You might also like
- S-Malunion - Principals and ManagementDocument45 pagesS-Malunion - Principals and ManagementshahnazroeentanmailNo ratings yet
- Presentation 1Document16 pagesPresentation 1Moiz AliNo ratings yet
- FR Distal HumerusDocument55 pagesFR Distal Humerusiisscribd100% (1)
- Management Tibial Plateau FractureDocument45 pagesManagement Tibial Plateau FracturePurushothama Rao NalamatiNo ratings yet
- U05-Distal Humerus FracturesDocument84 pagesU05-Distal Humerus FracturesAmina BentratNo ratings yet
- S-Distal Radius Malunion, CorrectionDocument28 pagesS-Distal Radius Malunion, CorrectionshahnazroeentanmailNo ratings yet
- Proximal Femoral NewDocument34 pagesProximal Femoral NewHimanshu HemantNo ratings yet
- Fractures of The Humeral Shaft: Gregory L. Desilva, MDDocument35 pagesFractures of The Humeral Shaft: Gregory L. Desilva, MDJulio Quiroz GuevaraNo ratings yet
- Trochanteric #Document20 pagesTrochanteric #Prakash AyyaduraiNo ratings yet
- Pelvic Ring Injuries: Definitive Management: James C. Krieg, MDDocument64 pagesPelvic Ring Injuries: Definitive Management: James C. Krieg, MDGabriel KlemensNo ratings yet
- Surgical Treatment For Temporomandibular Joint Disorders ObjectivesDocument29 pagesSurgical Treatment For Temporomandibular Joint Disorders Objectivessergiusz9No ratings yet
- The Principles of Intra-Articular Fracture Care: Joseph Schatzker M.D., B.SC., (Med.), F.R.C.S. (C)Document31 pagesThe Principles of Intra-Articular Fracture Care: Joseph Schatzker M.D., B.SC., (Med.), F.R.C.S. (C)baoNo ratings yet
- Distal Femur Fractures: Brett D. Crist, MDDocument88 pagesDistal Femur Fractures: Brett D. Crist, MDaddison woodNo ratings yet
- Discuss Tension Band Principles: by DR Kabiru SALISU 11 Aug. 2017Document40 pagesDiscuss Tension Band Principles: by DR Kabiru SALISU 11 Aug. 2017Azmi FarhadiNo ratings yet
- Articular Fractures: PrinciplesDocument24 pagesArticular Fractures: Principlestom kurniawanNo ratings yet
- Lower Limb Trauma: Cast Application For Common FracturesDocument58 pagesLower Limb Trauma: Cast Application For Common FracturesdrusmanjamilhcmdNo ratings yet
- FX of Distal HumerusDocument76 pagesFX of Distal HumerusGrace NazarenoNo ratings yet
- Correction of Hallux Valgus With OsteotomiesDocument30 pagesCorrection of Hallux Valgus With OsteotomiesMuhammad MoralNo ratings yet
- Total Knee ReplacementDocument49 pagesTotal Knee Replacementefancoolhand09No ratings yet
- My Experience in Paediatric Orthopaedics at Sanchetti Institute For Orthopaedics and RehabilitationDocument48 pagesMy Experience in Paediatric Orthopaedics at Sanchetti Institute For Orthopaedics and RehabilitationMd Ahsanuzzaman PinkuNo ratings yet
- Tibial Plateau Fractures: Yasser AlwabliDocument35 pagesTibial Plateau Fractures: Yasser AlwabliPin Han NaNo ratings yet
- Biomechanical Comparison of Dynamic Hip Screw, ProximalDocument24 pagesBiomechanical Comparison of Dynamic Hip Screw, ProximalPriscilla PriscillaNo ratings yet
- Malleolar Fractures 17Document41 pagesMalleolar Fractures 17ABUBAKER ZANBOUZINo ratings yet
- Distal Radius Osteotomy ComDocument37 pagesDistal Radius Osteotomy ComIskolar MorenoNo ratings yet
- Dasar-Dasar Radiologi Musculoskeletal PDFDocument101 pagesDasar-Dasar Radiologi Musculoskeletal PDFIndra MahaputraNo ratings yet
- Ankle Fractures - A Logical Approach To Their FixationDocument48 pagesAnkle Fractures - A Logical Approach To Their FixationRoman MosneagaNo ratings yet
- The Hip: Therapeutic Exercise 2 Lino Linford BangayanDocument91 pagesThe Hip: Therapeutic Exercise 2 Lino Linford BangayanLino Linford Yu Bangayan100% (1)
- Forearm Fractures: Derek J. Donegan, M.D. University of PennsylvaniaDocument55 pagesForearm Fractures: Derek J. Donegan, M.D. University of PennsylvaniaSherly DesnitaNo ratings yet
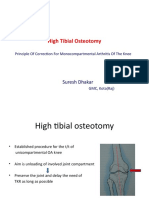
- High Tibial Osteotomy: Suresh DhakarDocument40 pagesHigh Tibial Osteotomy: Suresh DhakarAtul PandeyNo ratings yet
- Tibial Shaft Fracture: - Due To Subcutaneous LocationDocument19 pagesTibial Shaft Fracture: - Due To Subcutaneous LocationNuhu BankwhotNo ratings yet
- Total Knee Arthroplasty PrinciplesDocument40 pagesTotal Knee Arthroplasty PrinciplesMitri NassarNo ratings yet
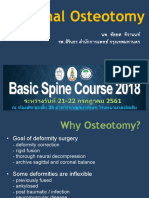
- Spinal Osteotomy 2018Document43 pagesSpinal Osteotomy 2018YoNo ratings yet
- Surgery For TMD - TJRDocument78 pagesSurgery For TMD - TJRJinz nazarNo ratings yet
- Mandible FracturesDocument60 pagesMandible FracturesMellow MenaisNo ratings yet
- Management of Fracture Acetabulum in Geriatric Age Group Saturday 12 15Document44 pagesManagement of Fracture Acetabulum in Geriatric Age Group Saturday 12 15tarikeopsNo ratings yet
- Bedah 2 - BimbelmantapDocument208 pagesBedah 2 - BimbelmantapDELLA DWINo ratings yet
- (Peserta) Bedah 2 - Mantap Februari 2017Document211 pages(Peserta) Bedah 2 - Mantap Februari 2017karno0% (1)
- Lecture 7 Femoral Diapisis and Distal FDocument16 pagesLecture 7 Femoral Diapisis and Distal FQueen SofiaNo ratings yet
- Osteotomies Jarthrodesis JDocument41 pagesOsteotomies Jarthrodesis Jdesire kbpNo ratings yet
- Distal Humeral Fractures - Basic Management Concepts: Dr. Jeffrey Kwee, PGY3 August 22, 2006Document27 pagesDistal Humeral Fractures - Basic Management Concepts: Dr. Jeffrey Kwee, PGY3 August 22, 2006sukhee_baatarNo ratings yet
- U04 Fxs of Humeral ShaftDocument88 pagesU04 Fxs of Humeral Shaftadrian_mogosNo ratings yet
- (Trauma) 18 September Lower Extremity AmputationDocument37 pages(Trauma) 18 September Lower Extremity Amputationpublic newbieNo ratings yet
- m4 Lecture 1 Ortho IntroDocument72 pagesm4 Lecture 1 Ortho IntroAqeel RehmanNo ratings yet
- Fracture ManagementDocument50 pagesFracture ManagementCharLes OdalNo ratings yet
- Revision Total Knee Arthroplasty: Principles of Management: Israel Orthopaedic Association December, 2012Document35 pagesRevision Total Knee Arthroplasty: Principles of Management: Israel Orthopaedic Association December, 2012TEJA B.M.K.PNo ratings yet
- Principles of External FixationDocument36 pagesPrinciples of External Fixationcromwellopoku42No ratings yet
- Fractures HFHDocument74 pagesFractures HFHEmmanuel Papa AcquahNo ratings yet
- Journal Reading: Nonunion of Fracture ClavicleDocument14 pagesJournal Reading: Nonunion of Fracture ClavicleKhafid Asy' AriNo ratings yet
- 18 Mandibular Fractures 2016-Presented LectureDocument34 pages18 Mandibular Fractures 2016-Presented LectureHanin AbukhiaraNo ratings yet
- Preprosthetic Surgery AGDLas Vegas 2017 FinalDocument133 pagesPreprosthetic Surgery AGDLas Vegas 2017 FinalArtanNo ratings yet
- Femoral Neck FractureDocument36 pagesFemoral Neck FractureAnonymous ekem7I100% (2)
- Mandible FX Slides 040526Document62 pagesMandible FX Slides 040526azharNo ratings yet
- Extremity Trauma Board Review 2018Document80 pagesExtremity Trauma Board Review 2018rigo montejoNo ratings yet
- Patellar FractureDocument43 pagesPatellar FractureAkash KoulNo ratings yet
- Inverted L OsteotomyDocument9 pagesInverted L OsteotomyhaneefmdfNo ratings yet
- Terrible Triad - ElbowDocument96 pagesTerrible Triad - ElbowWasim R. IssaNo ratings yet
- Distal Radius and UlnaDocument40 pagesDistal Radius and UlnaDia CembranoNo ratings yet
- Reduction, Relocation and Splinting in Emergency Room (RASER)From EverandReduction, Relocation and Splinting in Emergency Room (RASER)No ratings yet
- Tips and Tricks for Problem Fractures, Volume I: The Upper ExtremityFrom EverandTips and Tricks for Problem Fractures, Volume I: The Upper ExtremityDaniel S. HorwitzNo ratings yet
- Lab Ventilation SystemsDocument10 pagesLab Ventilation SystemsHyeong-Ho KimNo ratings yet
- Elite One PagerDocument1 pageElite One PagernikzakuNo ratings yet
- System 4 Med G 7831 - PG 85362Document76 pagesSystem 4 Med G 7831 - PG 85362jerimiah_manzonNo ratings yet
- Air Cargo (Assignment 1)Document5 pagesAir Cargo (Assignment 1)Sara khanNo ratings yet
- Buffer PH 10Document7 pagesBuffer PH 10saiful2016No ratings yet
- Reading Passage 2: HomeopathyDocument4 pagesReading Passage 2: HomeopathyNguyễn TịnhNo ratings yet
- Short EssayDocument2 pagesShort EssayMary Jane RiparipNo ratings yet
- Anil Ghom - Textbook of Oral Radiology - 2nd Ed - WWW - Thedentalhub.org - inDocument928 pagesAnil Ghom - Textbook of Oral Radiology - 2nd Ed - WWW - Thedentalhub.org - inSatavisha MohapatraNo ratings yet
- Chapter 08 - Ion Exchange, Water Demineralization & Resin TestingDocument23 pagesChapter 08 - Ion Exchange, Water Demineralization & Resin TestingMohamed ElbehlilNo ratings yet
- 1251-1260 MCQ in Facial Plastic and Reconstructive SurgeryDocument8 pages1251-1260 MCQ in Facial Plastic and Reconstructive SurgerySajag GuptaNo ratings yet
- Reliance NetmedsDocument4 pagesReliance NetmedsSiddhi ShindeNo ratings yet
- Manufacturing Process of Plastic BottlesDocument19 pagesManufacturing Process of Plastic BottlesAparna Samuel87% (23)
- Slope Stability Analysis of Unsaturated Soil - IMPORTANTE PDFDocument18 pagesSlope Stability Analysis of Unsaturated Soil - IMPORTANTE PDFAngela GonzálezNo ratings yet
- BancassuranceDocument53 pagesBancassuranceSonali Chaubey0% (1)
- Seko Tekna Evo TPG DatasheetDocument4 pagesSeko Tekna Evo TPG Datasheetনিস্তব্ধতার প্রহরেNo ratings yet
- Simply Put - ENT NOSE LECTURESDocument38 pagesSimply Put - ENT NOSE LECTURESCedric KyekyeNo ratings yet
- Final Examination Rubric On The Zumba Exercises RoutineDocument1 pageFinal Examination Rubric On The Zumba Exercises RoutinePizzaTobacco123100% (1)
- 2018 - Shiau - Evaluation of A Flipped Classroom Approach To Learning Introductory EpidemiologyDocument9 pages2018 - Shiau - Evaluation of A Flipped Classroom Approach To Learning Introductory EpidemiologySocorro Moreno LunaNo ratings yet
- Fifa 11+Document7 pagesFifa 11+HeiYu TongNo ratings yet
- Essentials of Neurology 2Document153 pagesEssentials of Neurology 2prahul2588100% (7)
- Sub Station ReportDocument43 pagesSub Station ReportSithartha SouryaNo ratings yet
- Insect Milk: VocabularyDocument3 pagesInsect Milk: VocabularyChris Mae Vinson DalumpinesNo ratings yet
- Types of CompressorsDocument44 pagesTypes of Compressorsjezreeleda.limNo ratings yet
- Diabettes Mellitus and Cognitive ImpairmentsDocument12 pagesDiabettes Mellitus and Cognitive ImpairmentsPutri YunandaNo ratings yet
- Specifications of Materials and Finishes: Project: Location: OwnerDocument66 pagesSpecifications of Materials and Finishes: Project: Location: OwnerHarry Ecal100% (1)
- ESWT - For Myositis Ossificans CaseDocument13 pagesESWT - For Myositis Ossificans CaseSienriesta NovianaNo ratings yet
- Brunei 2Document16 pagesBrunei 2Eva PurnamasariNo ratings yet
- Biology Revision Notes Part3Document10 pagesBiology Revision Notes Part3volvanskyNo ratings yet
- Brain Breaks: Animal WalksDocument6 pagesBrain Breaks: Animal WalksMárcia DiasNo ratings yet
- Proposal HR OutsourcingDocument7 pagesProposal HR Outsourcingraqi14850% (6)