You might also like
- Innate and Adaptive Immune Responses Against CoronavirusDocument17 pagesInnate and Adaptive Immune Responses Against CoronavirusHARDITA SALSABILA FORTUNA HARDITA SALSABILA FORTUNANo ratings yet
- Therapeutic Approaches Against Coronaviruses Acute Respiratory SyndromeDocument21 pagesTherapeutic Approaches Against Coronaviruses Acute Respiratory Syndromenow youloseNo ratings yet
- Bioorganic Chemistry: MD Jawaid Akhtar TDocument9 pagesBioorganic Chemistry: MD Jawaid Akhtar TRetno Tri RahayuNo ratings yet
- Bioactive Natural Compounds Against Human Coronavirus - 2020 - Acta PharmaceuticDocument12 pagesBioactive Natural Compounds Against Human Coronavirus - 2020 - Acta PharmaceuticMohammed Shuaib AhmedNo ratings yet
- How Nanotechnology Can Help To Combat CovidDocument23 pagesHow Nanotechnology Can Help To Combat CovidKishore PaknikarNo ratings yet
- Advances and Challenges in The Prevention and Treatment of COVID-19Document8 pagesAdvances and Challenges in The Prevention and Treatment of COVID-19RoyNo ratings yet
- Safety and Biodistribution of NanoligomersTM Targeting SARS-CoV-2 Genome For Treatment of COVID-19Document28 pagesSafety and Biodistribution of NanoligomersTM Targeting SARS-CoV-2 Genome For Treatment of COVID-19Sandra GonzalezNo ratings yet
- Journal Pre-Proof: Trends in Plant ScienceDocument17 pagesJournal Pre-Proof: Trends in Plant ScienceMUGDHA MITTALNo ratings yet
- Control of Covid-19: Martin L. Nelwan, PHDDocument18 pagesControl of Covid-19: Martin L. Nelwan, PHDShikha GuptaNo ratings yet
- PIIS0168827820336758Document17 pagesPIIS0168827820336758Yusup AhmadiNo ratings yet
- Viruses: Non-Nucleotide Rna-Dependent Rna Polymerase Inhibitor That Blocks Sars-Cov-2 ReplicationDocument10 pagesViruses: Non-Nucleotide Rna-Dependent Rna Polymerase Inhibitor That Blocks Sars-Cov-2 Replicationwadelkrid1270No ratings yet
- Covid 19 PDFDocument25 pagesCovid 19 PDFRaihandi PutraNo ratings yet
- Remdesivir in Treating Coronavirus-A Review: IP International Journal of Periodontology and ImplantologyDocument4 pagesRemdesivir in Treating Coronavirus-A Review: IP International Journal of Periodontology and ImplantologySkAliHassanNo ratings yet
- Antivirus CovidDocument12 pagesAntivirus CovidAni RahayuNo ratings yet
- COVID-19 and Therapy With Essential Oils Having Antiviral, Anti-Inflammatory, and Immunomodulatory Properties PDFDocument13 pagesCOVID-19 and Therapy With Essential Oils Having Antiviral, Anti-Inflammatory, and Immunomodulatory Properties PDFNoNWONo ratings yet
- Clinical Trials On Drug Repositioning For COVID-19 TreatmentDocument7 pagesClinical Trials On Drug Repositioning For COVID-19 TreatmentArthur TravassosNo ratings yet
- Flavonoid Covid 19 - 2Document23 pagesFlavonoid Covid 19 - 2nadia firaNo ratings yet
- PRL CovidDocument8 pagesPRL Covidzainy zehraNo ratings yet
- Seminario CovidDocument17 pagesSeminario CovidGonzalo Ccahuana YanqueNo ratings yet
- Nutrients: The Antiviral, Anti-Inflammatory E Medicinal Herbs and Mushrooms and Sars-Cov-2 InfectionDocument13 pagesNutrients: The Antiviral, Anti-Inflammatory E Medicinal Herbs and Mushrooms and Sars-Cov-2 Infectionmmbire@gmail.comNo ratings yet
- BiomedPap - Bio 202003 0001Document9 pagesBiomedPap - Bio 202003 0001Edison Chiriboga OrtegaNo ratings yet
- Features, Evaluation and Treatment Coronavirus (COVID-19)Document19 pagesFeatures, Evaluation and Treatment Coronavirus (COVID-19)Prem Shankar GuptaNo ratings yet
- Biomedicine & Pharmacotherapy: Rory J. Malek, Colin A. Bill, Charlotte M. VinesDocument21 pagesBiomedicine & Pharmacotherapy: Rory J. Malek, Colin A. Bill, Charlotte M. Vineszahraa ahmedNo ratings yet
- Upwork 1Document118 pagesUpwork 1Yellow MellowNo ratings yet
- International Journal of Antimicrobial AgentsDocument9 pagesInternational Journal of Antimicrobial AgentsautomationenggNo ratings yet
- Presence of Mismatches Between Diagnostic PCR Assays and Coronavirus Sars-Cov-2 GenomeDocument17 pagesPresence of Mismatches Between Diagnostic PCR Assays and Coronavirus Sars-Cov-2 GenomeYulaimy BatistaNo ratings yet
- The Critical Role of Laboratory Medicine During Coronavirus Disease 2019 (COVID-19) and Other Viral OutbreaksDocument8 pagesThe Critical Role of Laboratory Medicine During Coronavirus Disease 2019 (COVID-19) and Other Viral OutbreaksEdgar José Acosta GarcíaNo ratings yet
- Asselah 2020Document42 pagesAsselah 2020ENRICO 102011216No ratings yet
- Antiviral Efficacy of Medicinal Plants Against Respiratory Viruses: Respiratory Syncytial Virus (RSV) and Coronavirus (Cov) / Covid 19Document10 pagesAntiviral Efficacy of Medicinal Plants Against Respiratory Viruses: Respiratory Syncytial Virus (RSV) and Coronavirus (Cov) / Covid 19Sonja GadzovskaNo ratings yet
- 1 s2.0 S222541102030506X MainDocument8 pages1 s2.0 S222541102030506X Mainuniqlu9No ratings yet
- Antibiotics: Molnupiravir-A Novel Oral Anti-Sars-Cov-2 AgentDocument8 pagesAntibiotics: Molnupiravir-A Novel Oral Anti-Sars-Cov-2 AgentXuân BìnhNo ratings yet
- (Drug Development Research) Phadke, Mrudula - Saunik, Sujata - COVID-19 Treatment by Repurposing Drugs Until The Vaccine Is in Sight (2020)Document3 pages(Drug Development Research) Phadke, Mrudula - Saunik, Sujata - COVID-19 Treatment by Repurposing Drugs Until The Vaccine Is in Sight (2020)Francisco UrdanetANo ratings yet
- COVID19-innate ImmunityDocument16 pagesCOVID19-innate Immunityملكة زمانيNo ratings yet
- Repurposing Therapeutics For COVID-19: Rapid Prediction of Commercially Available Drugs Through Machine Learning and DockingDocument13 pagesRepurposing Therapeutics For COVID-19: Rapid Prediction of Commercially Available Drugs Through Machine Learning and Dockingpihu1No ratings yet
- Biomedicine & Pharmacotherapy: ReviewDocument18 pagesBiomedicine & Pharmacotherapy: ReviewRahmanda LintangNo ratings yet
- Excellent Paper On Covid 19Document20 pagesExcellent Paper On Covid 19GalenNo ratings yet
- Golchin2020 Article MesenchymalStemCellTherapyForCDocument7 pagesGolchin2020 Article MesenchymalStemCellTherapyForCJuan Pablo Rodríguez CoronaNo ratings yet
- DownloadfileDocument9 pagesDownloadfileSpamerNo ratings yet
- SARS-CoV-2 X ERDocument6 pagesSARS-CoV-2 X ERJulia MouraNo ratings yet
- Viable SARS-CoV-2 in The Air of A Hospital Room With COVID-19 Patients - J A Lednicky Et Al - 2020Document20 pagesViable SARS-CoV-2 in The Air of A Hospital Room With COVID-19 Patients - J A Lednicky Et Al - 2020Guto ClipesNo ratings yet
- COVID-19 20-April-2021Document28 pagesCOVID-19 20-April-2021jongsu kimNo ratings yet
- COVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsFrom EverandCOVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsNo ratings yet
- Serologic Responses To Sars-Cov-2 Infection Among Hospital Staff With Mild Disease in Eastern FranceDocument21 pagesSerologic Responses To Sars-Cov-2 Infection Among Hospital Staff With Mild Disease in Eastern FranceAssia AouachriaNo ratings yet
- Omeprazole in Covid 19 Germany StudyDocument28 pagesOmeprazole in Covid 19 Germany StudyTanushree PanjariNo ratings yet
- Antivirals For COVID-19 A Critical ReviewDocument10 pagesAntivirals For COVID-19 A Critical ReviewOskr VeraNo ratings yet
- IndianJMedRes000-3026339 082423Document6 pagesIndianJMedRes000-3026339 082423tummmereNo ratings yet
- WholeDocument3 pagesWholePQ TODANo ratings yet
- Insights of Severe Acute Respiratory Syndrome Coronavirus (Sars-Cov-2) Pandemic: A Current ReviewDocument22 pagesInsights of Severe Acute Respiratory Syndrome Coronavirus (Sars-Cov-2) Pandemic: A Current ReviewkentchickenNo ratings yet
- International Journal of Antimicrobial AgentsDocument3 pagesInternational Journal of Antimicrobial AgentsmiNo ratings yet
- The Critical Role of Laboratory Medicine During Coronavirus Disease 2019 (COVID-19) and Other Viral OutbreaksDocument8 pagesThe Critical Role of Laboratory Medicine During Coronavirus Disease 2019 (COVID-19) and Other Viral OutbreaksIsrael Parra-OrtegaNo ratings yet
- The Critical Role of Laboratory Medicine During Coronavirus Disease 2019 (COVID-19) and Other Viral OutbreaksDocument8 pagesThe Critical Role of Laboratory Medicine During Coronavirus Disease 2019 (COVID-19) and Other Viral OutbreaksIsrael Parra-OrtegaNo ratings yet
- Antivirals Against Coronaviruses: Candidate Drugs For Sars-Cov-2 Treatment?Document23 pagesAntivirals Against Coronaviruses: Candidate Drugs For Sars-Cov-2 Treatment?zizaviquisaNo ratings yet
- Breve Reseña Sobre Medicamentos y Vacunas Reutilizados para El Posible Tratamiento de COVID-19Document15 pagesBreve Reseña Sobre Medicamentos y Vacunas Reutilizados para El Posible Tratamiento de COVID-19Cristal Jewels DiamondNo ratings yet
- 4 Vol. 12 Issue 7 July 2021 IJPSR RE 4418Document7 pages4 Vol. 12 Issue 7 July 2021 IJPSR RE 4418VinayNo ratings yet
- Cellular and Molecular ImmunologyDocument21 pagesCellular and Molecular ImmunologyMUGDHA MITTALNo ratings yet
- COVID 19 An Emerging Coronavirus Infection Advances and Prospects in Designing and Developing Vaccines Immunotherapeutics and TherapeuticsDocument8 pagesCOVID 19 An Emerging Coronavirus Infection Advances and Prospects in Designing and Developing Vaccines Immunotherapeutics and TherapeuticsCertaf MaghnjaNo ratings yet
- A Comprehensive Summary of The Knowledge On COVID-19 TreatmentDocument37 pagesA Comprehensive Summary of The Knowledge On COVID-19 TreatmentChawki MokademNo ratings yet
- Andrade Et Al-2020-Journal of Health & Biological SciencesDocument9 pagesAndrade Et Al-2020-Journal of Health & Biological SciencesJuliaNo ratings yet
- Gil Loescher - Beyond Charity - International Cooperation and The Global Refugee Crisis A Twentieth Century Fund Book (1996)Document273 pagesGil Loescher - Beyond Charity - International Cooperation and The Global Refugee Crisis A Twentieth Century Fund Book (1996)Maressa OmenaNo ratings yet
- Jane Freedman (Auth.) - Gendering The International Asylum and Refugee Debate (2015, Palgrave Macmillan UK)Document249 pagesJane Freedman (Auth.) - Gendering The International Asylum and Refugee Debate (2015, Palgrave Macmillan UK)Maressa OmenaNo ratings yet
- Jane Freedman - Gendering The International Asylum and Refugee Debate (2007)Document225 pagesJane Freedman - Gendering The International Asylum and Refugee Debate (2007)Maressa OmenaNo ratings yet
- 1966 Bull - The Case For A Classical ApproachDocument18 pages1966 Bull - The Case For A Classical ApproachMaressa OmenaNo ratings yet
- Cambridge International AS & A Level: Biology 9700/12Document16 pagesCambridge International AS & A Level: Biology 9700/12shabanaNo ratings yet
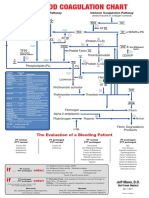
- Blood Clotting ChartDocument1 pageBlood Clotting ChartBianca SimionescuNo ratings yet
- Immune Dysfunction and Risk of Infection in CKD - 2019Document8 pagesImmune Dysfunction and Risk of Infection in CKD - 2019Lú VillalobosNo ratings yet
- Microbiology Notes: Bacteriology BacteriaDocument35 pagesMicrobiology Notes: Bacteriology BacteriaAngelo Jude CobachaNo ratings yet
- TGA Letter of Demand - 4 July 2023Document30 pagesTGA Letter of Demand - 4 July 2023Tim BrownNo ratings yet
- Upper Urinary Tract. InfectionDocument11 pagesUpper Urinary Tract. InfectionnadhifNo ratings yet
- Polydactyly PamphletDocument2 pagesPolydactyly PamphletAlan100% (1)
- Microbiology: PROKARYOTIC & EUKARYOTIC CELLSDocument10 pagesMicrobiology: PROKARYOTIC & EUKARYOTIC CELLSEmily RaeNo ratings yet
- Gingival Epithelium: Aathira VijayakumarDocument137 pagesGingival Epithelium: Aathira VijayakumarAathira MenonNo ratings yet
- Hemolytic Disease of The NewbornDocument1 pageHemolytic Disease of The NewbornMASIINo ratings yet
- As 4259-1995 Ancillary Devices For Expired Air ResuscitationDocument9 pagesAs 4259-1995 Ancillary Devices For Expired Air ResuscitationSAI Global - APACNo ratings yet
- Terminology of Unani NameDocument5 pagesTerminology of Unani NameWalid Hasan Towkir Ahammed sarkar100% (1)
- Pharagraph of Covid 19Document2 pagesPharagraph of Covid 19Bill RenzoNo ratings yet
- 2021 Antagonistic Activity of Lactic Acid Bacteria Against Phytopathogenic Fungi Isolated From Cherry TomatoDocument10 pages2021 Antagonistic Activity of Lactic Acid Bacteria Against Phytopathogenic Fungi Isolated From Cherry TomatoEduardo Urbano Moraga CáceresNo ratings yet
- Successful Treatment of Multiple Common Warts With Intralesional OzoneDocument6 pagesSuccessful Treatment of Multiple Common Warts With Intralesional OzoneRubensNo ratings yet
- Virus, Viroids and PrionsDocument29 pagesVirus, Viroids and PrionscatherinejoaquinNo ratings yet
- Gram Negative Aerobic and Facultative RodsDocument53 pagesGram Negative Aerobic and Facultative RodsChatie PipitNo ratings yet
- Hazard Identification - B-Sweet PotatoDocument2 pagesHazard Identification - B-Sweet PotatoFloreidNo ratings yet
- Bio1 11 - 12 Q1 0204 FDDocument22 pagesBio1 11 - 12 Q1 0204 FDJoe Marc Lamosao CaninNo ratings yet
- Eukaryotic Cell CultureDocument6 pagesEukaryotic Cell Culturesushaantb400No ratings yet
- Enterocolitis NecrosanteDocument21 pagesEnterocolitis NecrosantedenisNo ratings yet
- BIO Final22 QuestionssolDocument16 pagesBIO Final22 Questionssolmohamed.osama28599No ratings yet
- 7th Grade Pretest and KeyDocument8 pages7th Grade Pretest and Keyapi-377802356No ratings yet
- Endotoxin Limit PDFDocument1 pageEndotoxin Limit PDFkamran khanNo ratings yet
- Evolving Treatment Approaches For MGDocument59 pagesEvolving Treatment Approaches For MGSnezana MihajlovicNo ratings yet
- Paper 2 November 2001Document5 pagesPaper 2 November 2001MSHNo ratings yet
- MICR3213 - Microbial Ecology - 2018 PDFDocument44 pagesMICR3213 - Microbial Ecology - 2018 PDFCalesia FearonNo ratings yet
- EtestDocument6 pagesEtestFatima VessaliusNo ratings yet
- What Is Rheumatoid ArthritisDocument16 pagesWhat Is Rheumatoid ArthritisDurge Raj GhalanNo ratings yet
- Reviews: Fracture Healing: Mechanisms and InterventionsDocument10 pagesReviews: Fracture Healing: Mechanisms and InterventionsFatrika DewiNo ratings yet