Professional Documents
Culture Documents
Australian Psychologist - 2012 - Duncan - Adolescents Risk Behaviour and Confidentiality When Would Australian
Australian Psychologist - 2012 - Duncan - Adolescents Risk Behaviour and Confidentiality When Would Australian
Uploaded by
7sunqiiOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Australian Psychologist - 2012 - Duncan - Adolescents Risk Behaviour and Confidentiality When Would Australian
Australian Psychologist - 2012 - Duncan - Adolescents Risk Behaviour and Confidentiality When Would Australian
Uploaded by
7sunqiiCopyright:
Available Formats
bs_bs_banner
ORIGINAL ARTICLE
Adolescents, Risk Behaviour and Confidentiality: When Would
Australian Psychologists Breach Confidentiality to Disclose
Information to Parents?
Rony E Duncan,1,2,3,4 Ben J Williams,4 and Ann Knowles4
1
The Centre for Adolescent Health, Royal Children’s Hospital, 2Murdoch Childrens Research Institute, 3Department of Paediatrics, The University of
Melbourne, and 4Psychological Sciences and Statistics, Faculty of Life and Social Sciences, Swinburne University of Technology
The protection of confidentiality in psychological practice is vital. However, confidentiality is not absolute and psychologists are permitted to
breach confidentiality under particular circumstances. Ethical challenges surrounding confidentiality are complex with adolescent clients, as
assessments often consider the risk that adolescents pose to themselves in addition to the risk posed to others. The current study documented
situations in which Australian psychologists would breach adolescents’ confidentiality to disclose information about risk behaviour to parents,
with a focus on situations where adolescents posed a risk to themselves as opposed to other people putting adolescents at risk. A total of 264
Australian psychologists were surveyed online. They were each presented with 68 variations of a vignette about a 15-year-old boy who was
engaged in risk behaviour and were asked whether they would breach confidentiality in each case. The vignettes covered six behavioural
domains (smoking, sexual behaviour, drinking, drug use, suicide, stealing) and varied in behaviour intensity, frequency and duration. Consensus
was reached about breaching confidentiality in 16% of cases (related to sexual behaviour, drug use, and suicide). Consensus was reached about
not breaching confidentiality in 41% of cases (relating to smoking, sexual behaviour, drug use, suicide, and stealing). In the remaining 43% of
cases, significant disagreement occurred (relating to all six behavioural domains). The findings suggest a high degree of variation in opinion about
confidentiality with adolescents, emphasising the importance of transparent communication and informed consent. The findings also raise
questions about how important consistency of psychological practice is across Australia.
Key words: adolescent; confidentiality; ethics; minors; psychiatry; psychology.
What is already known on this topic What this paper adds
1 Confidentiality is necessary if adolescents are to disclose sensi- 1 The current article presents the views of 264 Australian psycholo-
tive and personal information to health professionals. gists about whether they would breach confidentiality with an ado-
2 Confidentiality in the psychological setting is not absolute. Psy- lescent client to disclose information about risk behaviour to
chologists are permitted to breach confidentiality under a range parents across 68 different vignettes. This is an important resource
of circumstances, including when an immediate and specified for professionals to contrast their own views and current practice.
risk of harm is present. 2 Respondents reached consensus about whether to breach confi-
3 Adolescent clients pose specific challenges regarding confiden- dentiality in the most high-risk and low-risk vignettes that were
tiality for psychologists because assessments of risk need to presented. However, in 43% of cases, respondents failed to reach
include not only the level of risk they pose to others but also the consensus about whether a breach of confidentiality was neces-
level of risk they pose to themselves. sary. This implies considerable variation among Australian psy-
chologists’ views regarding confidentiality with adolescent clients.
3 Given that variation exists in psychologists’ opinions about con-
fidentiality with adolescent clients, it is likely that current practice
varies also. It is therefore imperative that psychologists are clear
in their communication with adolescent clients and clients’
parents about their limits to confidentiality in order to uphold
principles of transparency and informed consent.
Correspondence: Rony Duncan, Centre for Adolescent Health, Level 2, Royal Children’s Hospital, Parkville, VIC 3052, Australia. Fax: +61 (3) 9345 6273; email:
rony.duncan@mcri.edu.au
Accepted for publication 23 October 2012
doi:10.1111/ap.12002
408 Australian Psychologist 48 (2013) 408–419
© 2012 The Australian Psychological Society
17429544, 2013, 6, Downloaded from https://aps.onlinelibrary.wiley.com/doi/10.1111/ap.12002 by Monash University, Wiley Online Library on [23/04/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
RE Duncan et al. Adolescents, risk behaviour and confidentiality
Confidentiality is essential for building effective therapeutic regarding confidentiality with students specifically (American
relationships within the psychological practice. However, psy- School Counselor Association, 2004). School psychologists
chologists have also described confidentiality as the cause of working in the USA are advised that their primary obligation is to
their most serious ethical dilemmas (Haas, Malouf, & Mayerson, the student and that information should remain confidential
1986; Pope & Vetter, 1992). Although fundamental, confiden- unless disclosure is required to prevent clear and imminent
tiality between therapists and clients can never be absolute, and danger to the student or others, or when legal requirements exist.
it is this stipulation that creates scope for ethical complexity and Detailed guidance about confidentiality with adolescents also
confusion (Jain & Roberts, 2009; Kampf, McSherry, Thomas, & exists outside the field of psychology. The position statements
Abrahams, 2008). Determining appropriate limits to confiden- of every major medical organisation, including the World Health
tiality, and making decisions about which cases require a breach Organisation (WHO), support confidential health care for ado-
of confidentiality, can be highly challenging and ethically lescents (American Academy of Paediatrics, 2008; American
fraught. This is especially true when clients are minors. Medical Association, 1993, 1994; Berlan & Bravender, 2009;
The phase of adolescence is often defined by societies in Ford, English, & Sigman, 2004; Society for Adolescent Medi-
relation to a combination of age and social roles, which can cine, 2004a; Wheeler, 2006; World Health Organisation [WHO],
result in little consistency across countries (Sawyer et al., 2012). 2002). In particular, the Society for Adolescent Medicine (SAM)
Unless otherwise stated, in the current article we use the terms has published a policy statement on confidential health care
“adolescents,” “young people,” and “minors” interchangeably for adolescents (Society for Adolescent Medicine, 2004b). This
to refer to people under the age of 18 years, in line with the states that “confidentiality is an essential component of health
Australian Psychological Society (APS) definition of “young care for adolescents because it is consistent with their develop-
people” (Australian Psychological Society, 2009). However, we ment of maturity and autonomy” (p. 160).
note that international definitions of adolescence are moving
towards a broader definition, encompassing those aged 10–24 The Ethical Complexity
years (Sawyer et al., 2012). This broader age-range is reflected Surrounding Confidentiality
in some of the literature we reference.
Despite the level of international consistency regarding
Guidelines Concerning Confidentiality guidance about confidentiality in psychological practice, it has
been argued that the application of these seemingly simple
Current guidance regarding confidentiality within psychological recommendations is in fact highly complex (Davis & Mickelson,
practice is internationally consistent. The APS has published 1994; Gustafson & McNamara, 1987; Isaacs & Stone, 1999;
the Code of Ethics (Australian Psychological Society, 2007). This Kaczmarek, 2000; Ledyard, 1998; Myers, 1982; Taylor &
requires psychologists to “safeguard the confidentiality of infor- Adelman, 1989) and not well understood by practitioners
mation obtained during their provision of psychological serv- (Fisher, 2008; Haas et al., 1986; Pope & Vetter, 1992; Younggren
ices” (p, 15). The Code also clarifies circumstances under which & Harris, 2008). Davidson (1995) in his review of articles con-
psychologists are permitted to disclose confidential information cerning confidentiality in psychological practice, explained that
that has been provided to them by their clients. These include disagreement exists in the field of psychology about what con-
situations in which the client (or the client’s legal guardian) stitutes harm and who should be protected. He also noted that
has provided consent, where there is a legal obligation to do so, legal, ethical, and professional codes can compete with one
where there is an immediate risk of harm that can only be another which means that deciding which to follow can consti-
averted by disclosing information, or when colleagues or super- tute a challenging task. McMahon and Knowles (1995) argue
visors need to be consulted. that although obligations of confidentiality are well known,
The APS has also recently published a detailed set of guidelines they are complicated by a range of factors such as legal protec-
specifically on working with young people (Australian Psycho- tions, ethical beliefs, institutional practices, and professional
logical Society, 2009). In relation to confidentiality, these guide- codes. The complexities associated with obligations of confiden-
lines are definitive about the need to prioritise young people’s tiality are therefore numerous, and it is perhaps not surprising
best interests above those of parents, as long as young people are that previous research indicates psychologists are confused
deemed competent. The guidelines specifically state that “psy- about when to breach confidentiality (Kampf et al., 2008).
chologists respect the young person’s wishes regarding confiden-
tiality and do not divulge any confidential information contrary Adolescents, Confidentiality, and
to the young person’s wishes, except as specified in section Psychological Care
5.1—Limits to Confidentiality” (p, 183). The “limits to confiden-
tiality” referred to are in line with those outlined in the APS Code Much has been written about the way in which confidentiality
of Ethics, described above. dilemmas are magnified when clients are minors (Sobocinski,
The American Psychological Association (APA) also has a Code 1990). Lawrence and Kurpius (2000) state that confidentiality
of Conduct (American Psychological Association, 2002). This is one of the most difficult legal and ethical dilemmas facing
closely mirrors the guidance outlined in the APS Code of Ethics, psychologists who work with minors. Milne (1995) argues that
although a specific discussion of therapy with young people is not issues regarding counsellor–client confidentiality pose particular
present. In addition to the APA’s Code of Conduct, the American difficulties when counselling is provided to adolescents directly.
School Counselor Association (ASCA) has published a document Isaacs and Stone (1999) suggest that managing confidentiality is
titled “Ethical Standards,” and this outlines the obligations often the most difficult ethical issue facing school counsellors.
Australian Psychologist 48 (2013) 408–419 409
© 2012 The Australian Psychological Society
17429544, 2013, 6, Downloaded from https://aps.onlinelibrary.wiley.com/doi/10.1111/ap.12002 by Monash University, Wiley Online Library on [23/04/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
Adolescents, risk behaviour and confidentiality RE Duncan et al.
McCurdy and Murray (2003) highlight the dilemmas that arise high school students found that 98% of adolescents believed
during family therapy, when minors are often seen alone for that confidentiality within a school counselling setting was
some sessions and may reveal private information during this either essential or important (Collins & Knowles, 1995). It has
time that is pertinent to the family situation. Several authors also been shown that the number of disclosures regarding sen-
have also noted the ambiguity of professional codes and laws sitive questions is higher when confidentiality is explicitly
regarding confidentiality with adolescent clients specifically assured by psychologists (Kobocow, McGuire, & Blau, 1983).
(Isaacs & Stone, 1999; Lawrence & Kurpius, 2000; McCurdy & Findings about the importance of confidentiality for young
Murray, 2003; Mitchell, Disque, & Robertson, 2002; Moyer & people have also been demonstrated extensively in the field of
Sullivan, 2008; Sealander, Schwiebert, Oren, & Weekley, 1999). adolescent medicine (Farrant & Watson, 2004; Ford, Millstein,
Less well articulated in existing literature is why young people Halpern-Felsher, & Irwin, 1997; Jones, Purcell, Singh, & Finer,
pose such a problem for notions of confidentiality in the psy- 2005; Reddy, Fleming, & Swain, 2002; Thrall et al., 2000).
chological setting. That is, what makes adolescents so different Most of the empirical research conducted with psychologists
from adults and thus the cause of such additional ethical uncer- and counsellors about confidentiality with adolescent clients has
tainty? Adolescents differ from adults in their cognitive, psycho- come from the USA. Beeman and Scott (1991) surveyed Ameri-
logical, and social capabilities and also in relation to the extent can psychologists in training and asked them to rate the impor-
of life experience they have had (Hazen, Schlozman, & Beresin, tance of a range of information provision to clients, finding that
2008). When contemplating ethical challenges of confidentiality information regarding the limits to confidentiality scored the
with adult clients, dilemmas often relate to whether the client highest of all types of information proposed. Davis and Mickel-
poses a risk to others; sometimes referred to as determina- son (1994) surveyed American school counsellors. They found
tions of the “dangerous” client (McMahon & Knowles, 1997). that there was less than 50% agreement on the preferred ethical
However, with adolescents, determinations about confidential- or correct legal choices in relation to dilemmas of student
ity often relate to whether the young person poses a risk to privacy, confidentiality, and parental rights. Isaacs and Stone
themselves as a consequence of engaging in risk behaviours. Such have conducted two studies with American counsellors about
determinations necessarily entail an assessment of maturity or confidentiality with minors (1999, 2001). In the first survey
competence as well, further increasing the ethical complexity. they asked school counsellors about the circumstances in
Psychological care is vital for adolescents, with research indi- which they would breach confidentiality with clients who were
cating a range of reasons to be concerned about their health and minors. The majority of counsellors reported that they would
well-being. Worldwide, there are over 1.8 billion young people breach confidentiality for the following issues: impending
aged 10–24 years, which is the largest adolescent population in suicide, retaliation for victimisation, use of crack cocaine, sex
history (Sawyer et al., 2012). Alcohol misuse alone is estimated with multiple partners when HIV positive, armed robbery, indi-
to account for 31.5% of all the deaths in 15–29 year old men in cations of depression, abortion, and marijuana use. They also
the developed world (Toumbourou et al., 2007). Statistics from found that the degree of dangerousness and also the minor’s age
the Australian Institute of Health and Welfare (AIHW) indicate influenced counsellors’ decisions about breaching confidential-
that almost one third of Australian young people aged 12–24 ity (Isaacs & Stone, 1999). In their second study, they surveyed
years of age drink alcohol in amounts that put them at risk of mental health counsellors and found that the same two factors;
harm in the short term, and around 17% are current smokers dangerousness of the behaviour and the client’s age impacted
(Australian Institute of Health and Welfare, 2007). In relation to on counsellors’ decisions about breaching confidentiality (Isaacs
sexual practices, 26% of Australian youth aged 12–24 years have & Stone, 2001).
engaged in sexual intercourse by the time they reach Year 10, Rae, Sullivan, and colleagues have conducted a number of
rising to 47% by Year 12. Disturbingly, 25% of males and 20% of studies aimed at documenting when psychologists and counsel-
females in Year 12 did not use a condom the last time they had sex lors would breach confidentiality with adolescent clients and
(Australian Institute of Health and Welfare, 2007). Injury con- what factors influence their decisions. The current study par-
tinues to be the leading cause of death in those aged 12–24 years, tially replicated their initial study, which entailed a survey
accounting for two thirds of all the deaths in this group. 74 American paediatric psychologists (Rae, Sullivan, Razo,
The prevalence of mental health problems among Australian George, & Ramirez, 2002; Sullivan, Ramirez, Rae, Razo, &
adolescents aged 13–17 years is 19%, and this increases to George, 2002). Findings from this initial study were published
27% among young adults aged 18–24 years (McGorry, Purcell, in two separate manuscripts. The first manuscript presented
Hickie, & Jorm, 2007). In fact, mental health disorders account the considerations that psychologists take into account when
for almost 50% of the total disease burden among young people making decisions about breaching confidentiality with adoles-
aged 12–24 years (Australian Institute of Health and Welfare, cent clients (Sullivan et al., 2002). Participants were presented
2007). Prevention and early intervention are thus both possible with 13 considerations and were asked to rate the importance of
and highly desirable for adolescents (Sanci, Sawyer, Kang, each for their decisions about confidentiality. Factor analysis of
Haller, & Patton, 2005). these responses provided support for a two-factor model to fit
the data. These two factors were termed “Negative Nature of
Empirical Research about Confidentiality in the Behaviour” and “Maintaining the Therapeutic Process.” The
Psychological Practice second manuscript presented the circumstances in which psy-
chologists believed it was ethical to breach confidentiality with
Research with young people demonstrates that adolescents adolescent clients (Rae et al., 2002). Vignettes describing a range
place a high value on confidentiality. A survey of Melbourne of adolescent risk behaviours were presented to participants,
410 Australian Psychologist 48 (2013) 408–419
© 2012 The Australian Psychological Society
17429544, 2013, 6, Downloaded from https://aps.onlinelibrary.wiley.com/doi/10.1111/ap.12002 by Monash University, Wiley Online Library on [23/04/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
RE Duncan et al. Adolescents, risk behaviour and confidentiality
and they were asked to rate how ethical it would be to breach Table 1 A Comparison of Demographic Characteristics between the
confidentiality and inform parents. The risk behaviours covered Study Sample and APS Members
six behavioural domains and across all of these, psychologists % of sampleb % APSa
were more likely to indicate that a breach of confidentiality was
ethical as the intensity, frequency, and duration of the behav- State of registration
iour increased. NSW 29 32
Rae, Sullivan, and colleagues have since replicated this survey VIC 29 33
with school psychologists and school counsellors. In surveying QLD 15 19
school counsellors they found, again, that as the intensity, dura- SA 6 6
tion, and dangerousness of the risk behaviour increased, so too TAS 5 2
did the propensity for school counsellors to deem a breach of WA 12 8
ACT 3 3
confidentiality ethical. They also found that although agree-
NT 1 1
ment occurred about the ethicality of breaching confidentiality
Age
in high-risk circumstances, such as a suicide attempt, disagree-
<30 23 14
ment occurred among respondents regarding less high-risk
30–39 35 26
behaviours (Moyer & Sullivan, 2008). They also found that
40–49 20 23
school psychologists used a vast range of complex considera- 50–59 16 22
tions in determining whether a breach of confidentiality was 60+ 6 15
ethical (Sullivan & Moyer, 2008). In surveying school psycholo- Gender
gists they found, yet again, that as the intensity, duration, and Male 13 21
dangerousness of the risk behaviour increased, so too did the Female 87 79
tendency for school psychologists to breach an adolescent’s con-
a
fidentiality (Rae, Sullivan, Razo, & De Alba, 2009). Demographic data from membership profile in APS (2011) Annual Report.
b
The current study aimed to replicate the initial American study Two participants did not supply the state they were practicing in.
described above (Rae et al., 2002; Sullivan et al., 2002) in order
to examine the considerations that Australian psychologists use
for making decisions about confidentiality with adolescents and 3% of the participants were still completing their qualifications.
also to document the circumstances in which Australian psy- The psychologists sampled worked in a range of settings, with
chologists believe it is appropriate to breach confidentiality with 26% working in schools, 22% in private practice, 11% in the
adolescents. The findings related to the considerations that psy- public sector, and small numbers working in a university, com-
chologists use in making such decisions have been published munity, or government settings. Eighty-two per cent of the par-
separately (Duncan, Williams, & Knowles, 2012). Here, findings ticipants were members of the APS. Currently, there is no
are presented in relation to the circumstances in which Austral- available demographic profile of Australian psychologists who
ian psychologists believe it is appropriate to breach confidential- work with young people. However, data are available for the
ity with adolescent clients. The focus was circumstances in which overall APS membership (Australian Psychological Society,
adolescents were posing a risk to themselves, as opposed to 2011). The age distribution in the current study sample was
situations in which another person was putting the adolescent at broadly comparable to the APS membership, although respond-
risk. The findings of the current study offer an empirical basis for ents under 30 and over 60 years of age were overrepresented in
comparison so that Australian psychologists can contrast their the sample, as were women. These differences may reflect the
own practice and opinions with that of their colleagues. characteristics of psychologists who work with adolescents or
may be due to the means used to collect data (i.e., familiarity
with the Internet). The geographic distribution of our partici-
Method pants closely matched the APS membership profile, with the
exception that Tasmania and Western Australia were signifi-
Participants cantly over-represented. Table 1 presents a comparison of
Participants were required to be working in Australia, have demographic characteristics between the study sample and APS
experience working with young people, and either studying members.
to become or qualified as a registered psychologist. While 282 Materials
people responded to the questionnaire, 18 either did not fit
these criteria or omitted over 10% of the questionnaire items An online questionnaire was used to survey the psychologists
and were consequently excluded from the sample, leaving a in this study and was adapted from the previous study being
total of 264 participants. The majority (87%) of the participants replicated (Rae et al., 2002; Sullivan et al., 2002). The question-
were female, and 13% were male, with an overall mean age of naire consisted of two parts; Part A related to the situations in
39 years (SD = 11) and most lived in the Australian states of which psychologists would deem it appropriate to breach con-
New South Wales or Victoria. They had a mean number of 9.5 fidentiality with adolescents, and Part B related to the consid-
years experience working with young people (SD = 7.8). A total erations they take into account when making such decisions.
of 42% had completed a 4-year degree plus 2 years of supervi- This article reports results from Part A of the questionnaire only.
sion, 49% had completed either a Doctorate of Psychology or a Results from Part B have been published separately (Duncan
Masters Degree, 7% had completed a PhD, and the remaining et al., 2012).
Australian Psychologist 48 (2013) 408–419 411
© 2012 The Australian Psychological Society
17429544, 2013, 6, Downloaded from https://aps.onlinelibrary.wiley.com/doi/10.1111/ap.12002 by Monash University, Wiley Online Library on [23/04/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
Adolescents, risk behaviour and confidentiality RE Duncan et al.
Table 2 The 68 Scenarios Presented in the Questionnaire (17 Categories of Risk Behaviour Each Divided into Four Levels of Frequency/Duration)
Behavioural domain 17 categories of risk behaviour Four levels of frequency/duration
Smoking Smoking one cigarette
Smoking more than a pack of cigarettes
Drinking One drink
Binge drinking
Sexual behaviour Sex with a girlfriend once several months ago
Sex with multiple partners monthly for several months
Unprotected sex while HIV+ weekly for several months
Drug use Using marijuana nearly daily for the last year
Using amphetamines
Using hallucinogens
Using inhalants
Suicide Suicidal ideation (“I wish I was dead”)
Suicide gesture (taking pills) once over a year ago
Suicide attempt (trying to hang himself) once several months ago
Stealing Stealing clothing from a store once during last month
Stealing a car more than once during last month
Breaking into homes and stealing valuables
Part A of the questionnaire used hypothetical vignettes to 6-point Likert scale. The authors of the previous study suggested
document situations in which psychologists would breach con- this alteration in design for future studies so that participants
fidentiality with adolescent clients and disclose information to would be forced to make a definitive choice, and more infor-
the adolescents’ parents about risk behaviour. Participants were mation could be gathered about where the tipping point lies for
first presented with the following hypothetical scenario: breaching confidentiality in such situations. The past study also
used two versions of the vignette, one that described a female
Chris is a 15-year-old male who was referred by his parents for client and one that described a male client. The current study
disrespectful, acting out, and oppositional behaviour that has become did not vary the gender of the client in the vignette. This was
much worse in the last few months. Chris is an only child of working due to limitations of the online questionnaire tool used
parents who describe themselves as middle class. His parents have (it was not possible to randomly allocate two versions of the
brought Chris to treatment, and he is not enthusiastic about the vignette online; one with a male client and one with a female
therapy since he does not believe that he has a “problem.” Chris is client). The previous American study used hard copies of the
also very concerned about confidentiality, but his parents have agreed questionnaire, and so the researchers were able to send out
that they will not ask you for details about the content of the therapy two different versions. The 17 risk behaviours covered six key
sessions. You assure Chris that you will only break confidentiality behavioural domains. These were: smoking; drinking; sexual
to his parents (or others) if he presents a danger to himself or to behaviour; drug taking; suicide; and stealing. Table 2 presents
others. During the sixth therapy session, Chris begins admitting to the 17 risk behaviours alongside the four levels of frequency/
risk-taking behaviours. duration that were presented in the questionnaire.
Participants were then provided with 17 different categories Procedure
of risk behaviour that Chris had engaged in, and each of the 17
categories was then divided into four separate levels of Following the receipt of University ethics approval, requests to
frequency/duration. Thus, in total, there were 68 different sce- participate were distributed in two ways. First, the study was
narios (17 categories, each divided into four levels of frequency/ advertised through a fortnightly APS email newsletter and a
duration). For example, the first of the 17 categories was “Chris notice on the APS website with a link to the study website.
admits to smoking one cigarette,” and the four levels of frequency/ Second, participants were invited via personal emails, which
duration related to this category were: once several months ago; included details about the survey and a link to the survey
monthly for several months; weekly for several months; and nearly website. This email distribution used the snowballing technique
daily for the last year. These 68 scenarios were taken from the in which the researchers emailed colleagues who were then
study being replicated. asked to forward the email to their colleagues and so on. This
For each of the 68 scenarios, participants were asked to indi- methodology meant that a response rate for the current study
cate whether they would breach confidentiality and inform could not be calculated as it is not known how many people
Chris’s parents about the risk behaviour. They did so on a binary received notification of the survey.
scale (yes, no), which differed from the previous American Participants completed the survey online and submitted their
study where participants were asked to rate “how ethical” a responses anonymously by clicking on a button titled submit at
breach of confidentiality would be in each scenario using a the end of the survey. An incentive was provided to potential
412 Australian Psychologist 48 (2013) 408–419
© 2012 The Australian Psychological Society
17429544, 2013, 6, Downloaded from https://aps.onlinelibrary.wiley.com/doi/10.1111/ap.12002 by Monash University, Wiley Online Library on [23/04/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
RE Duncan et al. Adolescents, risk behaviour and confidentiality
participants in the form of a $100 book/CD voucher prize draw. 100
Participants who wanted to be considered for this prize were
asked to provide a name and telephone number at the end of
80
the questionnaire. These details were separated from the ques-
Binge drinking
% would breach
tionnaire responses to maintain anonymity.
One drink
60
Smoking a pack of cigarettes
Results Smoking one cigarette
40
A cut-off of 80% agreement was used to indicate consensus
among participants about their views on whether to breach
20
confidentiality or not, in response to each vignette. This is con-
sistent with Pope, Tabachnick, and Keith-Spiegel (1988) who
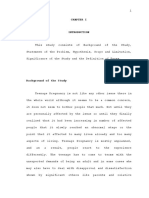
argued that 80% indicated “a clear majority”. Figures 1 and 2 0
present the percentage of participants who would breach
confidentiality with an adolescent client to inform parents of
100
risk behaviour across the four levels of frequency/duration, for
each of the six behavioural domains (smoking, drinking, sexual
behaviour, drug taking, suicide, and stealing). Within each 80
figure, responses have been separated into the different levels of
% would breach
behavioural intensity for each behavioural domain. 60
Respondents demonstrated greater than 80% consensus that
confidentiality should be breached in 11 of the 68 vignettes
40
(16%). These 11 items are presented in Table 3. They reflect a
range of high-intensity risk behaviours, including drug taking, Using inhalants
Using hallucinogens
suicidal behaviour, and engaging in unprotected sex while 20
Using amphetamines
HIV+. The highest level of consensus about breaching confiden- Smoking marijuana
tiality was 96%. This was achieved in relation to breaching 0
confidentiality following an admission of a suicide attempt more
than once in the last month.
Respondents demonstrated greater than 80% consensus 100
about not breaching confidentiality in 28 of the 68 vignettes
(41%). These 28 items are presented in Table 4. The circum-
80
stances prompting consensus about not breaching confidential-
% would breach
ity included a range of low-risk behaviours such as smoking
cigarettes and engaging in sex with a steady girlfriend, as well as 60
Sex while HIV+
a range of higher risk behaviours at low intensities, such as
Sex with multiple partners
engaging in illicit drug taking once several months ago or binge 40 Sex with steady girlfriend
drinking once a month for several months. The highest level
of consensus reached about not breaching confidentiality was
20
98%. This was achieved in relation to two items: smoking a pack
of cigarettes and/or binge drinking alcohol once several months
ago. 0
once monthly weekly nearly daily
Thus, there were a large range of circumstances in which several for several for several for the
participants did not believe a disclosure about risk behaviour months ago months months last year
by an adolescent client necessitated a breach of confidentiality Frequency of risk behaviour
to the adolescents’ parents. These circumstances far outweighed
the number of situations in which consensus was reached about Figure 1 Percentage of Participants Who Would Breach Confidentiality,
breaching confidentiality. There were 29 vignettes (43%) in Depending on Intensity and Frequency/Duration of Smoking, Drinking, Drug
which participants did not reach 80% consensus about whether Taking, and Sexual Behaviour.
to breach confidentiality. Table 5 presents these 29 items.
The tendency to breach confidentiality to inform parents of risk
behaviours increased across all six behavioural domains as the
frequency, intensity, and duration of the behaviour increased. adolescents’ parents about risk behaviour. The focus of the study
was circumstances in which adolescents were posing a risk to
Discussion themselves, as opposed to situations in which another person
was posing a risk to the adolescent. The study replicated a
The current study aimed to examine the situations in which previous study of American psychologists, published in two
Australian psychologists would breach confidentiality with parts, that examined when psychologists would breach confi-
an adolescent client in order to disclose information to the dentiality with adolescent clients (Rae et al., 2002) and what
Australian Psychologist 48 (2013) 408–419 413
© 2012 The Australian Psychological Society
17429544, 2013, 6, Downloaded from https://aps.onlinelibrary.wiley.com/doi/10.1111/ap.12002 by Monash University, Wiley Online Library on [23/04/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
Adolescents, risk behaviour and confidentiality RE Duncan et al.
100 months ago and one session of binge drinking several months
ago. The highest level of consensus reached about needing to
80 breach confidentiality was 96%, and this was achieved in rela-
tion to the vignette stating that a suicide attempt had occurred
% would breach
Stealing a car
more than once in the last month.
60 Breaking into homes
Stealing clothing It was more common for respondents to demonstrate consen-
sus about not needing to breach confidentiality than it was for
40 respondents to demonstrate consensus about breaching confi-
dentiality. Respondents reached consensus about not needing to
20 breach confidentiality in 41% of vignettes, whereas in only 16%
of vignettes was consensus reached about breaching confiden-
0 tiality. The most common outcome was therefore a situation in
which respondents failed to reach consensus about breaching or
not breaching confidentiality.
100 In 43% of the vignettes, respondents did not achieve con-
sensus about breaching or not breaching confidentiality. This
implies a significant degree of variation among respondents’
80
views regarding appropriate limits to confidentiality with ado-
% would breach
lescent clients engaged in risk behaviour. This disagreement
60
among respondents has also been found in past studies using
the same survey with American school counsellors. School
Suicide attempt
40 counsellors demonstrated agreement in relation to the most
Suicide gesture
Suicide ideation high-risk behaviours, such as suicide attempts; but for less high-
20 risk behaviours, they demonstrated a distinct lack of agreement
(Moyer & Sullivan, 2008).
0 One possible explanation for the significant variation in
once over once several once during more than opinion demonstrated by respondents in the current study is
a year ago months ago the last month once last month
that Australian psychologists are uncertain about when to
Frequency of risk behaviour breach confidentiality with an adolescent client to inform
parents about risk behaviour. That is, they are unclear about
Figure 2 Percentage of Participants Who Would Breach Confidentiality, precisely how to interpret “an immediate and specified risk of
Depending on Intensity and Frequency/Duration of Stealing and Suicidal harm” as specified in the APS Code of Ethics (p. 15). The
Behaviour. challenges associated with interpreting such statements have
also been discussed in previous literature regarding the notion
of “clear and imminent danger” that school counsellors in the
USA are advised to identify (Moyer & Sullivan, 2008).
factors psychologists use in their decision-making process (Sul- If the difference in opinion among respondents in the current
livan et al., 2002). The findings of the current study have simi- study reflects a lack of knowledge among Australian psycho-
larly been separated into two articles. This article presents logists about when a breach of confidentiality is appropriate,
findings related to when Australian psychologists would breach this would suggest a need for targeted training and support to
confidentiality with adolescent clients, while the findings about decrease the uncertainty and increase Australian psychologists’
the factors that Australian psychologists use in their decision- understanding and confidence about appropriate limits to con-
making processes have been published separately (Duncan fidentiality with adolescent clients (Isaacs & Stone, 2001; Moyer
et al., 2012). & Sullivan, 2008; Sullivan & Moyer, 2008). Current guidelines
To examine the circumstances in which Australian psycholo- do not provide in-depth information about the types of circum-
gists would breach confidentiality with adolescent clients, stances that constitute harm, leaving individual psychologists
respondents were presented with 68 variations of a vignette with the task of making their own professional judgments
in which a 15 year-old boy engaged in risk behaviour. The (Isaacs & Stone, 2001). In these circumstances, where guidance
vignettes covered six domains of risk behaviour (smoking, is not specific, it is therefore critical that appropriate supports
drinking, sexual behaviour, drug taking, suicide, and stealing) are in place. Processes and supports might include an opportu-
and varied in intensity, frequency and duration. For each nity to seek advice from colleagues or a supervisor, to seek
vignette, respondents were asked to indicate whether they assistance from a professional body, such as the APS, or to access
would breach confidentiality to inform the boy’s parents about information about what other psychologists have decided in
his behaviour. Consensus among respondents was defined as a similar circumstances. Younggren and Harris (2008) specifically
minimum of 80% agreement. highlight the need for psychotherapists to engage in peer
There was no vignette in which 100% consensus was consultation when confronted with confidentiality dilemmas.
reached. The highest level of consensus reached about not It might also be important for psychologists to have thorough
breaching confidentiality was 98%, and this was achieved in training in “normal” adolescent development so that they have
relation to two vignettes: smoking a packet of cigarettes several an understanding of the range of risk behaviours that are
414 Australian Psychologist 48 (2013) 408–419
© 2012 The Australian Psychological Society
17429544, 2013, 6, Downloaded from https://aps.onlinelibrary.wiley.com/doi/10.1111/ap.12002 by Monash University, Wiley Online Library on [23/04/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
RE Duncan et al. Adolescents, risk behaviour and confidentiality
Table 3 Circumstances in which Participants Demonstrated ⱖ80% Consensus that Confidentiality Should Be Breached to Inform Parents
Risk behaviour Level of frequency/duration % who would breach
confidentiality
Engaging in unprotected sex while HIV+ monthly for several months 87
weekly for several months 88
nearly daily for the last year 89
Using amphetamines nearly daily for the last year 80
Using inhalants nearly daily for the last year 83
Using hallucinogens nearly daily for the last year 82
Suicidal ideation (“I wish I was dead”) nearly daily for the last year 85
Suicide gesture (taking pills) once during the last month 87
more than once during last month 94
Suicide attempt (trying to hang himself) once during the last month 93
more than once during last month 96
Table 4 Circumstances in which Participants Demonstrated ⱖ80% Consensus that Confidentiality Should Not Be Breached to Inform Parents
Risk behaviour Level of frequency/duration % who would not breach
confidentiality
Smoking one cigarette once several months ago 97
monthly for several months 97
weekly for several months 96
nearly daily for the last year 92
Smoking more than a pack of cigarettes once several months ago 98
monthly for several months 95
weekly for several months 91
Engaging in sex with a steady girlfriend once several months ago 96
monthly for several months 91
weekly for several months 88
nearly daily for the last year 85
Engaging in sex with multiple partners once several months ago 94
monthly for several months 86
Drinking one drink once several months ago 97
monthly for several months 97
weekly for several months 90
Binge drinking once several months ago 98
monthly for several months 82
Smoking marijuana once several months ago 97
monthly for several months 82
Using amphetamines once several months ago 93
Using inhalants once several months ago 91
Using hallucinogens once several months ago 90
Suicidal ideation (“I wish I was dead”) once several months ago 83
Stealing clothing from a store once over a year ago 96
once several months ago 95
once during the last month 87
Stealing a car for a joyride with friends once over a year ago 83
common during this life stage in order to help them determine for situations that are not at the extremes of high or low risk,
whether a specific behaviour falls outside this norm. a decision about whether to breach confidentiality is depend-
A second possible explanation for the differences in opinion ent on additional, contextual factors. The vignettes presented
demonstrated in the current study is that perhaps not all within the survey were lacking in detail about contextual
scenarios in which an adolescent client is engaged in risk behav- factors. Thus, it is possible that individual respondents were
iour have a concrete and definitive “correct” response regarding swayed about whether to breach confidentiality based on
whether a breach of confidentiality is necessary. It might be that personal assumptions made about the context. For example,
Australian Psychologist 48 (2013) 408–419 415
© 2012 The Australian Psychological Society
17429544, 2013, 6, Downloaded from https://aps.onlinelibrary.wiley.com/doi/10.1111/ap.12002 by Monash University, Wiley Online Library on [23/04/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
Adolescents, risk behaviour and confidentiality RE Duncan et al.
Table 5 Circumstances in which Participants Demonstrated Significant Disagreementa about Whether Confidentiality Should be Breached to Inform Parents
Risk behaviour Level of frequency/duration % who would breach
confidentiality
Smoking more than a pack of cigarettes nearly daily for the last year 22
Engaging in sex with multiple partners weekly for several months 26
nearly daily for the last year 36
Engaging in unprotected sex while HIV+ once several months ago 73
Drinking one drink nearly daily for the last year 35
Binge drinking weekly for several months 39
nearly daily for the last year 70
Smoking marijuana weekly for several months 40
nearly daily for the last year 67
Using amphetamines monthly for several months 41
weekly for several months 65
Using inhalants monthly for several months 50
weekly for several months 71
Using hallucinogens monthly for several months 51
weekly for several months 71
Suicidal ideation monthly for several months 53
weekly for several months 74
Suicide gesture once over a year ago 38
once several months ago 56
Suicide attempt once over a year ago 54
once several months ago 72
Stealing clothing from store more than once during last month 32
Stealing a car for a joyride with friends once several months ago 17
once during the last month 24
more than once during last month 45
Breaking into homes and stealing valuables once over a year ago 21
once several months ago 30
once during the last month 47
more than once during last month 64
a
Significant disagreement is defined as <80% agreement.
respondents might have made assumptions about the quality of to vignettes that were not situated at the extreme ends of high
the adolescent’s family relationships or how often similar or low risk. This lack of context associated with the vignettes
behaviour had been engaged in over the past. has previously been noted as a limitation of the survey (Rae
As mentioned previously, a separate section of the survey et al., 2009).
used in the current study asked respondents about the consid- A third possible explanation for the differences in opinion
erations they use when making decisions about breaching con- demonstrated in the current survey is simply that Australian
fidentiality with adolescent clients. Those findings indicated psychologists do in fact differ in their views about when it is
that an extensive range of considerations are taken into appropriate to breach confidentiality with adolescent clients.
account (Duncan et al., 2012). Similar findings, demonstrating There are many reasons why professional judgements about
that psychologists use a vast range of considerations when when to breach confidentiality might differ. Potential mediators
making such decisions, have also been found in past studies might include age, gender, type of training, number of years
using the same survey (Sullivan & Moyer, 2008). Some of the working as a psychologist, or theoretical orientation. Previous
considerations used by psychologists include: how the family research looking at some of these mediators has found little
would respond if told about the risk behaviour; the adolescent’s evidence for the mediating influence of factors such as gender,
level of competence; workplace policy; the protective factors years of experience, or level of education (Isaacs & Stone, 2001;
present in the adolescent’s life; and whether the adolescent Moyer & Sullivan, 2008). However, it has been shown that
understands why a breach of confidentiality is necessary paediatric psychologists in the USA appear to have a higher
(Duncan et al., 2012). Given this wide variety of contextual tolerance for risk behaviours in adolescent clients (and thus a
factors that are used in the real world of psychological practice, decreased tendency to breach confidentiality) than school psy-
it seems plausible that the absence of detail about such factors chologists in the USA (Rae et al., 2009) indicating that perhaps
in the vignettes presented within the survey might have con- work setting or professional qualification might serve as medi-
tributed to respondents’ failure to reach consensus in response ating factors. Previous literature also highlights the fact that
416 Australian Psychologist 48 (2013) 408–419
© 2012 The Australian Psychological Society
17429544, 2013, 6, Downloaded from https://aps.onlinelibrary.wiley.com/doi/10.1111/ap.12002 by Monash University, Wiley Online Library on [23/04/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
RE Duncan et al. Adolescents, risk behaviour and confidentiality
when psychologists and counsellors are required to rely on their to breach (or not to breach) confidentiality with adolescent
own professional judgements, they are particularly vulnerable clients.
to being influenced by their personal values and beliefs (Moyer
& Sullivan, 2008; Sullivan & Moyer, 2008). Conclusion
If it is the case that the differences in opinion among respond-
ents in the current study reflect not a lack of knowledge and The current study aimed to document the circumstances in
not a lack of contextual detail within the vignettes, but rather which Australian psychologists would breach confidentiality
fundamental differences of opinion, the question that needs to with an adolescent client in order to inform parents about risk
be addressed is, does this matter? If Australian psychologists behaviour. It was more common for respondents to disagree
hold differing opinions about when it is appropriate to breach about whether a breach of confidentiality was necessary than it
confidentiality with adolescent clients, it is likely their practice was for respondents to reach consensus about the need to either
similarly differs. How important is it that psychological practice breach or not breach confidentiality. There are a range of poten-
regarding limits to confidentiality with adolescent clients is con- tial explanations for this. It could mean that Australian psy-
sistent throughout Australia? This is not a question that can be chologists are uncertain about when it is appropriate to breach
answered in this article, but it is one that certainly deserves confidentiality with adolescent clients, or it could mean that a
attention within the Australian psychological profession as a range of mediating factors or contextual details influence opin-
whole. ions. It could also reflect a real and significant variety of opinion
Perhaps the two most important pieces of information currently existing in the Australian psychological profession
provided by the current study are that first, a range of circum- regarding appropriate limits to confidentiality with adolescent
stances exist in which the majority of Australian psychologists clients. If this is the case, the profession must ask itself how
are likely to breach confidentiality with an adolescent client, important consistency of practice is and whether more training
and second, there are a range of scenarios in which practice is and guidance is required in this area. The findings of the current
likely to vary throughout Australia. Both of these findings high- study provide an important empirical resource for professionals
light the same critical fact; that Australian psychologists must to use as a basis for comparison with their own views and
engage in clear and direct communication about their individual practice. The findings also highlight the need for the psychology
limits to confidentiality with adolescent clients and their fami- profession to maintain principles of transparency and informed
lies at the onset of therapy. In this way, the principles of both consent through a commitment to clear communication about
transparency and informed consent are upheld. If clients have the limits to confidentiality at the onset of therapy and through-
been informed of their psychologists’ limits to confidentiality out the therapeutic process.
at the onset of therapy, then, if they disclose information that
requires a breach of confidentiality, they are aware of the likely Acknowledgements
consequences. This need for an initial explanation of the limits
to confidentiality is stipulated in current guidelines internation- Rony Duncan is partly supported through a Fellowship from
ally (American Psychological Association, 2002; Australian the Invergowrie Foundation. This study was supported by the
Psychological Society, 2009; British Psychological Society, 2006; Operational Infrastructure Support Program of the Victorian
Society for Adolescent Medicine, 2004b) and has also been Government.
emphasised by the authors of the American studies that the
current study replicates (Rae et al., 2009). References
The current study should be viewed in light of several limi-
tations. The vignettes presented to respondents all described a American Academy of Paediatrics (2008). Achieving quality health
male adolescent of 15 years of age. Thus, the results do not services for adolescents. Pediatrics, 121, 1263–1270.
necessarily extrapolate to female adolescent clients or adoles- American Medical Association (1993). Confidential health services for
adolescents. JAMA, 269, 1420–1424.
cents of different ages, and we were also not able to test for the
American Medical Association (1994). Code of medical ethics.
impact of client gender on participant responses. In the previous
American Psychological Association (2002). The ethical principles of
study that we replicate here, vignettes of both males and psychologists and code of conduct.
females were used, and there were two conditions in which American School Counselor Association (2004). Ethical standards for
a significant difference was found related to gender. First, school counselors.
respondents were more likely to find it ethical to breach confi- Australian Institute of Health and Welfare (2007). Young Australians:
dentiality for female smoking than they were for male smoking. Their health and wellbeing. Canberra.
Second, they found it more ethical to breach confidentiality for Australian Psychological Society (2007). Code of ethics.
female sexual behaviour than for male sexual behaviour, but Australian Psychological Society (2009). Guidelines for working with
only as the frequency/duration increased. young people.
Australian Psychological Society (2011). Annual report.
The vignettes presented in the current study were also all
Beeman, D. G., & Scott, N. A. (1991). Therapists’ attitudes toward
hypothetical scenarios. Thus, the current study provides no
psychotherapy informed consent with adolescents. Professional
information about what Australian psychologists actually do Psychology Research and Practice, 22, 230–234.
when faced with confidentiality dilemmas about adolescent Berlan, E. D., & Bravender, T. (2009). Confidentiality, consent, and caring
clients, only what they believe they would do. Future research for the adolescent patient. Current Opinion in Pediatrics, 21(4),
seeking to extend the current study might benefit from enquir- 450–456.
ing about actual past cases in which psychologists have chosen British Psychological Society (2006). Code of ethics and conduct.
Australian Psychologist 48 (2013) 408–419 417
© 2012 The Australian Psychological Society
17429544, 2013, 6, Downloaded from https://aps.onlinelibrary.wiley.com/doi/10.1111/ap.12002 by Monash University, Wiley Online Library on [23/04/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
Adolescents, risk behaviour and confidentiality RE Duncan et al.
Collins, N., & Knowles, A. D. (1995). Adolescents’ attitudes toward McGorry, P., Purcell, R., Hickie, I. B., & Jorm, A. F. (2007). Investing in
confidentiality between the school counsellor and the adolescent youth mental health is a best buy. Medical Journal of Australia, 187,
client. Australian Psychologist, 30, 179–182. S5–S7.
Davidson, G. (1995). The ethics of confidentiality: Introduction. Australian McMahon, M., & Knowles, A. (1997). Psychologists’ and psychiatrists’
Psychologist, 30(3), 153–157. perceptions of the dangerous client. Psychiatry, Psychology and Law,
Davis, J. L., & Mickelson, D. J. (1994). School counselors: Are you aware 4, 207–215.
of ethical and legal aspects of counseling? The School Counselor, 42, McMahon, M., & Knowles, A. D. (1995). Confidentiality in psychological
5–13. practice: A decrepit concept? Australian Psychologist, 30(3),
Duncan, R. E., Williams, B., & Knowles, A. (2012). Breaching confidentiality 164–168.
with adolescent clients: a survey of Australian psychologists about the Milne, J. (1995). An analysis of the law of confidentiality with special
considerations that influence their decisions. Psychiatry, Psychology reference to the counselling of minors. Australian Psychologist, 30,
and Law, 19, 209–220. 169–174.
Farrant, B., & Watson, P. D. (2004). Health care delivery: Perspectives of Mitchell, C. W., Disque, J. G., & Robertson, P. (2002). When parents want
young people with chronic illness and their parents. Journal of to know: Responding to parental demands for confidential
Paediatrics and Child Health, 40, 175–179. information. Professional School Counseling, 6, 156–161.
Fisher, M. A. (2008). Protecting confidentiality rights: The need for an Moyer, M. S., & Sullivan, J. (2008). Student risk-taking behaviours: When
ethical practice model. American Psychologist, 63, 1–13. do school counselors break confidentiality? Professional School
Ford, C. A., English, A., & Sigman, G. (2004). Confidential health care for Counseling, 11, 236–245.
adolescents: Position paper for the society for adolescent medicine. Myers, J. E. (1982). Legal issues surrounding psychotherapy with minor
The Journal of Adolescent Health, 35(2), 160–167. clients. Clinical Social Work Journal, 10(4), 303–314.
Ford, C. A., Millstein, S. G., Halpern-Felsher, B. L., & Irwin, C. E. (1997). Pope, K. S., Tabachnick, B. G., & Keith-Spiegel, P. (1988). Good and poor
Influence of physician confidentiality assurances on adolescents’ practices in psychotherapy: A national survey of beliefs of
willingness to disclose information and seek future health care: psychologists. Professional Psychology, 19, 547–552.
A randomised controlled trial. JAMA, 278, 1029–1034. Pope, K. S., & Vetter, V. A. (1992). Ethical dilemmas encountered by
Gustafson, K. E., & McNamara, J. R. (1987). Confidentiality with minor members of the American Psychological Association: A national
clients: Issues and guidelines for therapists. Professional Psychology, survey. The American Psychologist, 47(3), 397–411.
18, 503–508. Rae, W. A., Sullivan, J. R., Razo, N. P., & De Alba, R. G. (2009). Breaking
Haas, L. J., Malouf, J. L., & Mayerson, N. H. (1986). Ethical dilemmas in confidentiality to report adolescent risk-taking behavior by school
psychological practice: Results of a national survey. Professional psychologists. Ethics Behavior, 19, 449–460.
Psychology, 7, 316–321. Rae, W. A., Sullivan, J. R., Razo, N. P., George, C. A., & Ramirez, E. (2002).
Hazen, E., Schlozman, S., & Beresin, E. (2008). Adolescent psychological Adolescent health risk behavior: When do pediatric psychologists
development: A review. Pediatrics in Review, 29, 161–167. break confidentiality? Journal of Pediatric Psychology, 27, 541–549.
Isaacs, M. L., & Stone, C. (1999). School counselors and confidentiality: Reddy, D., Fleming, R., & Swain, C. (2002). Effect of mandatory parental
Factors affecting professional choices. Professional School Counseling, notification on adolescent girls’ use of sexual health care services.
2, 258–266. JAMA, 288, 710–714.
Isaacs, M. L., & Stone, C. (2001). Confidentiality with minors: Mental Sanci, L. A., Sawyer, S. M., Kang, M. S., Haller, D. M., & Patton, G. C.
health counselors’ attitudes toward breaching or preserving (2005). Confidential health care for adolescents: Reconciling clinical
confidentiality. Journal of Mental Health Counseling, 23, evidence with family values. The Medical Journal of Australia, 183,
342–356. 410–414.
Jain, S., & Roberts, L. W. (2009). Ethics in psychotherapy: A focus on Sawyer, S. M., Afifi, R. A., Bearinger, L. H., Blakemore, S.-J., Dick, B.,
professional boundaries and confidentiality practices. Psychiatric Ezeh, A. C., & Patton, G. C. (2012). Adolescence: A foundation for
Clinics of North America, 32, 299–314. future health. The Lancet, 379(9826), 1630–1640.
Jones, R., Purcell, A., Singh, S., & Finer, L. (2005). Adolescents’ reports of Sealander, K. A., Schwiebert, V. L., Oren, T. A., & Weekley, J. L. (1999).
parental knowledge of adolescents’ use of sexual health services and Confidentiality and the law. Professional School Counseling, 3,
their reactions to mandated parental notification for prescription 122–127.
contraception. JAMA, 293(3), 340–348. Sobocinski, M. R. (1990). Ethical principles in the counseling of gay and
Kaczmarek, R. (2000). Ethical and legal complexities inherent in lesbian adolescents: Issues of autonomy, competence, and
professional roles with children and adolescent clients. Counseling confidentiality. Professional Psychology, Research and Practice, 21,
and Human Development, 33, 1–21. 240–247.
Kampf, A., McSherry, B., Thomas, S., & Abrahams, H. (2008). Society for Adolescent Medicine (2004a). Access to health care for
Psychologists’ perceptions of legal and ethical requirements for adolescent and young adults. Journal of Adolescent Health, 35,
breaching confidentiality. Australian Psychologist, 43, 342–344.
194–204. Society for Adolescent Medicine (2004b). Confidential health care for
Kobocow, B., McGuire, J. M., & Blau, B. I. (1983). The influence of adolescents: Position paper of the society for adolescent medicine.
confidentiality conditions on self-disclosure of early adolescents. Journal of Adolescent Health, 35, 160–167.
Professional Psychology, 14, 435–443. Sullivan, J. R., & Moyer, M. S. (2008). Factors influencing the decision to
Lawrence, G., & Kurpius, S. E. (2000). Legal and ethical issues involved break confidentiality with adolescent students: A survey of school
when counseling minors in nonschool settings. Journal of Counseling counselors. Journal of School Counseling. Journal of School
& Development, 78, 130–136. Counseling, 6, n24. Retrieved from http://jsc.montana.edu/
Ledyard, P. (1998). Counselling minors: Ethical and legal issues. articles/v6n24.pdf
Counseling and Values, 42, 171–177. Sullivan, J. R., Ramirez, E., Rae, W. A., Razo, N. P., & George, C. A. (2002).
McCurdy, K. G., & Murray, K. C. (2003). Confidentiality Issues when minor Factors contributing to breaking confidentiality with adolescent
children disclose family secrets in family counseling. The Family clients: A survey of pediatric psychologists. Professional Psychology
Journal, 7, 393–398. 33, 396–401.
418 Australian Psychologist 48 (2013) 408–419
© 2012 The Australian Psychological Society
17429544, 2013, 6, Downloaded from https://aps.onlinelibrary.wiley.com/doi/10.1111/ap.12002 by Monash University, Wiley Online Library on [23/04/2024]. See the Terms and Conditions (https://onlinelibrary.wiley.com/terms-and-conditions) on Wiley Online Library for rules of use; OA articles are governed by the applicable Creative Commons License
RE Duncan et al. Adolescents, risk behaviour and confidentiality
Taylor, L., & Adelman, H. S. (1989). Reframing the confidentiality dilemma adolescent substance use. The Lancet, 369(9570),
to work in children’s best interests. Professional Psychology, 20, 1391–1401.
79–83. Wheeler, R. (2006). Gillick or Fraser? A plea for consistency over
Thrall, J. S., McCloskey, L., Ettner, S. L., Rothman, E., Tighe, J. E., & competence in children. BMJ (Clinical Research Ed.), 332(7545), 807.
Emans, S. J. (2000). Confidentiality and adolescents’ use of providers World Health Organisation (WHO) (2002). Adolescent friendly health
for health information and for pelvic examinations. Archives of services: An agenda for change. Geneva: WHO.
Pediatrics and Adolescent Medicine, 154(9), 885–892. Younggren, J. N., & Harris, E. A. (2008). Can you keep a secret?
Toumbourou, J. W., Stockwell, T., Neighbors, C., Marlatt, G. A., Sturge, J., Confidentiality in psychotherapy. Journal of Clinical Psychology, 64,
& Rehm, J. (2007). Interventions to reduce harm associated with 589–600.
Australian Psychologist 48 (2013) 408–419 419
© 2012 The Australian Psychological Society
You might also like
- The Concept of 'Psychological Safety'Document11 pagesThe Concept of 'Psychological Safety'Dr Suzanne Conboy-HillNo ratings yet
- Black & Decker The Complete Guide To GaragesDocument241 pagesBlack & Decker The Complete Guide To GaragesRade Mladenovic96% (25)
- Energy Sources and Global Warming: Inquiry-Based Lesson PlanDocument5 pagesEnergy Sources and Global Warming: Inquiry-Based Lesson Planapi-546882382No ratings yet
- Ethical Dilemmas of Confidentiality With Adolescent Clients Case Studies From PsychologistsDocument26 pagesEthical Dilemmas of Confidentiality With Adolescent Clients Case Studies From Psychologists7sunqiiNo ratings yet
- Breaching Confidentiality With Adolescent Clients A Survey of Australian Psychologists About The Considerations That Influence Their DecisionsDocument13 pagesBreaching Confidentiality With Adolescent Clients A Survey of Australian Psychologists About The Considerations That Influence Their Decisions7sunqiiNo ratings yet
- Cai DevpsycholDocument19 pagesCai DevpsycholConsu EloNo ratings yet
- Ethics of Neuroimaging in Pediatric Development: Veronica J. HintonDocument14 pagesEthics of Neuroimaging in Pediatric Development: Veronica J. HintonDiane MxNo ratings yet
- Teoria Del Apego y Evaluaciones de TuicionDocument15 pagesTeoria Del Apego y Evaluaciones de TuicionPatricio Ignacio Briceño EcheverríaNo ratings yet
- Bioethics - 2021 - Snoek - Parental Substance and Alcohol Abuse Two Ethical Frameworks To Assess Whether and HowDocument9 pagesBioethics - 2021 - Snoek - Parental Substance and Alcohol Abuse Two Ethical Frameworks To Assess Whether and HowYianni ZaxNo ratings yet
- Analyzing Your Sources Form Name - WRTG 121: Winter 2020Document4 pagesAnalyzing Your Sources Form Name - WRTG 121: Winter 2020Paul WahomeNo ratings yet
- Analyzing Your Sources Form Name - WRTG 121: Winter 2020Document4 pagesAnalyzing Your Sources Form Name - WRTG 121: Winter 2020Paul WahomeNo ratings yet
- IndianJPsychiatry CPG Assessment CAPDocument19 pagesIndianJPsychiatry CPG Assessment CAPGFGFNo ratings yet
- The GP Curriculum and Cerebral PalsyDocument9 pagesThe GP Curriculum and Cerebral PalsyFiaNo ratings yet
- How Can Leaders Influence ASafety CultureDocument11 pagesHow Can Leaders Influence ASafety CultureGustavo Tapia AvendañoNo ratings yet
- Psychol Psychother - 2023 - Kitchen - Barriers and Enablers For Young People Parents and Therapists Undertaking 1Document21 pagesPsychol Psychother - 2023 - Kitchen - Barriers and Enablers For Young People Parents and Therapists Undertaking 1U of T MedicineNo ratings yet
- Gavva Alisa - Annotated Bibliography - CYC347-F2021Document5 pagesGavva Alisa - Annotated Bibliography - CYC347-F2021alisaNo ratings yet
- British J Clinic Psychol - 2022 - Halldorsson - in The Moment Social Experiences and Perceptions of Children With SocialDocument17 pagesBritish J Clinic Psychol - 2022 - Halldorsson - in The Moment Social Experiences and Perceptions of Children With SocialMabel PatiñoNo ratings yet
- IndianJPsychiatry CPG Assessment CAPDocument19 pagesIndianJPsychiatry CPG Assessment CAPMaia MachavarianiNo ratings yet
- Cied Part CDocument2 pagesCied Part Capi-434994955No ratings yet
- UseAttmntTheo AdultPsychotherapyDocument14 pagesUseAttmntTheo AdultPsychotherapyVro AlfrzNo ratings yet
- Ethical and Professional Issues in Clinical PsychologyDocument6 pagesEthical and Professional Issues in Clinical Psychologymughaltalha01249212015No ratings yet
- Coghill Sonuga Barke 2012. Category Vs Dimension in PsychopathologyDocument21 pagesCoghill Sonuga Barke 2012. Category Vs Dimension in PsychopathologyAlexandru NaeNo ratings yet
- Dissertation Ideas Mental Health Social WorkDocument4 pagesDissertation Ideas Mental Health Social WorkPayToDoMyPaperSingapore100% (1)
- Herman 2011Document8 pagesHerman 2011weni astutiNo ratings yet
- Morrish 2018 JhappinessstudiesDocument24 pagesMorrish 2018 Jhappinessstudieseunyoung4819No ratings yet
- Clinicians' Perceptions of The Australian Paediatric Mental Health Service System: Problems and SolutionsDocument12 pagesClinicians' Perceptions of The Australian Paediatric Mental Health Service System: Problems and SolutionsCristianCorreaNo ratings yet
- Designación de Alto Riesgo de Parálisis Cerebral Una Declaración de Consenso ClínicoDocument10 pagesDesignación de Alto Riesgo de Parálisis Cerebral Una Declaración de Consenso ClíniconulintavaNo ratings yet
- Adaptation of The Mental Health Inventory MHI-38 For Adolescents - Indonesian VersionDocument12 pagesAdaptation of The Mental Health Inventory MHI-38 For Adolescents - Indonesian VersionREFIDA MUTIANo ratings yet
- 2011 - Linden - Attitudes of Qualified Vs Student Mental Health Nurses Towards An IndividualDocument10 pages2011 - Linden - Attitudes of Qualified Vs Student Mental Health Nurses Towards An IndividualRonii SzékelyNo ratings yet
- The Adolescent With A Chronic Condition. Part II: Healthcare ProvisionDocument7 pagesThe Adolescent With A Chronic Condition. Part II: Healthcare ProvisionAji Prima PutraNo ratings yet
- Journal - Pone.0290653 1Document26 pagesJournal - Pone.0290653 1U of T MedicineNo ratings yet
- A Learning Theory Approach To Attachment Theory: Exploring Clinical ApplicationsDocument22 pagesA Learning Theory Approach To Attachment Theory: Exploring Clinical ApplicationsCláudioToméNo ratings yet
- Am Headsss 3.0Document12 pagesAm Headsss 3.0Romeo Gian Vincent UrgelNo ratings yet
- Children and Youth Services ReviewDocument11 pagesChildren and Youth Services ReviewNadia Cenat CenutNo ratings yet
- A Cross-Sectional Study On Person-Centred Communication in The Care of Older People: The COMHOME Study ProtocolDocument9 pagesA Cross-Sectional Study On Person-Centred Communication in The Care of Older People: The COMHOME Study Protocolgladeva yugi antariNo ratings yet
- International Journal of Pediatric OtorhinolaryngologyDocument4 pagesInternational Journal of Pediatric Otorhinolaryngologyzaenal abidinNo ratings yet
- Chapter 1 3 ThesisDocument21 pagesChapter 1 3 ThesisJohn Patriarca0% (1)
- Trast Psiq en Niños en El MundoDocument12 pagesTrast Psiq en Niños en El Mundogustavo blancoNo ratings yet
- Journal Pone 0260891Document27 pagesJournal Pone 0260891Andi Nur Rizqi RamadhaniNo ratings yet
- A Prospective Study of The Effects of Optimism OnDocument12 pagesA Prospective Study of The Effects of Optimism OnBareeha AhmedNo ratings yet
- ReindersKrijnen2023Interprof IDandmotivationDocument12 pagesReindersKrijnen2023Interprof IDandmotivationsusi adeNo ratings yet
- Test Bank For Psychiatric Mental Health Nursing 1st Edition by PotterDocument38 pagesTest Bank For Psychiatric Mental Health Nursing 1st Edition by Potterlionelhuynhg7cNo ratings yet
- Microethics The Ethics of Everyday CliniDocument7 pagesMicroethics The Ethics of Everyday ClinimghaseghNo ratings yet
- Dissertation StigmaDocument5 pagesDissertation StigmaBuyACollegePaperCanada100% (1)
- Clinical Psychology - Midterm ReviewerDocument10 pagesClinical Psychology - Midterm ReviewerALEXIS LAROANo ratings yet
- Mako IjgorDocument14 pagesMako IjgorDóra TraxlerNo ratings yet
- Terapia Psicologica Negli AdultiDocument13 pagesTerapia Psicologica Negli Adultigrassochiara14No ratings yet
- Test Bank For Psychiatric Mental Health Nursing 1st Edition by PotterDocument36 pagesTest Bank For Psychiatric Mental Health Nursing 1st Edition by Potterstalder.assapana7ep100% (39)
- Lesson 3Document12 pagesLesson 3Jay Mark CabreraNo ratings yet
- Psychedelic Medicine - Safety and Ethical ConsiderationsDocument2 pagesPsychedelic Medicine - Safety and Ethical ConsiderationsKayla GreenstienNo ratings yet
- Nihms 1647679Document17 pagesNihms 1647679Wiwik sri wahyuniNo ratings yet
- Article JC at 2012Document15 pagesArticle JC at 2012David JoubertNo ratings yet
- Studiu 4Document13 pagesStudiu 4Raluca Zenovia Flocea căs CovaliuNo ratings yet
- 1 Depresion Niños Que Ahora Son AdultosDocument10 pages1 Depresion Niños Que Ahora Son AdultosLuz Maria RojasNo ratings yet
- Evidence Based Support For Autistic People Across TheDocument18 pagesEvidence Based Support For Autistic People Across TheDayna DamianiNo ratings yet
- NSG 436 Benchmark 2 Ethical Dilemma-2Document5 pagesNSG 436 Benchmark 2 Ethical Dilemma-2api-520026903No ratings yet
- Peisah 1999Document12 pagesPeisah 1999cursuriposdruNo ratings yet
- Mental Institution Research PaperDocument4 pagesMental Institution Research Paperixevojrif100% (1)
- Ethical Challenge Scholarly Paper 2Document6 pagesEthical Challenge Scholarly Paper 2api-721737905No ratings yet
- Develop Med Child Neuro - 2009 - WATERS - Quality of Life Instruments For Children and Adolescents With NeurodisabilitiesDocument10 pagesDevelop Med Child Neuro - 2009 - WATERS - Quality of Life Instruments For Children and Adolescents With NeurodisabilitiesCalin PirvaNo ratings yet
- Psychosocial Issues in Pediatric Oncology: Joel Marcus, PsydDocument5 pagesPsychosocial Issues in Pediatric Oncology: Joel Marcus, PsydIlinca RotariuNo ratings yet
- Minnesota Symposia on Child Psychology, Volume 36: The Origins and Organization of Adaptation and MaladaptationFrom EverandMinnesota Symposia on Child Psychology, Volume 36: The Origins and Organization of Adaptation and MaladaptationNo ratings yet
- Actuator Pneumatic Quarter Turn Scotch Yoke Rotork PDFDocument36 pagesActuator Pneumatic Quarter Turn Scotch Yoke Rotork PDFAdi HayyaNo ratings yet
- Market Analysis of Isopropyl AlcoholDocument4 pagesMarket Analysis of Isopropyl AlcoholhasanulfiqryNo ratings yet
- Cyber Security: Threats, Vulnerabilities and Countermeasures - A Perspective On The State of Affairs in MauritiusDocument15 pagesCyber Security: Threats, Vulnerabilities and Countermeasures - A Perspective On The State of Affairs in MauritiusliezelleannNo ratings yet
- 3DS Max Tutorial - The User InterfaceDocument10 pages3DS Max Tutorial - The User InterfaceIDrHotdogNo ratings yet
- Post Ap PDFDocument41 pagesPost Ap PDFMartin Sebastian Gomez GalizziNo ratings yet
- RFC 1337Document13 pagesRFC 1337NickyNETNo ratings yet
- The Stage Management HandbookDocument39 pagesThe Stage Management HandbookAimee HallNo ratings yet
- Huawei Parameter StrategyDocument22 pagesHuawei Parameter StrategyTùng NguyễnNo ratings yet
- Sra Third Party Vendor MGMTDocument11 pagesSra Third Party Vendor MGMTgraeme.mcdonaldNo ratings yet
- 206197-Pirolisis-Biomassa-Kayu-Pinus-Wood-Pine PDFDocument11 pages206197-Pirolisis-Biomassa-Kayu-Pinus-Wood-Pine PDFWahyu AjiNo ratings yet
- Multiple IntelligencesDocument10 pagesMultiple IntelligencesDianne Mojico100% (1)
- The Pros and Cons of Parents' Educational Expectations To The Academic Achievements of Junior High School StudentsDocument198 pagesThe Pros and Cons of Parents' Educational Expectations To The Academic Achievements of Junior High School Studentsyannah kristineNo ratings yet
- Leak Testing ProcedureDocument2 pagesLeak Testing ProcedureVara PrasadNo ratings yet
- Base Station Antenna: 1.4m 6port 3H Antenna With Integrated RCUDocument2 pagesBase Station Antenna: 1.4m 6port 3H Antenna With Integrated RCUДмитрийNo ratings yet
- Red Flags For Unhealthy RelationshipsDocument2 pagesRed Flags For Unhealthy Relationshipskepler8092% (13)
- Trends 2nd Quarter 1Document34 pagesTrends 2nd Quarter 1Fried OilNo ratings yet
- Analysis of To Autumn.Document5 pagesAnalysis of To Autumn.M JaanNo ratings yet
- Mockboard 122 Day 1 Am PP BL Hoa TappDocument23 pagesMockboard 122 Day 1 Am PP BL Hoa TappJHONA THE IGUANANo ratings yet
- Success of Pantaloons Retail India LimitedDocument65 pagesSuccess of Pantaloons Retail India Limitedcoolhunkdelhi67% (3)
- Nuc Entrepreneurship Notes 300 LevelDocument87 pagesNuc Entrepreneurship Notes 300 Level2004sadiqmusaNo ratings yet
- M - 1.6 - Training EvaluationDocument15 pagesM - 1.6 - Training EvaluationLGED ManikganjNo ratings yet
- Poetry 2nd GradeDocument42 pagesPoetry 2nd GradeAnahat MakarandNo ratings yet
- BS 476-7-1997Document24 pagesBS 476-7-1997Ivan ChanNo ratings yet
- Phoenician Settlement, Production, and Trade in Southern AndalucíaDocument22 pagesPhoenician Settlement, Production, and Trade in Southern AndalucíamarwanNo ratings yet
- Study On Mechanical Effect of The Vehicle at Corners: Ming NiDocument4 pagesStudy On Mechanical Effect of The Vehicle at Corners: Ming NiJay SoniNo ratings yet
- Reliance Resq Bhiwadi - Google SearchDocument1 pageReliance Resq Bhiwadi - Google Searchhrshukla092No ratings yet
- Program ListDocument12 pagesProgram ListSoham SealNo ratings yet
- 288112-Article Text-667512-1-10-20231016Document9 pages288112-Article Text-667512-1-10-20231016Al MugishaNo ratings yet