagesEvaluating Intervertebral Foramen MeasurrecepNo ratings yet
- Quantification of Fracture Healing From Radiographs Using The Maximum Callus IndexDocument6 pagesQuantification of Fracture Healing From Radiographs Using The Maximum Callus IndexFaheem AhmedNo ratings yet
- Comparison of Iliac Crest Versus Supraacetabular External FixatorDocument7 pagesComparison of Iliac Crest Versus Supraacetabular External FixatortripodegrandeNo ratings yet
- Assessment of central cartilaginous tumor of the appendicular bone: inter-observer and intermodality agreement and comparison of diagnostic performance of CT and MRIDocument11 pagesAssessment of central cartilaginous tumor of the appendicular bone: inter-observer and intermodality agreement and comparison of diagnostic performance of CT and MRIsilvana mendoncaNo ratings yet
- 1 s2.0 S2212440312000442 MainDocument6 pages1 s2.0 S2212440312000442 MainMarinaNo ratings yet
- improved maskrcnnDocument13 pagesimproved maskrcnnVainavi SamantNo ratings yet
- Ghid Plex Brahial Conturaj PDFDocument7 pagesGhid Plex Brahial Conturaj PDFMiruna MafteiNo ratings yet
- Jurnal ReadingDocument7 pagesJurnal ReadingHanif UlinNo ratings yet
- Aging and Cortical Bone Density of Mandible WithDocument5 pagesAging and Cortical Bone Density of Mandible WithAsdal AttoNo ratings yet
- 11 NMDocument7 pages11 NMAbhilash VemulaNo ratings yet
- Osteology 01 00009Document6 pagesOsteology 01 00009Dewi HanaNo ratings yet
- Ojsadmin, 302Document7 pagesOjsadmin, 302Abhilash VemulaNo ratings yet
- Vibe Mri: An Alternative To CT in The Imaging of Sports-Related Osseous Pathology?Document5 pagesVibe Mri: An Alternative To CT in The Imaging of Sports-Related Osseous Pathology?Ade Febrian RamadhanNo ratings yet
- Morphological Determination of Glenohumeral Joint and Acromioclavicular Joint With Computed TomographyDocument7 pagesMorphological Determination of Glenohumeral Joint and Acromioclavicular Joint With Computed TomographyRodrigoNo ratings yet
- Risk Prediction For Development of Traumatic Cervical Spinal Cord Injury Without Spinal InstabilityDocument7 pagesRisk Prediction For Development of Traumatic Cervical Spinal Cord Injury Without Spinal InstabilityTantriSaptennoPattiradjawaneNo ratings yet
- Analysis of Sacrococcygeal Morphology in Koreans Using Computed TomographyDocument9 pagesAnalysis of Sacrococcygeal Morphology in Koreans Using Computed TomographyUkik SaliroNo ratings yet
- Sicotj 8 34Document5 pagesSicotj 8 34robertoNo ratings yet
- MRI Craniocervical LigamentsDocument9 pagesMRI Craniocervical Ligamentsintan aryantiNo ratings yet
- Chemicalshift MRIDocument4 pagesChemicalshift MRIshreyahospital.motinagarNo ratings yet
- The Use of Whole Body Diffusion-Weighted PMMRI in Timing of Perinatal DeathsDocument7 pagesThe Use of Whole Body Diffusion-Weighted PMMRI in Timing of Perinatal DeathsDenys PutraNo ratings yet
- Weiner 2008Document6 pagesWeiner 2008Indira Ulfa DunandNo ratings yet
- Low Reliability of CBCT for Diagnosing TMJ Soft Tissue CalcificationDocument5 pagesLow Reliability of CBCT for Diagnosing TMJ Soft Tissue CalcificationMarinaNo ratings yet
- Imaging Techniques for Sacroiliac Joint PainDocument11 pagesImaging Techniques for Sacroiliac Joint PainIsmail Tidak Ada KepanjanganNo ratings yet
- okuyama1994Document3 pagesokuyama1994lauraserranogonzalez517No ratings yet
- Anatomical Variationsofthe Foramen MagnumDocument11 pagesAnatomical Variationsofthe Foramen MagnumChavdarNo ratings yet
- Leakage of Cement in Percutaneous Transpedicular Vertebroplasty For Painful Osteoporotic Compression FracturesDocument7 pagesLeakage of Cement in Percutaneous Transpedicular Vertebroplasty For Painful Osteoporotic Compression FracturesRamy ElmasryNo ratings yet
- 1 s2.0 S1878875023005466 MainDocument6 pages1 s2.0 S1878875023005466 MainJay ParkNo ratings yet
- 3D CT Evaluation of Craniofacial Deformity in Patients with Untreated TorticollisDocument10 pages3D CT Evaluation of Craniofacial Deformity in Patients with Untreated TorticollisLaidetNo ratings yet
- Automated Accurate and Three Dimensional Method For Calc - 2018 - Journal of BDocument6 pagesAutomated Accurate and Three Dimensional Method For Calc - 2018 - Journal of BRyuNo ratings yet
- Tian 2012Document6 pagesTian 2012Orto MespNo ratings yet
- Comparison of Two - and Three-Dimensional Measurement of The Cobb Angle in Scoliosis - Lechner Et Al. 2017Document6 pagesComparison of Two - and Three-Dimensional Measurement of The Cobb Angle in Scoliosis - Lechner Et Al. 2017Mohammad KaramNo ratings yet
- Chahla 2018Document9 pagesChahla 2018Miguel Angel Lamas RamirezNo ratings yet
- Evaluation of The Severity of Temporomandibular Joint Osteoarthritic Changes Related To Age Using Cone Beam Computed TomographyDocument8 pagesEvaluation of The Severity of Temporomandibular Joint Osteoarthritic Changes Related To Age Using Cone Beam Computed TomographyCharly Patricio Trincado FuenzalidaNo ratings yet
- Accuracy of Xray and Mri in Defining Tumor MarginDocument7 pagesAccuracy of Xray and Mri in Defining Tumor MarginDinda SaviraNo ratings yet
- BMC Musculoskeletal DisordersDocument7 pagesBMC Musculoskeletal DisordersTinkovan IonNo ratings yet
- MSCT Cervical Trauma Diagnosis TechniquesDocument4 pagesMSCT Cervical Trauma Diagnosis TechniquesRegina Rara AuliaNo ratings yet
- Radiographic Measurements of Normal Elbows: Clinical Relevance To Olecranon FracturesDocument4 pagesRadiographic Measurements of Normal Elbows: Clinical Relevance To Olecranon Fracturesjmhinos4833No ratings yet
- Reliability and Validity of Ultrasound Imaging of Features of Knee Osteoarthritis in The CommunityDocument8 pagesReliability and Validity of Ultrasound Imaging of Features of Knee Osteoarthritis in The CommunityCaitlynNo ratings yet
- Magnetic Resonance Imaging of The HipDocument11 pagesMagnetic Resonance Imaging of The HipsaadNo ratings yet
- Denny - 2021 - Coronal Pulp Cavity Index An Aid in Age Determination-Cone Beam CT StudyDocument6 pagesDenny - 2021 - Coronal Pulp Cavity Index An Aid in Age Determination-Cone Beam CT StudyGgNo ratings yet
- JCM 12 06172Document12 pagesJCM 12 06172Taulant MukaNo ratings yet
- Research ArticleDocument6 pagesResearch ArticleAnonymous I4Z6cPGSBnNo ratings yet
- 3D in Vivo Cervical Spine Kinematis: Preliminary Comparison of Fusion Patients and Control SubjectsDocument2 pages3D in Vivo Cervical Spine Kinematis: Preliminary Comparison of Fusion Patients and Control SubjectsAnthony OrtegaNo ratings yet
- YALE ET ALStudyofThreeDimensionalMorphologyDocument7 pagesYALE ET ALStudyofThreeDimensionalMorphology19-2 W. RIFQA NURFAIDAHNo ratings yet
- Upright, Prone, and Supine Spinal Morphology and Alignment in Adolescent Idiopathic ScoliosisDocument8 pagesUpright, Prone, and Supine Spinal Morphology and Alignment in Adolescent Idiopathic ScoliosisMr. wNo ratings yet
- 3 - Ultrasonido y Masa MuscularDocument7 pages3 - Ultrasonido y Masa MuscularFlor De LotoNo ratings yet
- Quantitative and Qualitative AssessmentDocument7 pagesQuantitative and Qualitative AssessmentErnestoNo ratings yet
- Oarsi 2Document3 pagesOarsi 2Mohd Yusof BaharuddinNo ratings yet
- Detecting Statistically Significant Changes in Cartilage Thickness With Sub-Voxel PrecisionDocument1 pageDetecting Statistically Significant Changes in Cartilage Thickness With Sub-Voxel PrecisionadmonsalvoNo ratings yet
- 1 s2.0 S0749806314004009 MainDocument10 pages1 s2.0 S0749806314004009 MainbilourNo ratings yet
- Acta Orthopaedica Et Traumatologica TurcicaDocument6 pagesActa Orthopaedica Et Traumatologica TurcicaAnonymous TvPFA4No ratings yet
- Assessment of Vertebral Wedge Strength Using Cancellous Textural - 2018 - JournaDocument7 pagesAssessment of Vertebral Wedge Strength Using Cancellous Textural - 2018 - JournaRyuNo ratings yet
- Is There Any Relation Between Distal Parameters of The Femur and Its Height and Width?Document9 pagesIs There Any Relation Between Distal Parameters of The Femur and Its Height and Width?juanibirisNo ratings yet
- Contents Lists Available At: SciencedirectDocument7 pagesContents Lists Available At: SciencedirectAmina GoharyNo ratings yet
- Cuñas MetalicasDocument8 pagesCuñas MetalicasOciel AcostaNo ratings yet
- Diagnostic Accuracy of Zero-Echo Time MRI For The Evaluation of Cervical Neural Foraminal StenosisDocument20 pagesDiagnostic Accuracy of Zero-Echo Time MRI For The Evaluation of Cervical Neural Foraminal StenosisThiago Astil RizzettoNo ratings yet
- 2004-Morphology of The Radial Head A Reverse Engineering Bases Evaluation Using Three-Dimensional Anatomical Data of Radial BoneDocument6 pages2004-Morphology of The Radial Head A Reverse Engineering Bases Evaluation Using Three-Dimensional Anatomical Data of Radial BonePongnarin JiamwatthanachaiNo ratings yet
- Research Article: Detailed Shoulder MRI Findings in Manual Wheelchair Users With Shoulder PainDocument8 pagesResearch Article: Detailed Shoulder MRI Findings in Manual Wheelchair Users With Shoulder PainairusmayantiNo ratings yet
- Quantitative MRI of the Spinal CordFrom EverandQuantitative MRI of the Spinal CordJulien Cohen-AdadNo ratings yet
- MNCs-consider-career-development-policyDocument2 pagesMNCs-consider-career-development-policySubhro MukherjeeNo ratings yet
- AP Standard Data All PDFDocument963 pagesAP Standard Data All PDFSiva Kumar100% (1)
- ASIA IVALUE Business ProfileDocument9 pagesASIA IVALUE Business ProfileDidiek PriambudiNo ratings yet
- CD 1 - Screening & DiagnosisDocument27 pagesCD 1 - Screening & DiagnosiskhairulfatinNo ratings yet
- GSAA HET 2005-15, Tranche B2 / BSABS 2005-TC2, Tranche M6 Shown As An Asset of Maiden LaneDocument122 pagesGSAA HET 2005-15, Tranche B2 / BSABS 2005-TC2, Tranche M6 Shown As An Asset of Maiden LaneTim BryantNo ratings yet
- Hotel Engineering Facilities: A Case Study of Maintenance PerformanceDocument7 pagesHotel Engineering Facilities: A Case Study of Maintenance PerformanceHoh Pui KeiNo ratings yet
- Fisher - Techincal Monograph 42 - Understanding DecibelsDocument8 pagesFisher - Techincal Monograph 42 - Understanding Decibelsleslie.lp2003No ratings yet
- A Primer On Financial Time Series AnalysisDocument93 pagesA Primer On Financial Time Series AnalysisKM AgritechNo ratings yet
- Ap4955 PDFDocument4 pagesAp4955 PDFGilvan HenriqueNo ratings yet
- Idler Sprockets: Poly Chain GT and Powergrip GTDocument2 pagesIdler Sprockets: Poly Chain GT and Powergrip GTVolodymуr VorobetsNo ratings yet
- Gfk-1383a 05012Document108 pagesGfk-1383a 05012occhityaNo ratings yet
- Olt CliDocument2 pagesOlt CliMohammad SaeedNo ratings yet
- Rolls-Royce M250 FIRST Network: 2015 Customer Support DirectoryDocument76 pagesRolls-Royce M250 FIRST Network: 2015 Customer Support Directoryale11vigarNo ratings yet
- Bài tập tiếng Anh 12 (Reading)Document7 pagesBài tập tiếng Anh 12 (Reading)Minh AnhNo ratings yet
- Batt ChargerDocument2 pagesBatt Chargerdjoko witjaksonoNo ratings yet
- Year 12 Holiday Homework Term 3Document4 pagesYear 12 Holiday Homework Term 3Lucas GauciNo ratings yet
- DaburDocument3 pagesDaburchiru94No ratings yet
- Tle 10 4quarterDocument2 pagesTle 10 4quarterCaryll BaylonNo ratings yet
- Henoch Schönlein PurpuraDocument12 pagesHenoch Schönlein PurpuraRavania Rahadian Putri100% (1)
- Pharmacology Ain Shams 123 - Compress 1Document552 pagesPharmacology Ain Shams 123 - Compress 1ahmed hoty100% (1)
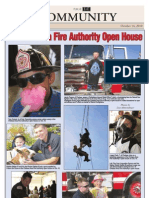
- CAFA Open House HighlightsDocument1 pageCAFA Open House HighlightsDaniel LaiNo ratings yet
- Engr2227 Apr03Document10 pagesEngr2227 Apr03Mohamed AlqaisiNo ratings yet
- READMEDocument3 pagesREADMERadu TimisNo ratings yet
- CB4 BBC Interviews EXTRA UnitDocument1 pageCB4 BBC Interviews EXTRA UnitCristianNo ratings yet
- Joe Ann MarcellanaDocument17 pagesJoe Ann MarcellanarudyNo ratings yet
- Download Zinc Surfaces A Guide To Alloys Finishes Fabrication And Maintenance In Architecture And Art 1St Edition L William Zahner all chapterDocument68 pagesDownload Zinc Surfaces A Guide To Alloys Finishes Fabrication And Maintenance In Architecture And Art 1St Edition L William Zahner all chapterdevin.brown498100% (7)