You might also like
- NANOTECHNOLOGY REVIEW: LIPOSOMES, NANOTUBES & PLGA NANOPARTICLESFrom EverandNANOTECHNOLOGY REVIEW: LIPOSOMES, NANOTUBES & PLGA NANOPARTICLESNo ratings yet
- Profhilo - Reologia e CitotoxicidadeDocument20 pagesProfhilo - Reologia e CitotoxicidadeRhelvis1No ratings yet
- Midfacial Rejuvenation by Hyaluronic Acid Fillers and Subcutaneous Adipose Tissue - A New ConceptDocument4 pagesMidfacial Rejuvenation by Hyaluronic Acid Fillers and Subcutaneous Adipose Tissue - A New ConceptArcelino FariasNo ratings yet
- 2016 Lagatta Rheology ALLIAXINDocument8 pages2016 Lagatta Rheology ALLIAXINANDRÉ CAMARGONo ratings yet
- Polymers 15 02438Document13 pagesPolymers 15 02438Stefy BîrjovanuNo ratings yet
- Ccid 10 431Document10 pagesCcid 10 431Ananda SantosNo ratings yet
- Anti-Aging and Depigmentation Effect of A Hyaluronic AcidDocument13 pagesAnti-Aging and Depigmentation Effect of A Hyaluronic AcidkdsmphNo ratings yet
- In - A Randomized Split Face Histomorphologic Study Comparing A Volumetric Calcium Hydroxylapatite and A Hyaluronic Acid Based Dermal FillerDocument6 pagesIn - A Randomized Split Face Histomorphologic Study Comparing A Volumetric Calcium Hydroxylapatite and A Hyaluronic Acid Based Dermal FillerFrancisco BotelhoNo ratings yet
- Jacovella2006 - CópiaDocument13 pagesJacovella2006 - CópiaVanessa Müller BardiniNo ratings yet
- Jurnal Pelesap Obat Sediaan TopikalDocument10 pagesJurnal Pelesap Obat Sediaan TopikalmarthagusnadiNo ratings yet
- Collagen StimulatorsDocument11 pagesCollagen StimulatorsElizabeth TovittoNo ratings yet
- Profhilo - Reologia 2Document20 pagesProfhilo - Reologia 2Rhelvis1No ratings yet
- Ccid 13 31Document18 pagesCcid 13 31Ananda SantosNo ratings yet
- MICROBOTOXDocument7 pagesMICROBOTOXFabianaNisanNo ratings yet
- Probiotic CreamDocument8 pagesProbiotic Creamirwan junNo ratings yet
- Gabriela Casabona Histological Effects of A CombinedDocument7 pagesGabriela Casabona Histological Effects of A CombinedHayley NicNo ratings yet
- reologiaDocument12 pagesreologiaJohn LacerdaNo ratings yet
- Polymers 03 00509 v2Document18 pagesPolymers 03 00509 v2Branko BabicNo ratings yet
- Hyaluronic Acid Beyond Skin Rejuvenation: The Intersection Between Beauty and Safety in Compliance With The New Eu Medical Devices RegulationDocument9 pagesHyaluronic Acid Beyond Skin Rejuvenation: The Intersection Between Beauty and Safety in Compliance With The New Eu Medical Devices RegulationIJAR JOURNALNo ratings yet
- 10 1097@DSS 0000000000001281Document11 pages10 1097@DSS 0000000000001281plastic guardiansNo ratings yet
- Thehyaluronicacid Fillers: Current Understanding of The Tissue Device InterfaceDocument10 pagesThehyaluronicacid Fillers: Current Understanding of The Tissue Device InterfaceLuis Fernando WeffortNo ratings yet
- Preparation of Transparent Starch Based Hydrogel MDocument10 pagesPreparation of Transparent Starch Based Hydrogel MRoNo ratings yet
- Dermatologic Therapy - 2022 - WongprasertDocument9 pagesDermatologic Therapy - 2022 - Wongprasertdocrubes50No ratings yet
- Fillers For Aesthetics On The Face Newer PerspectivesDocument7 pagesFillers For Aesthetics On The Face Newer PerspectiveshilderhNo ratings yet
- Biochemical and Physical Actions of Hyaluronic Acid Delivered by Intradermal Jet Injection RouteDocument8 pagesBiochemical and Physical Actions of Hyaluronic Acid Delivered by Intradermal Jet Injection RouteRosélia DutraNo ratings yet
- Modif Structure of HADocument6 pagesModif Structure of HAnina asrianaNo ratings yet
- Targeting Facial Aging With Nano and Regenerative Technologies and ProceduresDocument8 pagesTargeting Facial Aging With Nano and Regenerative Technologies and ProceduresAle EstradaNo ratings yet
- Bio MetilDocument20 pagesBio Metilsimone toledoNo ratings yet
- SF - Hydrogel - Hypertrophic ScarsDocument9 pagesSF - Hydrogel - Hypertrophic ScarsOana MariaNo ratings yet
- Sjad 173Document28 pagesSjad 173cocooakNo ratings yet
- An Approach To Structural Facial Rejuvenation With Fillers in WomenDocument15 pagesAn Approach To Structural Facial Rejuvenation With Fillers in WomenJhon RodriguezNo ratings yet
- Journal Pre-Proof: International Journal of Biological MacromoleculesDocument67 pagesJournal Pre-Proof: International Journal of Biological MacromoleculesPaulo Emílio Alves AlvesNo ratings yet
- jfb-14-00082Document14 pagesjfb-14-00082Vishwajeet GhorpadeNo ratings yet
- Effects of Hydrolysed Collagen Associated or Not With Physical AgentsDocument17 pagesEffects of Hydrolysed Collagen Associated or Not With Physical Agentssilvia roca mejiaNo ratings yet
- J of Cosmetic Dermatology - 2023 - Palauro - Innovation of The Protocol For The Application of Cryolipolysis Effects andDocument9 pagesJ of Cosmetic Dermatology - 2023 - Palauro - Innovation of The Protocol For The Application of Cryolipolysis Effects andPaolaNo ratings yet
- Consenso Brasileiro Sculptra CorporalDocument7 pagesConsenso Brasileiro Sculptra CorporalAndré Mauricio Freire Pires100% (1)
- Carboxi Regeneracion de ColagenoDocument6 pagesCarboxi Regeneracion de ColagenoContacto AllA-MedicalNo ratings yet
- The Role of Hyaluronidase For The Skin Necrosis Caused by Hyaluronic Acid Injection-Induced Embolism: A Rabbit Auricular Model StudyDocument9 pagesThe Role of Hyaluronidase For The Skin Necrosis Caused by Hyaluronic Acid Injection-Induced Embolism: A Rabbit Auricular Model Studyj_a_simoesNo ratings yet
- An Overview of Permanent and Semipermanent Fillers: SummaryDocument8 pagesAn Overview of Permanent and Semipermanent Fillers: SummaryArmin ArceoNo ratings yet
- Topical Caffeine For Sellit PDFDocument10 pagesTopical Caffeine For Sellit PDFMamakNya VidyaNo ratings yet
- Aloevera PDFDocument9 pagesAloevera PDFDeimer OrtizNo ratings yet
- Formulation Optimization of EGCG-Loaded Self-Double Emulsifying Drug Delivery System for Transdermal DeliveryDocument12 pagesFormulation Optimization of EGCG-Loaded Self-Double Emulsifying Drug Delivery System for Transdermal DeliveryMheliendha Cyank Z'muanyaNo ratings yet
- Medicina 57 00285Document11 pagesMedicina 57 00285Siti Zahra MaharaniNo ratings yet
- Viskositas HECDocument10 pagesViskositas HECVANESA WIRAMASNo ratings yet
- Ccid 13 701Document10 pagesCcid 13 701jess.sooares12No ratings yet
- Materials Science & Engineering C: SciencedirectDocument12 pagesMaterials Science & Engineering C: Sciencedirectkaushita banerjeeNo ratings yet
- Dexamethasone-Loaded Ureasil Hydrophobic Membrane For Bone Guided RegenerationDocument16 pagesDexamethasone-Loaded Ureasil Hydrophobic Membrane For Bone Guided RegenerationJoao Augusto Oshiro JuniorNo ratings yet
- Uso Concomitante de Ácido Hialurônico e Laser No Rejuvenescimento FacialDocument10 pagesUso Concomitante de Ácido Hialurônico e Laser No Rejuvenescimento Facialstephane beatrizNo ratings yet
- Sunekos Clinical-StudiesDocument6 pagesSunekos Clinical-StudiesGustavo Henrique MüllerNo ratings yet
- Benefits of Topical Hyaluronic Acid For Skin Quality and Signs of Skin Aging: From Literature Review To Clinical EvidenceDocument9 pagesBenefits of Topical Hyaluronic Acid For Skin Quality and Signs of Skin Aging: From Literature Review To Clinical EvidenceНадія АсадуллаєваNo ratings yet
- Rodriguez 2018Document7 pagesRodriguez 2018Bianca CampitelliNo ratings yet
- Ijms 23 08114 v2Document26 pagesIjms 23 08114 v2Marcia GouveiaNo ratings yet
- Science of Hyaluronic Acid Beyond Filling - Fibroblasts and Their Response To The Extracellular MatrixDocument8 pagesScience of Hyaluronic Acid Beyond Filling - Fibroblasts and Their Response To The Extracellular MatrixAnonymous LnWIBo1GNo ratings yet
- Thesis On Transdermal Drug Delivery SystemDocument8 pagesThesis On Transdermal Drug Delivery SystemOrderPapersOnlineWorcester100% (2)
- Formulation and Evaluation of Ketoconazole NiosomaDocument7 pagesFormulation and Evaluation of Ketoconazole NiosomaKevin Nauval KarimNo ratings yet
- Rheology Filler JurnalDocument6 pagesRheology Filler JurnalRobertoNo ratings yet
- Gels 10 00188Document46 pagesGels 10 00188mkhubaibNo ratings yet
- -Caryophyllene-Loaded Microemulsion-Based Topical Hydrogel: A Promising Carrier to Enhance the Analgesic and Anti-Inflammatory OutcomesDocument16 pages-Caryophyllene-Loaded Microemulsion-Based Topical Hydrogel: A Promising Carrier to Enhance the Analgesic and Anti-Inflammatory OutcomesVishwajeet GhorpadeNo ratings yet
- Role_of_porous_siliconhydrogel_composites_on_drug_Document9 pagesRole_of_porous_siliconhydrogel_composites_on_drug_Quế NghiNo ratings yet
- 2016 Fabbroncini 1Document5 pages2016 Fabbroncini 1ANDRÉ CAMARGONo ratings yet
- Ostenil ReologiaDocument24 pagesOstenil ReologiaRhelvis1No ratings yet
- Profhilo - CaracteristicasDocument15 pagesProfhilo - CaracteristicasRhelvis1No ratings yet
- US8822676Document20 pagesUS8822676Rhelvis1No ratings yet
- Wu2016 Article ClinicalComparisonBetweenTwoHyDocument7 pagesWu2016 Article ClinicalComparisonBetweenTwoHyRhelvis1No ratings yet
- Comparison ListDocument1 pageComparison ListRhelvis1No ratings yet
- 140-Article Text-551-1-10-20171022Document1 page140-Article Text-551-1-10-20171022Rhelvis1No ratings yet
- Reologia Do Restylane FinesseDocument8 pagesReologia Do Restylane FinesseRhelvis1No ratings yet
- Tamanho de Particula RestylaneDocument7 pagesTamanho de Particula RestylaneRhelvis1No ratings yet
- Tamanho de Particula RestylaneDocument7 pagesTamanho de Particula RestylaneRhelvis1No ratings yet
- Teste Com HialuronidaseDocument9 pagesTeste Com HialuronidaseRhelvis1No ratings yet
- XLL TH STD Bio-Zoology Practical Manual EM PDFDocument23 pagesXLL TH STD Bio-Zoology Practical Manual EM PDFDilli Babu60% (10)
- Somatoform DisordersDocument43 pagesSomatoform DisordersChristopher El MouhayyarNo ratings yet
- Eduardo Mondlane University Veterinary Faculty Course: Food Science and Technology Subject: English For Science 2º Level, 2º SemesterDocument8 pagesEduardo Mondlane University Veterinary Faculty Course: Food Science and Technology Subject: English For Science 2º Level, 2º SemesterAdriano RafaelNo ratings yet
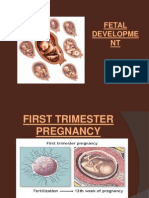
- Fetal DevelopmentDocument33 pagesFetal DevelopmentAnnapurna DangetiNo ratings yet
- You Can Grow Your IntelligenceDocument6 pagesYou Can Grow Your IntelligenceSoniaNo ratings yet
- ДокументDocument72 pagesДокументDianna ArzumanovaNo ratings yet
- Brain Chips Seminar ReportDocument3 pagesBrain Chips Seminar ReportPrince TreasureNo ratings yet
- Erasmus Rotterdam University MCDocument24 pagesErasmus Rotterdam University MCAndreea CroitoruNo ratings yet
- Download ebook Principles Of Tissue Engineering Pdf full chapter pdfDocument67 pagesDownload ebook Principles Of Tissue Engineering Pdf full chapter pdfbernard.moore610100% (20)
- Atlas Histology of HeartDocument2 pagesAtlas Histology of HeartYasir HadyNo ratings yet
- (Modern Genetics, V. 2) Alan F Wright - Barrie Jay-Molecular Genetics of Inherited Eye Disorders-Harwood Academic (1994)Document531 pages(Modern Genetics, V. 2) Alan F Wright - Barrie Jay-Molecular Genetics of Inherited Eye Disorders-Harwood Academic (1994)fawad ullahNo ratings yet
- PBL Report ThalassemiaDocument10 pagesPBL Report Thalassemiasarah_amigurlz88100% (2)
- Exercise 6Document10 pagesExercise 6Erika Mae Sta MariaNo ratings yet
- Parkinson's Disease - Wikipedia, The Free EncyclopediaDocument15 pagesParkinson's Disease - Wikipedia, The Free Encyclopediaopathena04No ratings yet
- Hem Lab3 Blood Smears F10Document10 pagesHem Lab3 Blood Smears F10Luke Hsu0% (1)
- LabreportnewDocument2 pagesLabreportnewRai Media TechnologiesNo ratings yet
- Cancer: Current scenario, strategies and projections for 2015Document7 pagesCancer: Current scenario, strategies and projections for 2015smbawasainiNo ratings yet
- 1700 Ebook DiseasesDocument250 pages1700 Ebook DiseasesAhmad Arif100% (1)
- ASD Comparison 092214Document6 pagesASD Comparison 092214Hemant KumarNo ratings yet
- Sars-Cov-2 (Qualitative RTPCR) : Nasopharyngeal / Oropharyngeal SwabDocument2 pagesSars-Cov-2 (Qualitative RTPCR) : Nasopharyngeal / Oropharyngeal SwabNaushadNo ratings yet
- Stuck in A Rut: Rethinking Depression and Its Treatment: Paul E. Holtzheimer and Helen S. MaybergDocument9 pagesStuck in A Rut: Rethinking Depression and Its Treatment: Paul E. Holtzheimer and Helen S. MaybergIlias MaNo ratings yet
- Dentinogenesis imperfecta causes dark tooth discolorationDocument4 pagesDentinogenesis imperfecta causes dark tooth discolorationmirfanulhaq100% (1)
- Bortolato2016 Depresi Pada KankerDocument50 pagesBortolato2016 Depresi Pada KankerYudha HudayaNo ratings yet
- IVIGDocument7 pagesIVIGPeraNo ratings yet
- Recent Advances in Retinoblastoma Management and GeneticsDocument12 pagesRecent Advances in Retinoblastoma Management and GeneticsDr Pranesh BalasubramaniamNo ratings yet
- YogaDocument12 pagesYogaRahfyahamedNo ratings yet
- DermatomyositisDocument4 pagesDermatomyositisLakshya J BasumataryNo ratings yet
- Science 1987 Slamon 177 82 PDFDocument6 pagesScience 1987 Slamon 177 82 PDFAmin ArabNo ratings yet
- All of These: C) Production of Virus Free PlantsDocument15 pagesAll of These: C) Production of Virus Free PlantsGufran AnsariNo ratings yet
- High School Biology ReviewerDocument26 pagesHigh School Biology ReviewerPatricia SioNo ratings yet