You might also like
- M.H. Sloboda - 1961 - Design and Strength of Brazed JointsDocument16 pagesM.H. Sloboda - 1961 - Design and Strength of Brazed JointsPieter van der MeerNo ratings yet
- Testing of TransformerDocument130 pagesTesting of TransformerRohit DuttaNo ratings yet
- FreeNAS 11.2Document370 pagesFreeNAS 11.2phong nguyen huuNo ratings yet
- Final Bridge Design Report (Berhampur AniDocument98 pagesFinal Bridge Design Report (Berhampur AniYogesh Indolia100% (6)
- Gantt Chart L2Document7 pagesGantt Chart L2AF OfficialNo ratings yet
- Unleash Your Speed: Thinking Forward. Challenging LimitsDocument3 pagesUnleash Your Speed: Thinking Forward. Challenging Limitsanon_19722876No ratings yet
- FF68 Manual Check DepositDocument10 pagesFF68 Manual Check DepositvittoriojayNo ratings yet
- Umbilical Cord Milking in Term Infants Delivered by Cesarean Section: A Randomized Controlled TrialDocument5 pagesUmbilical Cord Milking in Term Infants Delivered by Cesarean Section: A Randomized Controlled TrialAffah MustafaNo ratings yet
- Cit230 PDFDocument4 pagesCit230 PDFJoyBoyXNo ratings yet
- Clinical Case Study: Listeria Moncytogenes Cross-ContaminationDocument3 pagesClinical Case Study: Listeria Moncytogenes Cross-ContaminationjaljimNo ratings yet
- Penundaan Pemotongan TalipusatDocument14 pagesPenundaan Pemotongan Talipusatmaya maeNo ratings yet
- Thompson Et al-1998-BJOG An International Journal of Obstetrics & GynaecologyDocument5 pagesThompson Et al-1998-BJOG An International Journal of Obstetrics & GynaecologyCostin VrabieNo ratings yet
- CORD Albumin JAUNDICEDocument3 pagesCORD Albumin JAUNDICESuman MondalNo ratings yet
- Saco Pollitt1981Document9 pagesSaco Pollitt1981Víctor FuentesNo ratings yet
- The Prevalence of Gastroesophageal Reflux in Children With Tracheomalacia and LaryngomalaciaDocument5 pagesThe Prevalence of Gastroesophageal Reflux in Children With Tracheomalacia and LaryngomalaciakinghutanNo ratings yet
- Ictericia Por Seno MaternoDocument8 pagesIctericia Por Seno MaternoJose Antonio Labrada GonzalezNo ratings yet
- International JournalDocument4 pagesInternational JournalAbinaya RadhakrishnanNo ratings yet
- Febrile Urinary Tract Infections in 0-To 3-Month-Old Infants: A Prospective Follow-Up StudyDocument4 pagesFebrile Urinary Tract Infections in 0-To 3-Month-Old Infants: A Prospective Follow-Up StudyMark Vertiz CernaNo ratings yet
- Estudio de MariDocument6 pagesEstudio de MarianjidisNo ratings yet
- 1 s2.0 S0002937899707039 MainDocument5 pages1 s2.0 S0002937899707039 MainPutri AgriNo ratings yet
- Chorioamnionitis and Prognosis For Term Infants-13Document5 pagesChorioamnionitis and Prognosis For Term Infants-13ronny29No ratings yet
- DiareDocument10 pagesDiareNanda Putri SeptianaNo ratings yet
- Peds 2023-061931Document8 pagesPeds 2023-061931Rene H. Framcisco, MDNo ratings yet
- Is Breastfeeding Really Favoring Early Neonatal Jaundice?: Pediatrics April 2001Document8 pagesIs Breastfeeding Really Favoring Early Neonatal Jaundice?: Pediatrics April 2001Jeklee MancapNo ratings yet
- Umbilical Cord Milking PDFDocument5 pagesUmbilical Cord Milking PDFMax RodriguezNo ratings yet
- Diarrhea, Dehydration, and The Associated Mortality in Children With Complicated Severe Acute Malnutrition: A Prospective Cohort Study in UgandaDocument11 pagesDiarrhea, Dehydration, and The Associated Mortality in Children With Complicated Severe Acute Malnutrition: A Prospective Cohort Study in Ugandasalma romnalia ashshofaNo ratings yet
- Fetal Inflamatory Response SyndromeDocument9 pagesFetal Inflamatory Response SyndromeAnonymous mvNUtwidNo ratings yet
- Faecal Calprotectin (FC) in Babies Born To Oher With or Without IBDocument2 pagesFaecal Calprotectin (FC) in Babies Born To Oher With or Without IBMartinaNo ratings yet
- 991 FullDocument5 pages991 FullBelleNo ratings yet
- Hypothermia in Very Low Birth Weight InfantsDocument9 pagesHypothermia in Very Low Birth Weight InfantsGiovanni MictilNo ratings yet
- Ukuran Hepar Lien Pada AnakDocument6 pagesUkuran Hepar Lien Pada Anakivan ekoNo ratings yet
- 1642 Full PDFDocument5 pages1642 Full PDFAriana FlemingNo ratings yet
- Umbilical Artery Pulsatility Index and Fetal AbdominalDocument5 pagesUmbilical Artery Pulsatility Index and Fetal AbdominalerasmohuertasNo ratings yet
- Person's Correlation Coeffkient (I) WithDocument1 pagePerson's Correlation Coeffkient (I) WithMika OikuNo ratings yet
- Sepsisin ObstetricsDocument9 pagesSepsisin ObstetricsrakulsundaramNo ratings yet
- Mi2018 2845352 PDFDocument5 pagesMi2018 2845352 PDFDewi LarasatiNo ratings yet
- Mir Ghani 2006Document4 pagesMir Ghani 2006Sarly FebrianaNo ratings yet
- Bio MarkerDocument4 pagesBio MarkerShrimanta RamchiaryNo ratings yet
- Hyperbilirubinemia, Phototherapy, and Childhood Asthma: ObjectivesDocument11 pagesHyperbilirubinemia, Phototherapy, and Childhood Asthma: ObjectivesrizaniaNo ratings yet
- Hiperbilirrubinemia Neonatal ExtremaDocument3 pagesHiperbilirrubinemia Neonatal ExtremaKateNo ratings yet
- Ma 70 408Document5 pagesMa 70 408Zahra AfifahNo ratings yet
- Lactobacillus Acidophilus and Bifidobacterium Bifidum Atored at Ambient Temperature Are Effective in The Treatment of Acute DiarrhoeaDocument7 pagesLactobacillus Acidophilus and Bifidobacterium Bifidum Atored at Ambient Temperature Are Effective in The Treatment of Acute DiarrhoeaEvelynRuizNo ratings yet
- Pi Is 0015028207022418Document1 pagePi Is 0015028207022418Hayati Rizki PutriNo ratings yet
- Reduction of Severe Hyperbilirubinemia After Institution of Predischarge Bilirubin ScreeningDocument6 pagesReduction of Severe Hyperbilirubinemia After Institution of Predischarge Bilirubin ScreeningImran A. IsaacNo ratings yet
- Acta Paediatrica - 2014 - Velasco - Using A Urine Dipstick To Identify A Positive Urine Culture in Young Febrile Infants IsDocument6 pagesActa Paediatrica - 2014 - Velasco - Using A Urine Dipstick To Identify A Positive Urine Culture in Young Febrile Infants IsCris FischerNo ratings yet
- Leong Et Al-2004-BJOG: An International Journal of Obstetrics & GynaecologyDocument2 pagesLeong Et Al-2004-BJOG: An International Journal of Obstetrics & GynaecologyAngie MandeoyaNo ratings yet
- Diagnosis of Colorectal Polyps by Hydrocolonic Sonography in Children With Rectal BleedingDocument6 pagesDiagnosis of Colorectal Polyps by Hydrocolonic Sonography in Children With Rectal BleedingСергей СадовниковNo ratings yet
- Bhutan IDocument9 pagesBhutan IEderSoaresdeAlencarNo ratings yet
- Cervical FunnelingDocument3 pagesCervical FunnelingRatnakar KamathNo ratings yet
- Ivf PDFDocument2 pagesIvf PDFarjunNo ratings yet
- Hyperglycemia and Morbidity and Mortality in Extremely Low Birth Weight InfantsDocument7 pagesHyperglycemia and Morbidity and Mortality in Extremely Low Birth Weight InfantsIvan VeriswanNo ratings yet
- Fetal Biometei PDFDocument134 pagesFetal Biometei PDFfariska amanizataNo ratings yet
- C Reactive Protein in The Evaluation of Febrile IllnessDocument6 pagesC Reactive Protein in The Evaluation of Febrile IllnessSarang BondeNo ratings yet
- Kaplan1998 PDFDocument6 pagesKaplan1998 PDFAmsir LimbongNo ratings yet
- Are Women With Recurrent Spontaneous Preterm Births Different From Those Without Such HistoryDocument9 pagesAre Women With Recurrent Spontaneous Preterm Births Different From Those Without Such HistoryMichael HusainNo ratings yet
- Nihms825906 PDFDocument14 pagesNihms825906 PDFRhani TuananyNo ratings yet
- Doppler and Biophysical Assessment in Growth Restricted Fetuses: Distribution of Test ResultsDocument7 pagesDoppler and Biophysical Assessment in Growth Restricted Fetuses: Distribution of Test ResultslalimdNo ratings yet
- Neonatal Hypoglycaemia Mothers Given Sulphonylurea Drugs PregnancyDocument6 pagesNeonatal Hypoglycaemia Mothers Given Sulphonylurea Drugs PregnancyGideon NicoNo ratings yet
- The Efficacy of Quantitative Fetal Fibronectin in Predicting Spontaneous Preterm Birth in Symptomatic Women: A Retrospective Cohort StudyDocument6 pagesThe Efficacy of Quantitative Fetal Fibronectin in Predicting Spontaneous Preterm Birth in Symptomatic Women: A Retrospective Cohort StudyGeztaNasafirHermawanNo ratings yet
- Large-Volume Paracentesis in The Management of Ascites in ChildrenDocument5 pagesLarge-Volume Paracentesis in The Management of Ascites in ChildrenMed MorciNo ratings yet
- Dengue Infection and PlacentaDocument4 pagesDengue Infection and PlacentaGabriella ArgyNo ratings yet
- Can Fundal Height Predict Weight or Twins?: SommaireDocument4 pagesCan Fundal Height Predict Weight or Twins?: SommairePandawa ObgynNo ratings yet
- Delayed Uterine Fluid Clearance and Reduced Uterine Perfusion inDocument7 pagesDelayed Uterine Fluid Clearance and Reduced Uterine Perfusion inCarolinaNo ratings yet
- Fetal Anesthetic Requirement (MAC) For HalothaneDocument6 pagesFetal Anesthetic Requirement (MAC) For HalothaneSonia RogersNo ratings yet
- Factors Affecting Bilirubin Levels During First 48 Hours of Life in Healthy InfantsDocument10 pagesFactors Affecting Bilirubin Levels During First 48 Hours of Life in Healthy InfantsZed P. EstalillaNo ratings yet
- Congenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementFrom EverandCongenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementDiva D. De León-CrutchlowNo ratings yet
- Hilti, Inc. 5400 South 122 East Avenue Tulsa, OK 74146 1-800-879-8000Document10 pagesHilti, Inc. 5400 South 122 East Avenue Tulsa, OK 74146 1-800-879-8000Daniel PulgarNo ratings yet
- Brksec 3021Document131 pagesBrksec 3021alfagemeoNo ratings yet
- Fake ReviewDocument6 pagesFake ReviewHarshal PimpalshendeNo ratings yet
- Face Detection and Recognition TechnologyDocument17 pagesFace Detection and Recognition TechnologyDinesh KumarNo ratings yet
- Sist-En-13001-2-2014 NFDocument15 pagesSist-En-13001-2-2014 NF정주호No ratings yet
- Ertl MGT 4010 Final Exam APPLICATION Semester 2 2019Document6 pagesErtl MGT 4010 Final Exam APPLICATION Semester 2 2019Raihah Nabilah HashimNo ratings yet
- Computer Literacy - Lesson 1 - Computer SystemsDocument1 pageComputer Literacy - Lesson 1 - Computer SystemscuddlesttNo ratings yet
- Fast and Reliable: Handheld TympanometerDocument4 pagesFast and Reliable: Handheld TympanometerKothapalli ChiranjeeviNo ratings yet
- Math 115 Uiuc Written Homework 6 SolutionsDocument4 pagesMath 115 Uiuc Written Homework 6 Solutionsafmspqvdy100% (1)
- Block Ciphers and The Data Encryption Standard Presented byDocument34 pagesBlock Ciphers and The Data Encryption Standard Presented bySabin BhandariNo ratings yet
- Sinumerik 802dDocument212 pagesSinumerik 802dThanh BuiNo ratings yet
- 05 iPASO LCT Training Manual (Ethernnet) Dec2012-2Document105 pages05 iPASO LCT Training Manual (Ethernnet) Dec2012-2Wubie NegaNo ratings yet
- Shivani Mehan - ResumeDocument1 pageShivani Mehan - ResumeShivani MehanNo ratings yet
- Steering Gear PrincipalDocument21 pagesSteering Gear PrincipaljanuarNo ratings yet
- Tems Cellplanner: Driving Network ExcellenceDocument8 pagesTems Cellplanner: Driving Network ExcellenceTarasNo ratings yet
- BoT-IoT - GenerationDocument40 pagesBoT-IoT - GenerationHassina KouachiNo ratings yet
- AsasDocument180 pagesAsasAres SagaNo ratings yet
- Prime NumbersDocument2 pagesPrime NumbersDarkas2100% (1)
- Ada 5 Condensadores PDFDocument2 pagesAda 5 Condensadores PDFTony Maldonado PinzonNo ratings yet
- Modification Sheet Yaesu FT-847: So This and All of My Modification Sheet Are For Education Purposes Only !Document28 pagesModification Sheet Yaesu FT-847: So This and All of My Modification Sheet Are For Education Purposes Only !Yudi WisenoNo ratings yet
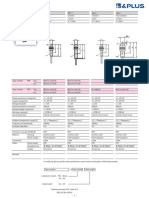
- B&Plus Proximity Sensor - 001.BES07e - Usm8-1Document1 pageB&Plus Proximity Sensor - 001.BES07e - Usm8-1Hussein RamzaNo ratings yet
- SOT Tool - Required UpdatesDocument3 pagesSOT Tool - Required UpdatesJuzar CMNo ratings yet
- BDSP Lecture 3Document79 pagesBDSP Lecture 3Mohammed FarisNo ratings yet