You might also like
- 05 Nov User Manual Bxs Elevators PDFDocument108 pages05 Nov User Manual Bxs Elevators PDFEdi Piñeros JaimesNo ratings yet
- MINI CVT 040930 MapDocument1 pageMINI CVT 040930 MapBivolaru Teodor MarianNo ratings yet
- Catalog Winker SemiremorciDocument62 pagesCatalog Winker SemiremorciRusu Alina IoanaNo ratings yet
- SWVLDocument9 pagesSWVLSohaib SyedNo ratings yet
- Streetscapes PompeiiDocument20 pagesStreetscapes PompeiiSonika PatelNo ratings yet
- Gravure Printing Atoz 2013 PDFDocument59 pagesGravure Printing Atoz 2013 PDFAlmir Machado0% (1)
- Assignment 3 Mode Choice ModelsDocument4 pagesAssignment 3 Mode Choice ModelsSesay Alieu100% (2)
- IMCASF - Mar 18Document3 pagesIMCASF - Mar 18Shivkumar JadhavNo ratings yet
- IMCA Safety Flash 09/19Document4 pagesIMCA Safety Flash 09/19Harman SandhuNo ratings yet
- IMCASF - Apr 16Document6 pagesIMCASF - Apr 16Shivkumar JadhavNo ratings yet
- IMCASF - Apr 17 (12Document5 pagesIMCASF - Apr 17 (12Shivkumar JadhavNo ratings yet
- IMCA Safety Flash 19/20: 1 Fall From A Height Into A Ballast TankDocument6 pagesIMCA Safety Flash 19/20: 1 Fall From A Height Into A Ballast TankGianluca PiccinettiNo ratings yet
- IMCASF - Nov 16Document4 pagesIMCASF - Nov 16Shivkumar JadhavNo ratings yet
- IMCASF - Oct 17Document6 pagesIMCASF - Oct 17Shivkumar JadhavNo ratings yet
- IMCASF - Jun 18Document4 pagesIMCASF - Jun 18Shivkumar JadhavNo ratings yet
- Imcasf 14 20 PDFDocument6 pagesImcasf 14 20 PDFsameer hiiNo ratings yet
- IMCASF - Apr 16Document3 pagesIMCASF - Apr 16Shivkumar JadhavNo ratings yet
- IMCASF - Jun 17Document5 pagesIMCASF - Jun 17Shivkumar JadhavNo ratings yet
- IMCASF - Feb 19Document6 pagesIMCASF - Feb 19Shivkumar JadhavNo ratings yet
- IMCASF - Jul 16Document4 pagesIMCASF - Jul 16Shivkumar JadhavNo ratings yet
- IMCASF - Jan 18Document5 pagesIMCASF - Jan 18Shivkumar JadhavNo ratings yet
- Imcasf 22 19Document5 pagesImcasf 22 19Pippo TopolinoNo ratings yet
- IMCASF - Sept 17Document4 pagesIMCASF - Sept 17Shivkumar JadhavNo ratings yet
- IMCASF - Oct 16Document8 pagesIMCASF - Oct 16Shivkumar JadhavNo ratings yet
- IMCASF - May 16Document5 pagesIMCASF - May 16Shivkumar JadhavNo ratings yet
- IMCASF - Aug 17Document7 pagesIMCASF - Aug 17Shivkumar JadhavNo ratings yet
- IMCASF - July 19Document5 pagesIMCASF - July 19Shivkumar JadhavNo ratings yet
- IMCASF - Oct 16Document4 pagesIMCASF - Oct 16Shivkumar JadhavNo ratings yet
- IMCASF - Mar 16Document4 pagesIMCASF - Mar 16Shivkumar JadhavNo ratings yet
- IMCASF - Sept 16Document7 pagesIMCASF - Sept 16Shivkumar JadhavNo ratings yet
- Imcasf20 18Document6 pagesImcasf20 18Era ErmerraNo ratings yet
- IMCASF - Oct 18Document6 pagesIMCASF - Oct 18Shivkumar JadhavNo ratings yet
- IMCASF - Sept 20Document6 pagesIMCASF - Sept 20Shivkumar JadhavNo ratings yet
- IMCASF - Oct 17Document6 pagesIMCASF - Oct 17Shivkumar JadhavNo ratings yet
- IMCASF - Jul 17Document6 pagesIMCASF - Jul 17Shivkumar JadhavNo ratings yet
- IMCASF - Jan 16Document6 pagesIMCASF - Jan 16Shivkumar JadhavNo ratings yet
- IMCASF - Nov 16Document7 pagesIMCASF - Nov 16Shivkumar JadhavNo ratings yet
- IMCASF - Oct 18Document5 pagesIMCASF - Oct 18Shivkumar JadhavNo ratings yet
- IMCASF - May 16Document2 pagesIMCASF - May 16Shivkumar JadhavNo ratings yet
- IMCASF - Oct 16Document5 pagesIMCASF - Oct 16Shivkumar JadhavNo ratings yet
- IMCASF - Jul 16Document4 pagesIMCASF - Jul 16Shivkumar JadhavNo ratings yet
- IMCASF - Nov 18Document5 pagesIMCASF - Nov 18Shivkumar JadhavNo ratings yet
- IMCASF - Jun 18Document5 pagesIMCASF - Jun 18Shivkumar JadhavNo ratings yet
- IMCASF - Oct 17Document8 pagesIMCASF - Oct 17Shivkumar JadhavNo ratings yet
- IMCASF - Dec 18Document5 pagesIMCASF - Dec 18Shivkumar JadhavNo ratings yet
- IMCASF - Dec 17Document6 pagesIMCASF - Dec 17Shivkumar JadhavNo ratings yet
- IMCASF - Jan 17Document2 pagesIMCASF - Jan 17Shivkumar JadhavNo ratings yet
- IMCASF - Jun 18Document5 pagesIMCASF - Jun 18Shivkumar JadhavNo ratings yet
- IMCASF - Dec 17Document4 pagesIMCASF - Dec 17Shivkumar JadhavNo ratings yet
- IMCASF - May 20Document6 pagesIMCASF - May 20Shivkumar JadhavNo ratings yet
- IMCASF - Jul 17Document7 pagesIMCASF - Jul 17Shivkumar JadhavNo ratings yet
- Title 1Document21 pagesTitle 1Muhd QaiyumNo ratings yet
- SF 22 23Document6 pagesSF 22 23Shivkumar JadhavNo ratings yet
- SF 19 22Document6 pagesSF 19 22Shivkumar JadhavNo ratings yet
- IMCASF - Dec 16Document6 pagesIMCASF - Dec 16Shivkumar JadhavNo ratings yet
- IMCASF - Mar 18Document5 pagesIMCASF - Mar 18Shivkumar JadhavNo ratings yet
- IMCASF - Jan 18Document5 pagesIMCASF - Jan 18Shivkumar JadhavNo ratings yet
- Imcasf 10 18Document6 pagesImcasf 10 18Shola EshoNo ratings yet
- IMCASF - Oct 16Document6 pagesIMCASF - Oct 16Shivkumar JadhavNo ratings yet
- IMCASF - Sept 20Document6 pagesIMCASF - Sept 20Shivkumar JadhavNo ratings yet
- IMCASF - Feb 16Document7 pagesIMCASF - Feb 16Shivkumar JadhavNo ratings yet
- IMCASF - Feb 17Document3 pagesIMCASF - Feb 17Shivkumar JadhavNo ratings yet
- SF 27 22Document5 pagesSF 27 22Shivkumar JadhavNo ratings yet
- IMCASF - Aug 19Document6 pagesIMCASF - Aug 19Shivkumar JadhavNo ratings yet
- Imcasf21 18Document6 pagesImcasf21 18Era ErmerraNo ratings yet
- IMCA Safety Flashes 2009 07Document6 pagesIMCA Safety Flashes 2009 07Francisco TajúNo ratings yet
- IMCASF - Oct 18Document5 pagesIMCASF - Oct 18Shivkumar JadhavNo ratings yet
- IMCASF - Jul 18Document6 pagesIMCASF - Jul 18Shivkumar JadhavNo ratings yet
- IMCASF - Jan 17Document7 pagesIMCASF - Jan 17Shivkumar JadhavNo ratings yet
- IMCASF - Mar 17Document5 pagesIMCASF - Mar 17Shivkumar JadhavNo ratings yet
- IMCASF - Mar 18Document4 pagesIMCASF - Mar 18Shivkumar JadhavNo ratings yet
- IMCASF - Jan 17Document2 pagesIMCASF - Jan 17Shivkumar JadhavNo ratings yet
- IMCASF - Mar 17Document6 pagesIMCASF - Mar 17Shivkumar JadhavNo ratings yet
- IMCASF - Jul 17Document6 pagesIMCASF - Jul 17Shivkumar JadhavNo ratings yet
- IMCASF - May 17Document7 pagesIMCASF - May 17Shivkumar JadhavNo ratings yet
- IMCASF - Jun 17Document5 pagesIMCASF - Jun 17Shivkumar JadhavNo ratings yet
- IMCASF - Oct 16Document4 pagesIMCASF - Oct 16Shivkumar JadhavNo ratings yet
- IMCASF - Feb 17Document3 pagesIMCASF - Feb 17Shivkumar JadhavNo ratings yet
- IMCASF - Nov 16Document4 pagesIMCASF - Nov 16Shivkumar JadhavNo ratings yet
- IMCASF - Nov 16Document4 pagesIMCASF - Nov 16Shivkumar JadhavNo ratings yet
- IMCASF - Jun 17Document6 pagesIMCASF - Jun 17Shivkumar JadhavNo ratings yet
- IMCASF - Oct 16Document2 pagesIMCASF - Oct 16Shivkumar JadhavNo ratings yet
- IMCASF - Apr 16Document3 pagesIMCASF - Apr 16Shivkumar JadhavNo ratings yet
- IMCASF - Oct 16Document6 pagesIMCASF - Oct 16Shivkumar JadhavNo ratings yet
- IMCASF - Aug 16Document10 pagesIMCASF - Aug 16Shivkumar JadhavNo ratings yet
- SF 02 24Document6 pagesSF 02 24Shivkumar JadhavNo ratings yet
- IMCASF - May 20Document3 pagesIMCASF - May 20Shivkumar JadhavNo ratings yet
- SF 22 23Document6 pagesSF 22 23Shivkumar JadhavNo ratings yet
- IMCASF - May 20Document6 pagesIMCASF - May 20Shivkumar JadhavNo ratings yet
- SF 07 24Document6 pagesSF 07 24Shivkumar JadhavNo ratings yet
- SF 04 24Document6 pagesSF 04 24Shivkumar JadhavNo ratings yet
- SF 27 23Document6 pagesSF 27 23Shivkumar JadhavNo ratings yet
- SF 28 23Document8 pagesSF 28 23Shivkumar JadhavNo ratings yet
- SF 16 23Document6 pagesSF 16 23Shivkumar JadhavNo ratings yet
- How Does A Gas Turbine Power Plant Work?: 1. CompressorDocument8 pagesHow Does A Gas Turbine Power Plant Work?: 1. CompressorSuresh Ram R100% (1)
- Project Proposal Bat-Ongan JanmarkDocument5 pagesProject Proposal Bat-Ongan JanmarkJanmark MarquezNo ratings yet
- Continuous Synopsis Record (CSR)Document2 pagesContinuous Synopsis Record (CSR)mustaffa bakriNo ratings yet
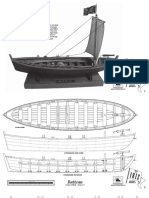
- Ba Eau: 1/24 SCALE MODEL 1/2" 1'-0"Document11 pagesBa Eau: 1/24 SCALE MODEL 1/2" 1'-0"Gassab MohamedNo ratings yet
- 1950 24 Hours of Le MansDocument132 pages1950 24 Hours of Le MansPaoloViarengoNo ratings yet
- Sailor 60, 90 Satellite TV: Built For Maritime ProfessionalsDocument2 pagesSailor 60, 90 Satellite TV: Built For Maritime ProfessionalsAdamNo ratings yet
- Police Log November 23, 2015Document12 pagesPolice Log November 23, 2015MansfieldMAPoliceNo ratings yet
- Rules For Classification and Construction VI Additional Rules and GuidelinesDocument34 pagesRules For Classification and Construction VI Additional Rules and Guidelineshapcyu05No ratings yet
- Mounting Systems For Solar TechnologyDocument24 pagesMounting Systems For Solar TechnologyEngineering SESNANo ratings yet
- ISUZU Spear Part ListDocument6 pagesISUZU Spear Part ListtolgaNo ratings yet
- HDP e Drainage Products Brochure 10222114Document20 pagesHDP e Drainage Products Brochure 10222114realchicNo ratings yet
- Year End 2023 Tourism Measures 1Document33 pagesYear End 2023 Tourism Measures 1Anonymous UpWci5No ratings yet
- Cebu PacificDocument4 pagesCebu PacificPrecious Love Santillan NicomedesNo ratings yet
- Asking For and Giving DirectionsDocument7 pagesAsking For and Giving Directionsandreia silverioNo ratings yet
- 4 SignsDocument3 pages4 SignsJonathan GonzalezNo ratings yet
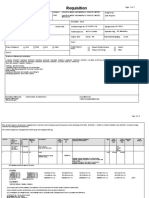
- Req. 607614 - 531.DU911 - VER 2Document2 pagesReq. 607614 - 531.DU911 - VER 2JCSNo ratings yet
- Car Insurance IrelandDocument4 pagesCar Insurance IrelandDavidNo ratings yet
- hsg177 - Managing Health and Safety in DockworkDocument29 pageshsg177 - Managing Health and Safety in Dockworkchelios2No ratings yet
- Øresund BridgeDocument12 pagesØresund BridgeHaziq Fadli ZiqReenNo ratings yet
- İngDocument14 pagesİngBeyza ÇiftçiNo ratings yet
- DLF Siruseri Plots in Parc Estate ChennaiDocument31 pagesDLF Siruseri Plots in Parc Estate ChennaiLuxe HabitatNo ratings yet