You might also like
- 7 Steps To Discovering Your Personal Values - Scott Jeffrey PDFDocument9 pages7 Steps To Discovering Your Personal Values - Scott Jeffrey PDFtraketeoNo ratings yet
- Basic Guide To Proposal Writing: Step 1: Developing Your Proposal IdeaDocument11 pagesBasic Guide To Proposal Writing: Step 1: Developing Your Proposal Ideanisaralamjan8616100% (2)
- Empowering Parents: AutismDocument10 pagesEmpowering Parents: AutismSuellen Concessio FernandesNo ratings yet
- Concepts of Industrial ManagementDocument9 pagesConcepts of Industrial ManagementSandeep Shrivastava50% (2)
- Role of Feed Additives in Bangladesh Poultry Industries in 2003Document10 pagesRole of Feed Additives in Bangladesh Poultry Industries in 2003Md. Morshed AlamNo ratings yet
- British Thoracic Society Guideline For The Management of Nontuberculous Mycobacterial Pulmonary Disease (NTM-PD) 2017Document13 pagesBritish Thoracic Society Guideline For The Management of Nontuberculous Mycobacterial Pulmonary Disease (NTM-PD) 2017Magaly Esteban GonzalesNo ratings yet
- Auricular Causative Diagnosis-Finding The Roots of Diseases: A Study of Clinical CasesDocument11 pagesAuricular Causative Diagnosis-Finding The Roots of Diseases: A Study of Clinical Casesyan92120No ratings yet
- Book 1Document50 pagesBook 1Varudhini PatkiNo ratings yet
- Journal Pone 0269931Document13 pagesJournal Pone 0269931Abdelali MoufidiNo ratings yet
- Deep Learning-Based Segmentation of Epithelial Ovarian Cancer On T2-Weighted Magnetic Resonance ImagesDocument14 pagesDeep Learning-Based Segmentation of Epithelial Ovarian Cancer On T2-Weighted Magnetic Resonance Imagessukeshini jadhavNo ratings yet
- JPM 11 00515 v2Document25 pagesJPM 11 00515 v2Hasnain Ali ShahNo ratings yet
- Zhai Et Al 2020 Automatic Orbital Computed Tomography Coordinating Method and Quantitative Error Evaluation Based OnDocument6 pagesZhai Et Al 2020 Automatic Orbital Computed Tomography Coordinating Method and Quantitative Error Evaluation Based OnKevin TandartoNo ratings yet
- MiiaDocument10 pagesMiiaCesar Pujay RasecNo ratings yet
- Machine Learning - Based CT Texture Analysis To Predict HPV Status in Oropharyngeal Squamous Cell Carcinoma: Comparison of 2D and 3D SegmentationDocument9 pagesMachine Learning - Based CT Texture Analysis To Predict HPV Status in Oropharyngeal Squamous Cell Carcinoma: Comparison of 2D and 3D Segmentationazul2233No ratings yet
- 1 s2.0 S0001299811000742 MainDocument14 pages1 s2.0 S0001299811000742 Mainkababey111No ratings yet
- An Overview of Artificial Intelligence in Medical Physics and Radiation OncologyDocument11 pagesAn Overview of Artificial Intelligence in Medical Physics and Radiation Oncologyxiwevi4103No ratings yet
- Ultrasound Based Deep Learning Radiomics Nomogram For Risk Stratification of Testicular Masses: A Two Center StudyDocument13 pagesUltrasound Based Deep Learning Radiomics Nomogram For Risk Stratification of Testicular Masses: A Two Center Studybismarck0510No ratings yet
- 2023 A Literature Review On "Lung Cancer Detection Approaches Using Medical Images"Document9 pages2023 A Literature Review On "Lung Cancer Detection Approaches Using Medical Images"graythomasinNo ratings yet
- Applsci 12 08650 v2Document15 pagesApplsci 12 08650 v2Sabir MuhammadNo ratings yet
- Stacked Sparse Autoencoder (SSAE) For Nuclei Detection On Breast Cancer Histopathology ImagesDocument12 pagesStacked Sparse Autoencoder (SSAE) For Nuclei Detection On Breast Cancer Histopathology ImagesSuneetha ChittineniNo ratings yet
- 10 1002@ima 22445Document13 pages10 1002@ima 22445barti koksNo ratings yet
- Lung Cancer Detection and Classification Using Machine Learning AlgorithmDocument7 pagesLung Cancer Detection and Classification Using Machine Learning AlgorithmMadhu C KNo ratings yet
- Pancreas Disease Detection and Segmentation Using Abdominal CT ScanDocument9 pagesPancreas Disease Detection and Segmentation Using Abdominal CT ScanIJAR JOURNALNo ratings yet
- New CNNDocument12 pagesNew CNNMaryam AhmedNo ratings yet
- Guided Soft Attention Network For Classification of Breast Cancer Histopathology ImagesDocument10 pagesGuided Soft Attention Network For Classification of Breast Cancer Histopathology ImagesraniahNo ratings yet
- 05 Ijictv3n9spl PDFDocument6 pages05 Ijictv3n9spl PDFBudi Utami FahnunNo ratings yet
- Quantitative-Analysis CYLINDER DIMENSSIONSDocument5 pagesQuantitative-Analysis CYLINDER DIMENSSIONSp110054No ratings yet
- An Overview of Volumetric Imaging Technologies and Their Quality Assurance For IGRTDocument9 pagesAn Overview of Volumetric Imaging Technologies and Their Quality Assurance For IGRTBounegta AhmedNo ratings yet
- Ritik, Piyush IP Survey PaperDocument7 pagesRitik, Piyush IP Survey PaperGunjan chandwaniNo ratings yet
- Implementation of CT Image Segmentation Based On ADocument11 pagesImplementation of CT Image Segmentation Based On AZAHRA FASKANo ratings yet
- 10 1016@j Bbe 2019 06 003Document11 pages10 1016@j Bbe 2019 06 003HaryadiNo ratings yet
- Qims 12 01 766Document15 pagesQims 12 01 766Hamza ArjahNo ratings yet
- Radiographic Bone Texture Analysis Using Deep Learning Models For Early Rheumatoid Arthritis DiagnosisDocument15 pagesRadiographic Bone Texture Analysis Using Deep Learning Models For Early Rheumatoid Arthritis DiagnosisRaj PanchalNo ratings yet
- 17 J MST 88 2023 131 138 1671Document8 pages17 J MST 88 2023 131 138 1671k3proNo ratings yet
- The Role of Deep Learning and Radiomic FDocument14 pagesThe Role of Deep Learning and Radiomic FuditiNo ratings yet
- 10 1002@jmri 27182 PDFDocument10 pages10 1002@jmri 27182 PDFMădălina MoldovanuNo ratings yet
- Automatic Detection of Tuberculosis Related Abnormalities in Chest X-Ray Images Using Hierarchical FDocument17 pagesAutomatic Detection of Tuberculosis Related Abnormalities in Chest X-Ray Images Using Hierarchical FReadoy RahmanNo ratings yet
- 基于多任务学习的肝细胞癌分割与病理分化程度预测方法 文含Document10 pages基于多任务学习的肝细胞癌分割与病理分化程度预测方法 文含Jack HNo ratings yet
- Development of A Deep-Learning-Based Method For Breast Ultrasound Image SegmentationDocument6 pagesDevelopment of A Deep-Learning-Based Method For Breast Ultrasound Image SegmentationKEREN EVANGELINE I (RA1913011011002)No ratings yet
- Vial 2017Document5 pagesVial 2017Varun RathodNo ratings yet
- Fonc 11 631686Document11 pagesFonc 11 631686pasyaNo ratings yet
- Automated Brain Tumor Detection of MRI Image Based On Hybrid Image Processing TechniquesDocument10 pagesAutomated Brain Tumor Detection of MRI Image Based On Hybrid Image Processing TechniquesTELKOMNIKANo ratings yet
- Segmentation of Vestibular Schwannoma From MRI, An Open Annotated Dataset and Baseline AlgorithmDocument6 pagesSegmentation of Vestibular Schwannoma From MRI, An Open Annotated Dataset and Baseline AlgorithmIndra PrimaNo ratings yet
- Incertidumbres 2Document9 pagesIncertidumbres 2TELLY GONZALO ROMERO BRIOSONo ratings yet
- Cell Cluster Graph For Prediction of Biochemical Recurrence in Prostate Cancer Patients From Tissue MicroarraysDocument11 pagesCell Cluster Graph For Prediction of Biochemical Recurrence in Prostate Cancer Patients From Tissue MicroarraysFrontiersNo ratings yet
- 11.deep Learning Applications in Medical Image Analysis-Brain TumorDocument4 pages11.deep Learning Applications in Medical Image Analysis-Brain TumorVenky Naidu BalineniNo ratings yet
- Haga 2017Document9 pagesHaga 2017tsania nkdNo ratings yet
- Prostate Segmentation ThesisDocument9 pagesProstate Segmentation Thesisgj9ggjry100% (2)
- Pi Is 2452109422001488Document10 pagesPi Is 2452109422001488Raul Matute MartinNo ratings yet
- Review Bio Medical ImagingDocument23 pagesReview Bio Medical ImagingSweta TripathiNo ratings yet
- ReportDocument18 pagesReportEshwarNo ratings yet
- Applied Sciences: Deep Learning-Based Automatic Segmentation of Mandible and Maxilla in Multi-Center CT ImagesDocument15 pagesApplied Sciences: Deep Learning-Based Automatic Segmentation of Mandible and Maxilla in Multi-Center CT ImagesDyah Dhani MustikariniNo ratings yet
- Lung Tumor Localization and Visualization in ChestDocument17 pagesLung Tumor Localization and Visualization in ChestAida Fitriyane HamdaniNo ratings yet
- Artificial Neural Network For Cervical Abnormalities Detection On Computed Tomography ImagesDocument9 pagesArtificial Neural Network For Cervical Abnormalities Detection On Computed Tomography ImagesIAES IJAINo ratings yet
- PravallikaDocument28 pagesPravallikaVegesana SumythriNo ratings yet
- Transfer LearningDocument7 pagesTransfer LearningAdah EneNo ratings yet
- Automatic Tool Segmentation and Tracking During Robotic Intravascular Catheterization For Cardiac InterventionsDocument23 pagesAutomatic Tool Segmentation and Tracking During Robotic Intravascular Catheterization For Cardiac InterventionsNishant UzirNo ratings yet
- Kidney and Tumor Segmentation Using Combined Deep Learning MethodDocument11 pagesKidney and Tumor Segmentation Using Combined Deep Learning MethodegamrNo ratings yet
- Lung Tumor Diagnosis System Using Whale Optimization and SVMDocument11 pagesLung Tumor Diagnosis System Using Whale Optimization and SVMDr Mohammed KamalNo ratings yet
- Deep Learning Methods To Generate Synthetic CT From MRI in Radiotherapy A Literature ReviewDocument17 pagesDeep Learning Methods To Generate Synthetic CT From MRI in Radiotherapy A Literature ReviewColman SiuNo ratings yet
- Cancers 13 00661 v2Document14 pagesCancers 13 00661 v2seyfu mogesNo ratings yet
- Encoder Decoder With Dense Dilated Spatial Pyramid Pooling For Prostate MRDocument8 pagesEncoder Decoder With Dense Dilated Spatial Pyramid Pooling For Prostate MRSatyaNurAnggaNo ratings yet
- Two Path Gland Segmentation Algorithm of Colon Pathological Image Based On Local Semantic GuidanceDocument8 pagesTwo Path Gland Segmentation Algorithm of Colon Pathological Image Based On Local Semantic GuidancejamesraiaanNo ratings yet
- Qin 2018Document5 pagesQin 2018sadNo ratings yet
- T2 NanthagopalDocument10 pagesT2 NanthagopalbelajartvkuNo ratings yet
- Reducing The Model Variance of A Rectal Cancer Segmentation NetworkDocument9 pagesReducing The Model Variance of A Rectal Cancer Segmentation NetworkDiego Marcelino Santos SilvaNo ratings yet
- The Effects of Essence-Formed Cosmetic Ingredients Containing The GalactomycesDocument8 pagesThe Effects of Essence-Formed Cosmetic Ingredients Containing The GalactomycesLwsynergylab OfficialNo ratings yet
- Nota Bene For My ReviewersDocument4 pagesNota Bene For My ReviewersYomadoNo ratings yet
- Neonatology Short Case History Taking Format by SPKathankar 1Document5 pagesNeonatology Short Case History Taking Format by SPKathankar 1HkNo ratings yet
- TGI0221 FinalDocument81 pagesTGI0221 FinalInes NarcisoNo ratings yet
- Carbohydrate Mcas Questions 1 2015Document3 pagesCarbohydrate Mcas Questions 1 2015api-263230840No ratings yet
- Nursing Core Competencies For Quality LevelDocument5 pagesNursing Core Competencies For Quality Leveljava_biscocho1229No ratings yet
- Department of Education: Directions: Choose The Letter of The Correct AnswerDocument2 pagesDepartment of Education: Directions: Choose The Letter of The Correct AnswerMelitado WengNo ratings yet
- Research PaperDocument4 pagesResearch Paperapi-611611708No ratings yet
- Mediclear: Site Office - 90, Vasant Complex, Mayur Vihar, DelhiDocument3 pagesMediclear: Site Office - 90, Vasant Complex, Mayur Vihar, Delhiafsarkhan85No ratings yet
- What Do We Know About The Food We Eat?: Teaching and Learning Activities, Including Assessment OpportunitiesDocument14 pagesWhat Do We Know About The Food We Eat?: Teaching and Learning Activities, Including Assessment OpportunitiesaravindyellowNo ratings yet
- Teva AR 2017 - PharmaceuticalIndustriesLtdDocument805 pagesTeva AR 2017 - PharmaceuticalIndustriesLtdBhushanNo ratings yet
- Digi T Vigilance TestDocument6 pagesDigi T Vigilance TestJillianne FrancoNo ratings yet
- Bahasa Inggris UTS Kelas 5 SMT 2Document5 pagesBahasa Inggris UTS Kelas 5 SMT 2Aulia Laily MaulindaNo ratings yet
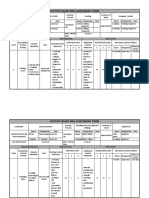
- Activity-Based Risk Assessment Form: Wearing InspectorDocument3 pagesActivity-Based Risk Assessment Form: Wearing InspectorSherly MagatNo ratings yet
- Formula, Good or Not For The Babies ?: Written By: Rakhmah Sari Indah C. - XII P7 /28Document4 pagesFormula, Good or Not For The Babies ?: Written By: Rakhmah Sari Indah C. - XII P7 /28Inda KecilNo ratings yet
- ListeningDocument7 pagesListeningPallavi JNo ratings yet
- Data Peserta Gartheting LT 3aumst Final 2022Document11 pagesData Peserta Gartheting LT 3aumst Final 2022Doni IrawanNo ratings yet
- CARE EMB Brief 1 - WebDocument5 pagesCARE EMB Brief 1 - WebbeckianoNo ratings yet
- Synerquest 2014 Annual Calendar of DOLE-prescribed CoursesDocument3 pagesSynerquest 2014 Annual Calendar of DOLE-prescribed CoursesrobinrubinaNo ratings yet
- Effectiveness and Neural Mechanisms of Home-BasedDocument5 pagesEffectiveness and Neural Mechanisms of Home-BasedMuhammad ImronNo ratings yet
- DecomposingDocument2 pagesDecomposingapi-254428474100% (1)
- BIOBASE SCSJ-V Series User ManualDocument25 pagesBIOBASE SCSJ-V Series User Manualsoporte03No ratings yet