You might also like
- Distant Force A Memoir of The Teledyne Corporation and The Man Who Created It With An IntroDocument20 pagesDistant Force A Memoir of The Teledyne Corporation and The Man Who Created It With An Introgauravpassion0% (1)
- Review: Autism Spectrum Disorder: Advances in Evidence-Based PracticeDocument11 pagesReview: Autism Spectrum Disorder: Advances in Evidence-Based PracticeWafaNo ratings yet
- Potential Conflicts of Interest: 2012 American Neurological Association 983Document2 pagesPotential Conflicts of Interest: 2012 American Neurological Association 983Khuen Yen NgNo ratings yet
- Practica Basada en Lae Evidencia TEADocument11 pagesPractica Basada en Lae Evidencia TEAdadamianiNo ratings yet
- 01 s2.0 S0925443910002954 MainDocument8 pages01 s2.0 S0925443910002954 MainAthena DiggoryNo ratings yet
- 1 s2.0 S1071909120300401 MainDocument10 pages1 s2.0 S1071909120300401 MainMónica Álvarez CórdobaNo ratings yet
- Wik 2Document9 pagesWik 2Debiani WulandariNo ratings yet
- Psychiatry Clin Neurosci - 2017 - Waye - Genetics and Epigenetics of Autism A ReviewDocument17 pagesPsychiatry Clin Neurosci - 2017 - Waye - Genetics and Epigenetics of Autism A ReviewKaline DantasNo ratings yet
- An Etiologic Classification of Autism Spectrum Disorders: Lidia V. Gabis MD and John Pomeroy MDDocument4 pagesAn Etiologic Classification of Autism Spectrum Disorders: Lidia V. Gabis MD and John Pomeroy MDCarlos Charlotte SalvadorNo ratings yet
- Neurobiological Context of AutizmDocument22 pagesNeurobiological Context of AutizmGerasim HarutyunyanNo ratings yet
- Encef Peds PDFDocument11 pagesEncef Peds PDFNicolas TovarNo ratings yet
- lukmanji2019 الصرعDocument11 pageslukmanji2019 الصرعkhadidja BOUTOUILNo ratings yet
- Jurnal AdhdDocument38 pagesJurnal AdhdbimoNo ratings yet
- Diagnostic Exome Sequencing in Persons With Severe Intellectual DisabilityDocument9 pagesDiagnostic Exome Sequencing in Persons With Severe Intellectual DisabilityMiaNo ratings yet
- Robinson2012 Article ChildhoodEpilepsyAndAutismSpecDocument9 pagesRobinson2012 Article ChildhoodEpilepsyAndAutismSpecTheo KhouryNo ratings yet
- Perinatalni I Prenatalni Uzroci AutizmaDocument8 pagesPerinatalni I Prenatalni Uzroci AutizmaJohn SmithNo ratings yet
- Dandy-Walker Syndrome Patients - GREEN AAMDocument35 pagesDandy-Walker Syndrome Patients - GREEN AAMdonilord19No ratings yet
- Fneur 2018 00670Document4 pagesFneur 2018 00670SASIKUMAR SNo ratings yet
- AutismDocument32 pagesAutismadaainNo ratings yet
- Analysis and Evaluation of ASD TheoriesDocument9 pagesAnalysis and Evaluation of ASD Theoriestracycw100% (1)
- Prevalence of Tourette Syndrome and Chronic Tics I PDFDocument16 pagesPrevalence of Tourette Syndrome and Chronic Tics I PDFFitriazneNo ratings yet
- Epilepsy in Patients With Autism: Links, Risks and Treatment ChallengesDocument10 pagesEpilepsy in Patients With Autism: Links, Risks and Treatment ChallengesDiana NaNo ratings yet
- Cerebellar and Striatal Implications in Autism Spectrum Disorders: From Clinical Observations To Animal ModelsDocument33 pagesCerebellar and Striatal Implications in Autism Spectrum Disorders: From Clinical Observations To Animal ModelsurosNo ratings yet
- Incidence and Prevalence of Childhood Epilepsy: A Nationwide Cohort StudyDocument11 pagesIncidence and Prevalence of Childhood Epilepsy: A Nationwide Cohort StudyasfwegereNo ratings yet
- Practice Guideline Summary: Sudden Unexpected Death in Epilepsy Incidence Rates and Risk FactorsDocument10 pagesPractice Guideline Summary: Sudden Unexpected Death in Epilepsy Incidence Rates and Risk FactorsB NadyaNo ratings yet
- E472 FullDocument17 pagesE472 FullC_DanteNo ratings yet
- 1456 FullDocument7 pages1456 Fulldrmanishmahajan79No ratings yet
- Neuro J 1Document11 pagesNeuro J 1Anonymous CtjSRA4No ratings yet
- Autismo EgiptoDocument8 pagesAutismo EgiptoOvsd Vfsg SDNo ratings yet
- The American Academy of Pediatrics, 141 Northwest Point BLVD., Elk Grove Village, IL 60007Document34 pagesThe American Academy of Pediatrics, 141 Northwest Point BLVD., Elk Grove Village, IL 60007neuropedNo ratings yet
- Autism: DefinitionDocument6 pagesAutism: DefinitionBallave SudiptaNo ratings yet
- NIH Public Access: Author ManuscriptDocument25 pagesNIH Public Access: Author ManuscriptRominaNo ratings yet
- Prader WilliDocument15 pagesPrader WilliGVHHNo ratings yet
- 30 Scientific Studies That Demonstrate Vaccines Can Cause AutismDocument23 pages30 Scientific Studies That Demonstrate Vaccines Can Cause Autismazrulelias100% (6)
- Paulea - Rowlandb.fergusona - Chelonisc.tannockd - Swansone.castellanos. ADHD Characteristics Interventions ModelsDocument21 pagesPaulea - Rowlandb.fergusona - Chelonisc.tannockd - Swansone.castellanos. ADHD Characteristics Interventions ModelsRute Almeida RomãoNo ratings yet
- Research Paper On AutismDocument11 pagesResearch Paper On Autismapi-529885888No ratings yet
- Epidemiology and Initial Management of Ambiguous Genitalia at Birth in GermanyDocument9 pagesEpidemiology and Initial Management of Ambiguous Genitalia at Birth in GermanyFikri Abd AzisNo ratings yet
- Chapter 8 - Autism Spectrum Disorder - 2018 - Integrative MedicineDocument14 pagesChapter 8 - Autism Spectrum Disorder - 2018 - Integrative MedicineandreNo ratings yet
- Autism Spectrum DisorderDocument4 pagesAutism Spectrum DisorderParishna BhuyanNo ratings yet
- Autism-Spectrum-Disorders-an-Intervention-Approach LAO JIDocument12 pagesAutism-Spectrum-Disorders-an-Intervention-Approach LAO JIErica Alejandra SchumacherNo ratings yet
- Autism Spectrum DisordersDocument6 pagesAutism Spectrum DisordersHans HorstNo ratings yet
- Nihms 460725Document18 pagesNihms 460725urosNo ratings yet
- ALSDocument14 pagesALSZé CunhaNo ratings yet
- Alzheimer's - Alzheimer's Disease - Kaj Blennow, Mony J de Leon, Henrik ZeterbergDocument17 pagesAlzheimer's - Alzheimer's Disease - Kaj Blennow, Mony J de Leon, Henrik ZeterbergCatinean DanielaNo ratings yet
- Utility of Neurodiagnostic Studies in The Diagnosis of Autoimmune Encephalitis in PDFDocument26 pagesUtility of Neurodiagnostic Studies in The Diagnosis of Autoimmune Encephalitis in PDFMaverick 18No ratings yet
- Environmental Risk Factors and Biomarkers For Autism Spectrum Disorder: An Umbrella Review of The EvidenceDocument11 pagesEnvironmental Risk Factors and Biomarkers For Autism Spectrum Disorder: An Umbrella Review of The EvidenceLaurenLuodiYuNo ratings yet
- Autism and EpilepsyDocument5 pagesAutism and Epilepsyclarajimena25No ratings yet
- Genetic Advances in Autism - Heterogeneity and Convergence On Shared PathwaysDocument12 pagesGenetic Advances in Autism - Heterogeneity and Convergence On Shared PathwaysDaniela SalazarNo ratings yet
- Relation Between Increased Frequency of Serum Antineuronal Antibodies Abd The Severity of AutismDocument5 pagesRelation Between Increased Frequency of Serum Antineuronal Antibodies Abd The Severity of AutismAchref HoussamNo ratings yet
- Trends in Neuroscience and EducationDocument4 pagesTrends in Neuroscience and EducationNielsen ValeNo ratings yet
- 2017 Examining The Causes of AutismDocument12 pages2017 Examining The Causes of AutismrimaNo ratings yet
- Alzheimers Disease Research Paper ThesisDocument6 pagesAlzheimers Disease Research Paper Thesisgw0pajg4100% (1)
- Sample Paper For FormatDocument8 pagesSample Paper For FormatTiffanyNo ratings yet
- Neonatal Encephalopathy: Need For Recognition of Multiple Etiologies For Optimal ManagementDocument7 pagesNeonatal Encephalopathy: Need For Recognition of Multiple Etiologies For Optimal ManagementDiana De La CruzNo ratings yet
- Autism Spectrum Disorder - A Case Study of MikeyDocument25 pagesAutism Spectrum Disorder - A Case Study of MikeyMuhammad FadhilNo ratings yet
- Nfluenza-Associated Encephalitis Encephalopathy Identified by The Australian Childhood Encephalitis Study 2013-2015.Document6 pagesNfluenza-Associated Encephalitis Encephalopathy Identified by The Australian Childhood Encephalitis Study 2013-2015.zhoujNo ratings yet
- A Case Report of Obsessive-Compulsive DisorderDocument6 pagesA Case Report of Obsessive-Compulsive DisorderfonsoalNo ratings yet
- A View of Ayurveda On Autism Spectrum DisordersDocument9 pagesA View of Ayurveda On Autism Spectrum DisordersgrspavaniNo ratings yet
- Causes of AutismDocument10 pagesCauses of AutismnourNo ratings yet
- Running Head: Autism: The Complicated Truths 1Document11 pagesRunning Head: Autism: The Complicated Truths 1Leon Hersch GonzalezNo ratings yet
- Unit 5 Corporate Mission, Objectives and Responsibility: StructureDocument30 pagesUnit 5 Corporate Mission, Objectives and Responsibility: StructureRadhika KidambiNo ratings yet
- Escrow Rbi RulesDocument2 pagesEscrow Rbi RulesAtiqur Rahman BarbhuiyaNo ratings yet
- Marketing Plan For Madge Café: Caro, Marie Joy Casiple, Koleen Estebal, Honey Faye Longno, JosieDocument15 pagesMarketing Plan For Madge Café: Caro, Marie Joy Casiple, Koleen Estebal, Honey Faye Longno, JosieJoyNo ratings yet
- NH Field Guide For Residential New Construction - 2011Document88 pagesNH Field Guide For Residential New Construction - 2011Nh Energy CodeNo ratings yet
- Unit 01: Systems Analysis and DesignDocument15 pagesUnit 01: Systems Analysis and Designwendle vidwanNo ratings yet
- The 108 Star Bearers in The Suikoden TierkiesDocument51 pagesThe 108 Star Bearers in The Suikoden TierkiesEkky Maretha PrathiwiNo ratings yet
- Module 2-Introduction To Chemistry (Week 2)Document3 pagesModule 2-Introduction To Chemistry (Week 2)Ian ParoneNo ratings yet
- CD74HCT4052, CD54/74HC4053, CD54/74HC54053 High-Speed Cmos Logic Analog Multiplexers/DemultiplexersDocument34 pagesCD74HCT4052, CD54/74HC4053, CD54/74HC54053 High-Speed Cmos Logic Analog Multiplexers/DemultiplexersAndrea DispoNo ratings yet
- New Organized Crime Handbook 2 - Mam SallyDocument57 pagesNew Organized Crime Handbook 2 - Mam SallycaspherNo ratings yet
- Lecture 2 - Project ManagementDocument30 pagesLecture 2 - Project ManagementktubdaNo ratings yet
- Metal Cutting PDFDocument92 pagesMetal Cutting PDFJagadishchandrabose KondamudiNo ratings yet
- Ii. Functions: Trust?Document6 pagesIi. Functions: Trust?Jeffrey Garcia IlaganNo ratings yet
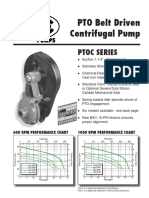
- Ptoc 03-13Document4 pagesPtoc 03-13Matias Contreras KöbrichNo ratings yet
- Science 9 - Q2 - Week 5-M13-M16Document32 pagesScience 9 - Q2 - Week 5-M13-M16Rhyan Zero-four BaluyutNo ratings yet
- Parent Record 74-75Document6 pagesParent Record 74-75Sujan BaralNo ratings yet
- Social Audit - Definition - Objectives - Need - Disclosure of Information PDFDocument4 pagesSocial Audit - Definition - Objectives - Need - Disclosure of Information PDFSorabh KumarNo ratings yet
- Scentsy Layers Ingrediants ListDocument16 pagesScentsy Layers Ingrediants ListsimonejanesNo ratings yet
- FOURTH Quarter - Module 1: Structure and Functions of The Digestive SystemDocument5 pagesFOURTH Quarter - Module 1: Structure and Functions of The Digestive SystemChristian jade Quijano100% (1)
- FOMB - Letter - Senate of Puerto Rico - Response Letter Section 204 (A) (6) SB 1304 - February 7, 2024Document3 pagesFOMB - Letter - Senate of Puerto Rico - Response Letter Section 204 (A) (6) SB 1304 - February 7, 2024Metro Puerto RicoNo ratings yet
- Narvacan - Week 5 - 6 Concurrecy - Processes Synchronization and DeadlocksDocument24 pagesNarvacan - Week 5 - 6 Concurrecy - Processes Synchronization and DeadlocksArnold NarvacanNo ratings yet
- IBM x3850X5 x3950X5 HX5 OverviewDocument118 pagesIBM x3850X5 x3950X5 HX5 OverviewTruong Anh VuNo ratings yet
- Vitamin Water 1Document34 pagesVitamin Water 1mei1004100% (10)
- First-Order Partial DerivativesDocument4 pagesFirst-Order Partial DerivativesRochelle ParedesNo ratings yet
- Fao 2016 The State of Food and Agriculture PDFDocument194 pagesFao 2016 The State of Food and Agriculture PDFYenny Rodriguez100% (1)
- Steel Connection MethodsDocument18 pagesSteel Connection MethodsVishnuVardhan100% (1)
- Analog ModulationDocument26 pagesAnalog Modulationmraziff2009No ratings yet
- HCM Cloud - Global HR - New Hire and Manage ChangesDocument53 pagesHCM Cloud - Global HR - New Hire and Manage ChangesRAM SNo ratings yet
- Couch To 5K Jogging PlanDocument2 pagesCouch To 5K Jogging PlanByzantine PGNo ratings yet
- Govt. Pilot High School Rawalakot AJK Pre-Board ExamDocument2 pagesGovt. Pilot High School Rawalakot AJK Pre-Board ExamAbdul qadeerNo ratings yet