You might also like
- Recent Trends in Computer-aided Diagnostic Systems for Skin Diseases: Theory, Implementation, and AnalysisFrom EverandRecent Trends in Computer-aided Diagnostic Systems for Skin Diseases: Theory, Implementation, and AnalysisNo ratings yet
- Hybrid Approach For Skin Disease Classification Integrating Machine Learning and Deep LearningDocument8 pagesHybrid Approach For Skin Disease Classification Integrating Machine Learning and Deep LearningIJRASETPublicationsNo ratings yet
- Electronics 10 03158 v2Document29 pagesElectronics 10 03158 v2Abdulahi AbebeNo ratings yet
- An Automatic Dermatology Detection System Based On Deep Learning and Computer VisionDocument10 pagesAn Automatic Dermatology Detection System Based On Deep Learning and Computer VisionSURYA PRAKASH K ITNo ratings yet
- Applied SciencesDocument21 pagesApplied Sciencesseyfu mogesNo ratings yet
- Melanoma Disease Detection and Classification Using Deep LearningDocument11 pagesMelanoma Disease Detection and Classification Using Deep LearningIJRASETPublicationsNo ratings yet
- Skin Disease Detection Using Machine LearningDocument6 pagesSkin Disease Detection Using Machine LearningIJRASETPublicationsNo ratings yet
- Diagnostics 13 03147 v2Document40 pagesDiagnostics 13 03147 v2SURYA PRAKASH K ITNo ratings yet
- JETIR2312164Document6 pagesJETIR2312164Divya WaghmareNo ratings yet
- 5 A Machine Learning Approach For Skin Disease Detection and 2022 HealthcareDocument15 pages5 A Machine Learning Approach For Skin Disease Detection and 2022 HealthcarePaul Awinpang GodswayNo ratings yet
- Skin Lesions Detection Using Deep Learning TechniquesDocument5 pagesSkin Lesions Detection Using Deep Learning TechniquesIJRASETPublicationsNo ratings yet
- Skin Cancer Detection Using Deep Learning TechniquesDocument11 pagesSkin Cancer Detection Using Deep Learning TechniquesIJRASETPublicationsNo ratings yet
- Skin Cancer ClassificationDocument7 pagesSkin Cancer ClassificationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Identification and Classification of Skin Cancer Using A GUI and A Deep Neural NetworkDocument14 pagesIdentification and Classification of Skin Cancer Using A GUI and A Deep Neural NetworkIJRASETPublicationsNo ratings yet
- Research PaperDocument4 pagesResearch Paperlakshyaggarwal18sepNo ratings yet
- AlexNet and DenseNet-121-Based Hybrid CNN Architecture For Skin Cancer Prediction From Dermoscopic ImagesDocument11 pagesAlexNet and DenseNet-121-Based Hybrid CNN Architecture For Skin Cancer Prediction From Dermoscopic ImagesIJRASETPublicationsNo ratings yet
- Artificial Intelligence in Cosmetic Dermatology ADocument21 pagesArtificial Intelligence in Cosmetic Dermatology ArhsiboneyNo ratings yet
- 1a85 PDFDocument9 pages1a85 PDFHedinyer MauricioNo ratings yet
- Sensors: Classification of Skin Disease Using Deep Learning Neural Networks With Mobilenet V2 and LSTMDocument27 pagesSensors: Classification of Skin Disease Using Deep Learning Neural Networks With Mobilenet V2 and LSTMtemp 22No ratings yet
- A Convolutional Neural Network Framework For AccurDocument22 pagesA Convolutional Neural Network Framework For AccurDiti DivekarNo ratings yet
- (IJCST-V10I3P38) :ameena K A, Aparna K, Aysha C R, Nazana P N, Vidya HariDocument9 pages(IJCST-V10I3P38) :ameena K A, Aparna K, Aysha C R, Nazana P N, Vidya HariEighthSenseGroupNo ratings yet
- Fsurg 09 1029991Document9 pagesFsurg 09 1029991Juanito AlojNo ratings yet
- Computers in Biology and Medicine: Manu Goyal, Thomas Knackstedt, Shaofeng Yan, Saeed HassanpourDocument11 pagesComputers in Biology and Medicine: Manu Goyal, Thomas Knackstedt, Shaofeng Yan, Saeed Hassanpourchandranv76No ratings yet
- Efficient Fusion of Handcrafted and Pre-Trained Cnns Features To Classify Melanoma Skin CancerDocument20 pagesEfficient Fusion of Handcrafted and Pre-Trained Cnns Features To Classify Melanoma Skin CancerMd. Sazzad Mia 191-15-2503No ratings yet
- Bjro 20190037Document8 pagesBjro 20190037GPTV AdmissionsNo ratings yet
- Preprints202206 0384 v1Document12 pagesPreprints202206 0384 v1rakeshsinghpariharNo ratings yet
- 1 s2.0 S2352914819302047 Main PDFDocument6 pages1 s2.0 S2352914819302047 Main PDFAysha ShabbirNo ratings yet
- Paper 8661Document2 pagesPaper 8661IJARSCT JournalNo ratings yet
- Skin Lesion Classification From Dermoscopy and Clinical Images With A Deep Learning ApproachDocument7 pagesSkin Lesion Classification From Dermoscopy and Clinical Images With A Deep Learning ApproachIJAR JOURNALNo ratings yet
- 1 s2.0 S2772442523000102 MainDocument12 pages1 s2.0 S2772442523000102 MainSURYA PRAKASH K ITNo ratings yet
- Computer Vision For Skin Cancer Diagnosis and Recognition Using RBF and SOMDocument9 pagesComputer Vision For Skin Cancer Diagnosis and Recognition Using RBF and SOMAI Coordinator - CSC JournalsNo ratings yet
- Skin Diseases Detection Using LBP and WLD-An Ensembling ApproachDocument24 pagesSkin Diseases Detection Using LBP and WLD-An Ensembling ApproachCarmen OrellanaNo ratings yet
- Literature Paper (Copy)Document7 pagesLiterature Paper (Copy)A To Z INFONo ratings yet
- 169 Melanoma Skin Cancer Detection Using Image Processing and Machine Learning20190703-23098-1o8hr8x-With-cover-page-V2Document6 pages169 Melanoma Skin Cancer Detection Using Image Processing and Machine Learning20190703-23098-1o8hr8x-With-cover-page-V2Md. Sazzad Mia 191-15-2503No ratings yet
- Dermatologist Level Dermoscopy Skin Cancer Classification Using Different Deep Learning Convolutional Neural Networks Algorithms - RezvantalabDocument15 pagesDermatologist Level Dermoscopy Skin Cancer Classification Using Different Deep Learning Convolutional Neural Networks Algorithms - RezvantalabEshtiaqul HaqueNo ratings yet
- Skin Lesion Classification Based On ConvolutionalDocument6 pagesSkin Lesion Classification Based On ConvolutionalAnchal SharmaNo ratings yet
- Deep Learning Based Skin Diseases Classification Using SmartphonesDocument11 pagesDeep Learning Based Skin Diseases Classification Using Smartphonesbvkarthik2711No ratings yet
- Melanoma Skin Cancer Detection Using Image Processing and Machine LearningDocument5 pagesMelanoma Skin Cancer Detection Using Image Processing and Machine LearningEditor IJTSRDNo ratings yet
- Literature Survey On Skin Lesion ClassificationDocument7 pagesLiterature Survey On Skin Lesion ClassificationIJRASETPublicationsNo ratings yet
- Smartphone Assisted Artificial Intelligence in Dermatology A Novel Approach To Help General Practitioners in Underserved AreasDocument3 pagesSmartphone Assisted Artificial Intelligence in Dermatology A Novel Approach To Help General Practitioners in Underserved AreasAthenaeum Scientific PublishersNo ratings yet
- Identification of Cancerous Cell From Noisy ImagesDocument5 pagesIdentification of Cancerous Cell From Noisy ImagesIJRASETPublicationsNo ratings yet
- A Proposed Architecture For Convolutional Neural Networks To Detect Skin CancersDocument9 pagesA Proposed Architecture For Convolutional Neural Networks To Detect Skin CancersIAES IJAINo ratings yet
- DeepSkin A Deep Learning Approach For Skin Cancer ClassificationDocument10 pagesDeepSkin A Deep Learning Approach For Skin Cancer ClassificationShivam MaheshNo ratings yet
- An Efficient Deep Learning-Based Skin Cancer Classifier For An Imbalanced DatasetDocument16 pagesAn Efficient Deep Learning-Based Skin Cancer Classifier For An Imbalanced DatasetenthusiasticroseNo ratings yet
- Research Article: Skin Disease Recognition Method Based On Image Color and Texture FeaturesDocument11 pagesResearch Article: Skin Disease Recognition Method Based On Image Color and Texture FeaturesAYUSH KUMARNo ratings yet
- Boundary Tracing Algorithm For Automatic Skin Lesion Detection in Macroscopic ImagesDocument9 pagesBoundary Tracing Algorithm For Automatic Skin Lesion Detection in Macroscopic ImagesKranthirekha ChennaboinaNo ratings yet
- Automated System To Classify and Detect The Skin LesionDocument5 pagesAutomated System To Classify and Detect The Skin LesionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Applied SciencesDocument20 pagesApplied Sciencesseyfu mogesNo ratings yet
- Skin Cancer Detection and Classification Using GUI and Deep Neural NetworkDocument11 pagesSkin Cancer Detection and Classification Using GUI and Deep Neural NetworkIJRASETPublicationsNo ratings yet
- IJETR041117Document4 pagesIJETR041117erpublicationNo ratings yet
- FaceDocument39 pagesFaceALNATRON GROUPSNo ratings yet
- 3.. Malignant Melanoma Classification Using Deep Learning Datasets, Performance Measurements, Challenges and OpportunitiesDocument25 pages3.. Malignant Melanoma Classification Using Deep Learning Datasets, Performance Measurements, Challenges and OpportunitiesMuhammad Awais QureshiNo ratings yet
- Artificial Intelligence For Skin Cancer Detection and Classification For Clinical Environment: A Systematic ReviewDocument13 pagesArtificial Intelligence For Skin Cancer Detection and Classification For Clinical Environment: A Systematic Reviewmloureiro17No ratings yet
- Automated Skin Lesion Diagnosis and Classification Using Learning AlgorithmsIntelligent Automation and Soft ComputingDocument13 pagesAutomated Skin Lesion Diagnosis and Classification Using Learning AlgorithmsIntelligent Automation and Soft ComputingJesús Isabel Castillo MontesNo ratings yet
- Skin Lesion Detection Using CNNDocument7 pagesSkin Lesion Detection Using CNNInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Zhang Et Al. - 2021 - Opportunities and Challenges Classification of SKDocument14 pagesZhang Et Al. - 2021 - Opportunities and Challenges Classification of SKseyfu mogesNo ratings yet
- A Survey of Feature Extraction in Dermoscopy Image Analysis of Skin CancerDocument14 pagesA Survey of Feature Extraction in Dermoscopy Image Analysis of Skin CancerSUMIT GANGWARNo ratings yet
- Non-Invasive Diagnostic Techniques in DermatologyDocument3 pagesNon-Invasive Diagnostic Techniques in DermatologyVinh ThếNo ratings yet
- A Mobile-Based Skin Disease Identification System Using Convolutional Neural NetworksDocument10 pagesA Mobile-Based Skin Disease Identification System Using Convolutional Neural NetworksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Capstone SynopsisDocument6 pagesCapstone Synopsissmita prajapatiNo ratings yet
- EN - Abhilash Dash - ResumeDocument3 pagesEN - Abhilash Dash - ResumeAbhilash DashNo ratings yet
- HandymanDocument7 pagesHandymanBehailu Teketel Alemu100% (1)
- SSC MTS Mock Test PDF - (English Version)Document23 pagesSSC MTS Mock Test PDF - (English Version)LBKNo ratings yet
- Institute of Space Technology: Assignment 1 - BasicsDocument5 pagesInstitute of Space Technology: Assignment 1 - BasicsAneeqaa AbrarNo ratings yet
- Mathematical Olympiad Series Vol14Document65 pagesMathematical Olympiad Series Vol141paper 1pen100% (1)
- Java, JSF, Mysql and Hibernate Login ProjectDocument7 pagesJava, JSF, Mysql and Hibernate Login ProjectFatema TahaNo ratings yet
- How To: Connect To AXIS Camera StationDocument18 pagesHow To: Connect To AXIS Camera StationYuda YudaNo ratings yet
- Penetration Testing Report PDFDocument19 pagesPenetration Testing Report PDFLikesh ShresthaNo ratings yet
- RSLTE037 - Service Retainability-PLMN-day-rslte LTE19 Reports RSLTE037 xml-2021 02 26-15 53 33 168Document118 pagesRSLTE037 - Service Retainability-PLMN-day-rslte LTE19 Reports RSLTE037 xml-2021 02 26-15 53 33 168Nguyen Quoc DoanNo ratings yet
- SDFC - Active DirectoryDocument82 pagesSDFC - Active DirectoryLouR2011No ratings yet
- Classes and ObjectDocument26 pagesClasses and ObjectPhannaro PLNo ratings yet
- Python CheatSheet - CodeWithHarryDocument19 pagesPython CheatSheet - CodeWithHarryibrahimsiikanderNo ratings yet
- Mathematical Foundations For Data Science: BITS PilaniDocument29 pagesMathematical Foundations For Data Science: BITS PilaniManisha MNo ratings yet
- Fanuc 0i-TD Mate Standard Features and OptionsDocument7 pagesFanuc 0i-TD Mate Standard Features and OptionsTamil SelvanNo ratings yet
- تقرير ادارة مكمنيةDocument9 pagesتقرير ادارة مكمنيةHassan AlaliNo ratings yet
- Pitch DeckDocument23 pagesPitch DeckkameshchakrapaniNo ratings yet
- IELTS Writing Task 1 Vocabulary PDFDocument3 pagesIELTS Writing Task 1 Vocabulary PDFSexavet RafiyevNo ratings yet
- Masibus FIB MAS-AI-U-08-D - R0F - 0515 - Field Interface Board 8 CH Linearised RTD - TC InputDocument2 pagesMasibus FIB MAS-AI-U-08-D - R0F - 0515 - Field Interface Board 8 CH Linearised RTD - TC InputKeval MistryNo ratings yet
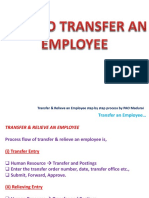
- IFHRMS - Transfer and Relieve An EmployeeDocument26 pagesIFHRMS - Transfer and Relieve An EmployeemangaiyarkarasiNo ratings yet
- Multiband RadioDocument4 pagesMultiband RadioGiorgi RcheulishviliNo ratings yet
- es2000AC SM EN 0006cDocument1,153 pageses2000AC SM EN 0006cshajanachal2006No ratings yet
- CY28447 - ETC PLL Clock Generator DatasheetDocument21 pagesCY28447 - ETC PLL Clock Generator DatasheetewolwentaNo ratings yet
- Practical No 1 Aim Horizontal FragmentatDocument42 pagesPractical No 1 Aim Horizontal FragmentatScientist RPNo ratings yet
- Deep Learning Based Smart Garbage Classifier For Effective Waste ManagementDocument4 pagesDeep Learning Based Smart Garbage Classifier For Effective Waste Managementjuanes torresNo ratings yet
- Scrcpy Commands and ShortcutsDocument9 pagesScrcpy Commands and ShortcutsKaushik SenapatiNo ratings yet
- Introduction To Visual Aids in Technical WritingDocument8 pagesIntroduction To Visual Aids in Technical WritingShivam PathakNo ratings yet
- Future of Social MediaDocument11 pagesFuture of Social MediaShreya AgrahariNo ratings yet
- Machine Learning-Unit-V-NotesDocument23 pagesMachine Learning-Unit-V-NotespalailalithaNo ratings yet
- Muluken KirosDocument62 pagesMuluken KirosSimersen tradingNo ratings yet
- Ivunit Query ProcessingDocument12 pagesIvunit Query ProcessingKeshava VarmaNo ratings yet
- Generative AI: The Insights You Need from Harvard Business ReviewFrom EverandGenerative AI: The Insights You Need from Harvard Business ReviewRating: 4.5 out of 5 stars4.5/5 (3)
- The Master Algorithm: How the Quest for the Ultimate Learning Machine Will Remake Our WorldFrom EverandThe Master Algorithm: How the Quest for the Ultimate Learning Machine Will Remake Our WorldRating: 4.5 out of 5 stars4.5/5 (107)
- HBR's 10 Must Reads on AI, Analytics, and the New Machine AgeFrom EverandHBR's 10 Must Reads on AI, Analytics, and the New Machine AgeRating: 4.5 out of 5 stars4.5/5 (69)
- Working with AI: Real Stories of Human-Machine Collaboration (Management on the Cutting Edge)From EverandWorking with AI: Real Stories of Human-Machine Collaboration (Management on the Cutting Edge)Rating: 5 out of 5 stars5/5 (5)
- Four Battlegrounds: Power in the Age of Artificial IntelligenceFrom EverandFour Battlegrounds: Power in the Age of Artificial IntelligenceRating: 5 out of 5 stars5/5 (5)
- Scary Smart: The Future of Artificial Intelligence and How You Can Save Our WorldFrom EverandScary Smart: The Future of Artificial Intelligence and How You Can Save Our WorldRating: 4.5 out of 5 stars4.5/5 (55)
- ChatGPT Side Hustles 2024 - Unlock the Digital Goldmine and Get AI Working for You Fast with More Than 85 Side Hustle Ideas to Boost Passive Income, Create New Cash Flow, and Get Ahead of the CurveFrom EverandChatGPT Side Hustles 2024 - Unlock the Digital Goldmine and Get AI Working for You Fast with More Than 85 Side Hustle Ideas to Boost Passive Income, Create New Cash Flow, and Get Ahead of the CurveNo ratings yet
- Artificial Intelligence: A Guide for Thinking HumansFrom EverandArtificial Intelligence: A Guide for Thinking HumansRating: 4.5 out of 5 stars4.5/5 (30)
- System Design Interview: 300 Questions And Answers: Prepare And PassFrom EverandSystem Design Interview: 300 Questions And Answers: Prepare And PassNo ratings yet
- T-Minus AI: Humanity's Countdown to Artificial Intelligence and the New Pursuit of Global PowerFrom EverandT-Minus AI: Humanity's Countdown to Artificial Intelligence and the New Pursuit of Global PowerRating: 4 out of 5 stars4/5 (4)
- The AI Advantage: How to Put the Artificial Intelligence Revolution to WorkFrom EverandThe AI Advantage: How to Put the Artificial Intelligence Revolution to WorkRating: 4 out of 5 stars4/5 (7)
- Artificial Intelligence & Generative AI for Beginners: The Complete GuideFrom EverandArtificial Intelligence & Generative AI for Beginners: The Complete GuideRating: 5 out of 5 stars5/5 (1)
- 100M Offers Made Easy: Create Your Own Irresistible Offers by Turning ChatGPT into Alex HormoziFrom Everand100M Offers Made Easy: Create Your Own Irresistible Offers by Turning ChatGPT into Alex HormoziNo ratings yet
- Rise of Generative AI and ChatGPT: Understand how Generative AI and ChatGPT are transforming and reshaping the business world (English Edition)From EverandRise of Generative AI and ChatGPT: Understand how Generative AI and ChatGPT are transforming and reshaping the business world (English Edition)No ratings yet
- Hands-On System Design: Learn System Design, Scaling Applications, Software Development Design Patterns with Real Use-CasesFrom EverandHands-On System Design: Learn System Design, Scaling Applications, Software Development Design Patterns with Real Use-CasesNo ratings yet
- Artificial Intelligence: The Insights You Need from Harvard Business ReviewFrom EverandArtificial Intelligence: The Insights You Need from Harvard Business ReviewRating: 4.5 out of 5 stars4.5/5 (104)
- How to Make Money Online Using ChatGPT Prompts: Secrets Revealed for Unlocking Hidden Opportunities. Earn Full-Time Income Using ChatGPT with the Untold Potential of Conversational AI.From EverandHow to Make Money Online Using ChatGPT Prompts: Secrets Revealed for Unlocking Hidden Opportunities. Earn Full-Time Income Using ChatGPT with the Untold Potential of Conversational AI.No ratings yet
- AI and Machine Learning for Coders: A Programmer's Guide to Artificial IntelligenceFrom EverandAI and Machine Learning for Coders: A Programmer's Guide to Artificial IntelligenceRating: 4 out of 5 stars4/5 (2)
- The Digital Mind: How Science is Redefining HumanityFrom EverandThe Digital Mind: How Science is Redefining HumanityRating: 4.5 out of 5 stars4.5/5 (2)
- Our Final Invention: Artificial Intelligence and the End of the Human EraFrom EverandOur Final Invention: Artificial Intelligence and the End of the Human EraRating: 4 out of 5 stars4/5 (82)
- Make Money with ChatGPT: Your Guide to Making Passive Income Online with Ease using AI: AI Wealth MasteryFrom EverandMake Money with ChatGPT: Your Guide to Making Passive Income Online with Ease using AI: AI Wealth MasteryNo ratings yet
- The Roadmap to AI Mastery: A Guide to Building and Scaling ProjectsFrom EverandThe Roadmap to AI Mastery: A Guide to Building and Scaling ProjectsNo ratings yet