You might also like
- Carotid Endarterectomy: Experience in 8743 Cases.Document13 pagesCarotid Endarterectomy: Experience in 8743 Cases.Alexandre Campos Moraes AmatoNo ratings yet
- RIBA Outline Plan of Work ExplainedDocument20 pagesRIBA Outline Plan of Work ExplainedkenNo ratings yet
- Pola Cco 2013Document3 pagesPola Cco 2013akivaNo ratings yet
- Pnemothorax PDFDocument10 pagesPnemothorax PDFHelpful HandNo ratings yet
- An Evidence Based Blunt Trauma ProtocolDocument7 pagesAn Evidence Based Blunt Trauma ProtocolPepe pepe pepeNo ratings yet
- Miyazaki 2013Document6 pagesMiyazaki 2013Teja LaksanaNo ratings yet
- The Very Long-Term Outcome of Radiosurgery For Classical Trigeminal NeuralgiaDocument9 pagesThe Very Long-Term Outcome of Radiosurgery For Classical Trigeminal NeuralgiaJose Damian Lemus IbacacheNo ratings yet
- The Effectiveness and Safety of General and Spinal Anesthesia On Systemic Inflammatory Response in Patients With Tumor-Type Total Knee ArthroplastyDocument6 pagesThe Effectiveness and Safety of General and Spinal Anesthesia On Systemic Inflammatory Response in Patients With Tumor-Type Total Knee Arthroplastyjean carlo ulloa velaNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyAldo AtjehNo ratings yet
- 2 PDFDocument6 pages2 PDFOtto NaftariNo ratings yet
- USG Nervo Optico e TC CrânioDocument5 pagesUSG Nervo Optico e TC CrânioVictor CiriloNo ratings yet
- NERVIO OPTICO HIPERTENSIOM CRANEAL 2021Document5 pagesNERVIO OPTICO HIPERTENSIOM CRANEAL 2021Andrea GutierrezNo ratings yet
- Role of High Resolution Ultrasound in Assessment oDocument16 pagesRole of High Resolution Ultrasound in Assessment oilham Maulana ArifNo ratings yet
- Schmidt2020 Article SynergisticEffectsOfForensicMeDocument12 pagesSchmidt2020 Article SynergisticEffectsOfForensicMeLanny Dwi ChandraNo ratings yet
- Prosch2012 (Jurnal 7)Document11 pagesProsch2012 (Jurnal 7)MayNo ratings yet
- Temporal Bone Imaging: Comparison of Flat Panel Volume CT and Multisection CTDocument6 pagesTemporal Bone Imaging: Comparison of Flat Panel Volume CT and Multisection CTNovi DwiyantiNo ratings yet
- CT vs DSA for intracranial vascular pathologyDocument9 pagesCT vs DSA for intracranial vascular pathologyPari Pengda BaliNo ratings yet
- The Roof of The Labyrinthine Facial Nerve Canal and The Geniculate Ganglion Fossa On High-Resolution Computed Tomography - Dehiscence Thickness and PneumatizationDocument11 pagesThe Roof of The Labyrinthine Facial Nerve Canal and The Geniculate Ganglion Fossa On High-Resolution Computed Tomography - Dehiscence Thickness and PneumatizationSa'Deu FondjoNo ratings yet
- Lung BiopsyDocument8 pagesLung BiopsySiya PatilNo ratings yet
- Presentation 01Document15 pagesPresentation 01KDNo ratings yet
- Tumor in Dogs StudyDocument8 pagesTumor in Dogs StudyMikeNo ratings yet
- Abstract No. 301 - Angiographic Catheters - A Comprehensive Review For The Interventionalist In-TrainingDocument2 pagesAbstract No. 301 - Angiographic Catheters - A Comprehensive Review For The Interventionalist In-TrainingPeter LiNo ratings yet
- Yoon 2021Document5 pagesYoon 2021Muhammad Azhar ImranNo ratings yet
- Diagnostic Accuracy of Oblique Chest Radiograph For Occult Pneumothorax: Comparison With UltrasonographyDocument7 pagesDiagnostic Accuracy of Oblique Chest Radiograph For Occult Pneumothorax: Comparison With UltrasonographyVirni AprieliaNo ratings yet
- The Pattern and Prevalence of Vertebral Artery Injury in Patients With Cervical Spine FracturesDocument4 pagesThe Pattern and Prevalence of Vertebral Artery Injury in Patients With Cervical Spine FracturesFrontiersNo ratings yet
- The Potential For Undertaking Slow CT Using A Modern CT ScannerDocument7 pagesThe Potential For Undertaking Slow CT Using A Modern CT ScannerAndreas RonaldNo ratings yet
- VIRTOPSY The Swiss Virtual Autopsy ApproachDocument5 pagesVIRTOPSY The Swiss Virtual Autopsy ApproachgarethNo ratings yet
- 2Document17 pages2fikryahNo ratings yet
- 3D cone-beam CT of the ankle using a novel twin robotic X-ray systemDocument7 pages3D cone-beam CT of the ankle using a novel twin robotic X-ray systemanderson.mancianoNo ratings yet
- 1357 FullDocument8 pages1357 FullPaulius GecasNo ratings yet
- Endoskopik 2.brankialDocument5 pagesEndoskopik 2.brankialDogukan DemirNo ratings yet
- CT Scan in VeterinaryDocument4 pagesCT Scan in VeterinarySurajNo ratings yet
- Xie2013 PDFDocument8 pagesXie2013 PDFAmril MukminNo ratings yet
- 10.1007@s00068 019 01274 3Document10 pages10.1007@s00068 019 01274 3Mylda PratiwiNo ratings yet
- 586 2012 Article 2505Document6 pages586 2012 Article 2505sulthoni ikaNo ratings yet
- Accuracy and Longitudinal Reproducibility of QuantDocument18 pagesAccuracy and Longitudinal Reproducibility of QuantChristian Huapaya ContrerasNo ratings yet
- Zumsteg Et Al 2015Document8 pagesZumsteg Et Al 2015Alyssa Anne GrandaNo ratings yet
- Imaging in Polytrauma e Principles and Current ConceptsDocument8 pagesImaging in Polytrauma e Principles and Current ConceptsJJCONo ratings yet
- Schimming, Eckelt e Kittner (1999) The Value of Coronal Computer Tomograms in Fractures of The Mandibular Condylar ProcessDocument8 pagesSchimming, Eckelt e Kittner (1999) The Value of Coronal Computer Tomograms in Fractures of The Mandibular Condylar ProcessSamádhi FugitaNo ratings yet
- Indications For Bullet Removal: Overview of The Literature, and Clinical Practice Guidelines For European Trauma SurgeonsDocument5 pagesIndications For Bullet Removal: Overview of The Literature, and Clinical Practice Guidelines For European Trauma SurgeonsTefera LeteboNo ratings yet
- Gonfiotti A 2010 PDFDocument7 pagesGonfiotti A 2010 PDFOliver BlandyNo ratings yet
- Rti 0000000000000180Document4 pagesRti 0000000000000180kennyNo ratings yet
- The Impact of F-FDG PET/CT On Assessment of Nasopharyngeal Carcinoma at DiagnosisDocument9 pagesThe Impact of F-FDG PET/CT On Assessment of Nasopharyngeal Carcinoma at DiagnosisAqsha AmandaNo ratings yet
- 2023 TrungluDocument9 pages2023 Trungludr.speleologNo ratings yet
- Aortaresektion Marulli 2015Document6 pagesAortaresektion Marulli 2015t.krbekNo ratings yet
- Korir 2015Document11 pagesKorir 2015Rimo RimoNo ratings yet
- Ijss Oct Oa25 PDFDocument5 pagesIjss Oct Oa25 PDFGonçalo Cunha-CoutinhoNo ratings yet
- Role of Bedside Ultrasonography in Detecting Occult PneumothoraxDocument23 pagesRole of Bedside Ultrasonography in Detecting Occult PneumothoraxMukhizalNo ratings yet
- Fraktur FrakDocument11 pagesFraktur FrakRirin SeptianiNo ratings yet
- Damme Rer 2021Document10 pagesDamme Rer 2021son leNo ratings yet
- 2022 - Haske - The Immo Traffic Light SystemDocument11 pages2022 - Haske - The Immo Traffic Light SystemScience BrasilNo ratings yet
- Corbacioglu SerefDocument6 pagesCorbacioglu SerefFabio Antonio Villadiego FontanillaNo ratings yet
- 1530 Jul 27Document6 pages1530 Jul 27kelvin amahNo ratings yet
- Modified 2 CM Super Single Port vs. The Traditional 3 CM Single Port For Video Assisted Thoracoscopic Surgery LobectomyDocument8 pagesModified 2 CM Super Single Port vs. The Traditional 3 CM Single Port For Video Assisted Thoracoscopic Surgery LobectomyAlin Ionut BurlacuNo ratings yet
- Evaluation of Blunt Chest Trauma With Multidetector Computed TomographyDocument4 pagesEvaluation of Blunt Chest Trauma With Multidetector Computed TomographyasclepiuspdfsNo ratings yet
- Pon XDocument6 pagesPon XMillerNo ratings yet
- Clavicle Fracture Following Neck Dissection: Imaging Features and Natural CourseDocument6 pagesClavicle Fracture Following Neck Dissection: Imaging Features and Natural CourseAngel IschiaNo ratings yet
- DownloadDocument9 pagesDownloadhasan nazzalNo ratings yet
- Clinical Application CTDocument40 pagesClinical Application CTWalaa MajeedNo ratings yet
- Radiology in Forensic Medicine: From Identification to Post-mortem ImagingFrom EverandRadiology in Forensic Medicine: From Identification to Post-mortem ImagingGiuseppe Lo ReNo ratings yet
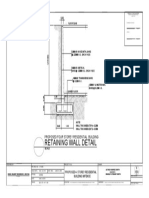
- Retaining Wall DetailsDocument1 pageRetaining Wall DetailsWilbert ReuyanNo ratings yet
- Business Judgment Rule and Directors' Duty to Inform in Smith v Van GorkomDocument1 pageBusiness Judgment Rule and Directors' Duty to Inform in Smith v Van GorkomDorothy ParkerNo ratings yet
- Computer ViruesDocument19 pagesComputer ViruesMuhammad Adeel AnsariNo ratings yet
- Sem Iii Sybcom Finacc Mang AccDocument6 pagesSem Iii Sybcom Finacc Mang AccKishori KumariNo ratings yet
- Learn To Hear The Voice of GodDocument110 pagesLearn To Hear The Voice of Godtrue prophet100% (1)
- Definition and Scope of Public FinanceDocument2 pagesDefinition and Scope of Public FinanceArfiya MubeenNo ratings yet
- Bahasa Inggris Kelas XIIDocument2 pagesBahasa Inggris Kelas XIIMuhammad ImadudinNo ratings yet
- B.Ed Syllabus NEW 2015-16 PDFDocument170 pagesB.Ed Syllabus NEW 2015-16 PDFVikas KuthadiNo ratings yet
- Health Fitness Guide UK 2018 MayDocument100 pagesHealth Fitness Guide UK 2018 MayMitch Yeoh100% (2)
- Pharmacology Ain Shams 123 - Compress 1Document552 pagesPharmacology Ain Shams 123 - Compress 1ahmed hoty100% (1)
- YlideDocument13 pagesYlidePharaoh talk to youNo ratings yet
- Engagement LetterDocument1 pageEngagement LetterCrystal Jenn Balaba100% (1)
- FMAI - Ch04 - Stock MarketDocument105 pagesFMAI - Ch04 - Stock Marketngoc duongNo ratings yet
- Batt ChargerDocument2 pagesBatt Chargerdjoko witjaksonoNo ratings yet
- The Accidental AddictsDocument6 pagesThe Accidental AddictsnorthandsouthnzNo ratings yet
- DWDM Route Planning A4 WPDocument3 pagesDWDM Route Planning A4 WPChavara MatekweNo ratings yet
- MaheshDocument20 pagesMaheshParthNo ratings yet
- 9284 - Technical Instruction Addenum 3 Corrigendum 2Document5 pages9284 - Technical Instruction Addenum 3 Corrigendum 2Bambang HerimantoNo ratings yet
- Plant Chicago 2Document4 pagesPlant Chicago 2api-321978505No ratings yet
- Quantification Skills in The Construction IndustryDocument34 pagesQuantification Skills in The Construction IndustryBRGRNo ratings yet
- Mercury Poisoning Symptoms and TreatmentsDocument1 pageMercury Poisoning Symptoms and TreatmentsRakheeb BashaNo ratings yet
- GSAA HET 2005-15, Tranche B2 / BSABS 2005-TC2, Tranche M6 Shown As An Asset of Maiden LaneDocument122 pagesGSAA HET 2005-15, Tranche B2 / BSABS 2005-TC2, Tranche M6 Shown As An Asset of Maiden LaneTim BryantNo ratings yet
- Arduino Programming Step by Step Guide To Mastering Arduino Hardware and SoftwareDocument109 pagesArduino Programming Step by Step Guide To Mastering Arduino Hardware and SoftwareMohan100% (3)
- Lesson 2Document10 pagesLesson 2angeliquefaithemnaceNo ratings yet
- Tle 10 4quarterDocument2 pagesTle 10 4quarterCaryll BaylonNo ratings yet
- Radio Codes and ConventionsDocument2 pagesRadio Codes and Conventionsapi-570661298No ratings yet
- Phy Worksheet IG 3 Phase 2Document6 pagesPhy Worksheet IG 3 Phase 2Umair RazaNo ratings yet
- UnitTest D10 Feb 2024Document26 pagesUnitTest D10 Feb 2024dev.shah8038No ratings yet
- Su1 Assessment U01Document14 pagesSu1 Assessment U01Cristian Seas ArceNo ratings yet