You might also like
- Methane Mitigation Global Summit Event Agenda66gJmFneLs0Uka79kaphvNEH1gLxwA14MVkznCe5Document22 pagesMethane Mitigation Global Summit Event Agenda66gJmFneLs0Uka79kaphvNEH1gLxwA14MVkznCe5Nyasimi GeoffreyNo ratings yet
- VisArt10E SampleEbookDocument76 pagesVisArt10E SampleEbookFuture Managers Pty Ltd83% (6)
- Dinosaurs That Never WereDocument66 pagesDinosaurs That Never WereAiden Turner100% (8)
- The Effect of Continuous Positive Airway Pressure and Mandibular Advancement Device On Sleep Bruxism Intensity in Obstructive Sleep Apnea PatientsDocument10 pagesThe Effect of Continuous Positive Airway Pressure and Mandibular Advancement Device On Sleep Bruxism Intensity in Obstructive Sleep Apnea PatientsMarco Saavedra BurgosNo ratings yet
- Fphar 09 01513Document8 pagesFphar 09 01513william lozaNo ratings yet
- Life 13 00296Document12 pagesLife 13 00296venancioNo ratings yet
- 1 s2.0 S1389945723001144 MainDocument7 pages1 s2.0 S1389945723001144 MainsoylahijadeunvampiroNo ratings yet
- Fulltext - Ajsd v2 Id1016Document3 pagesFulltext - Ajsd v2 Id1016belleNo ratings yet
- Smoking and Sleep Apnea Duration Mediated The Sex Difference in Daytime Sleepiness in OSA PatientsDocument9 pagesSmoking and Sleep Apnea Duration Mediated The Sex Difference in Daytime Sleepiness in OSA PatientsDamian MendelevNo ratings yet
- 2021 - Front Med - Ragnoli - Interrelatsionship BTWN OSA and Severe AsthmaDocument8 pages2021 - Front Med - Ragnoli - Interrelatsionship BTWN OSA and Severe AsthmaManuel MendezNo ratings yet
- State of The Art: Epidemiology of Obstructive Sleep ApneaDocument23 pagesState of The Art: Epidemiology of Obstructive Sleep ApneaMelly NoviaNo ratings yet
- Bruno 2013Document7 pagesBruno 2013Ferdy LainsamputtyNo ratings yet
- Case ReportsDocument11 pagesCase ReportsYash KakodkerNo ratings yet
- Efficacy of Atomoxetine Plus Oxybutynin in The Treatment of Obstructive Sleep Apnea With Moderate Pharyngeal CollapsibilityDocument9 pagesEfficacy of Atomoxetine Plus Oxybutynin in The Treatment of Obstructive Sleep Apnea With Moderate Pharyngeal CollapsibilityAlain NICOLASNo ratings yet
- Art 6 CSDocument11 pagesArt 6 CSalicia salvatoreNo ratings yet
- Displasia BroncopulmonarDocument4 pagesDisplasia BroncopulmonarRaul VillacresNo ratings yet
- Correlation Between Apnea Severity and Sagittal CeDocument10 pagesCorrelation Between Apnea Severity and Sagittal Cesolodont1No ratings yet
- Ryan 2018Document6 pagesRyan 2018Hisham GamalNo ratings yet
- Consequences of OSADocument11 pagesConsequences of OSAhammodihotmailcomNo ratings yet
- State of The Art: Epidemiology of Obstructive Sleep ApneaDocument23 pagesState of The Art: Epidemiology of Obstructive Sleep Apneaa3llamNo ratings yet
- 2012-David-CVD Consequences of OSADocument14 pages2012-David-CVD Consequences of OSAGoongGiing MatinaNo ratings yet
- Pathophysiological Mechanisms and Therapeutic Approaches in Obstructive Sleep Apnea SyndromeDocument46 pagesPathophysiological Mechanisms and Therapeutic Approaches in Obstructive Sleep Apnea SyndromeFrancisco Javier MacíasNo ratings yet
- The Effects of Intravenous Aminophylline On Level of Consciousness in Acute Intentional Benzodiazepines Poisoning in Comparison To FlumazenilDocument6 pagesThe Effects of Intravenous Aminophylline On Level of Consciousness in Acute Intentional Benzodiazepines Poisoning in Comparison To FlumazenilMarco Antonio Rosales GuerreroNo ratings yet
- Insomnia and Excessive Daytime Sleepiness in ObstrDocument3 pagesInsomnia and Excessive Daytime Sleepiness in ObstrChatterjee SomanNo ratings yet
- Comorbid Insomnia and Obstructive Sleep Apnea: Challenges For Clinical Practice and ResearchDocument9 pagesComorbid Insomnia and Obstructive Sleep Apnea: Challenges For Clinical Practice and ResearchIriawan Indra PutraNo ratings yet
- Fpsyt 13 1067437Document9 pagesFpsyt 13 1067437putriNo ratings yet
- Jurnal OSADocument10 pagesJurnal OSAflorensiaNo ratings yet
- Privação Do SonoDocument3 pagesPrivação Do SonoHugo BarbosaNo ratings yet
- Heenam 2018 Sleep Dependent Directional Coupling ofDocument8 pagesHeenam 2018 Sleep Dependent Directional Coupling ofArda Safira Kardono D4AJNo ratings yet
- Apnea Hipoapnea PDFDocument7 pagesApnea Hipoapnea PDFleidys solanoNo ratings yet
- ObstructiveSleepApnoeaSyndrome, EndothelialFunctionandMarkersof Endothelialization - changesafterCPAPDocument13 pagesObstructiveSleepApnoeaSyndrome, EndothelialFunctionandMarkersof Endothelialization - changesafterCPAPAlzeniraNo ratings yet
- Treatment of Obstructive Sleep Apnea With Oral Appliances: Research Open AccessDocument9 pagesTreatment of Obstructive Sleep Apnea With Oral Appliances: Research Open AccessVinay MuppanaNo ratings yet
- Effect of Myofunctional Therapy On Children With Obstructive Sleep ApneaDocument8 pagesEffect of Myofunctional Therapy On Children With Obstructive Sleep ApneaIrzam PratamaNo ratings yet
- Evidence For The Pathophysiology of InsomniaDocument2 pagesEvidence For The Pathophysiology of InsomniaEDGAR DÍAZ URDANETANo ratings yet
- Lyu 2019Document8 pagesLyu 2019Endang Dwii SuhartiningsihNo ratings yet
- Acupuncture As An Effective Treatment For Moderate Obstructive ApneaDocument51 pagesAcupuncture As An Effective Treatment For Moderate Obstructive ApneaManuel LavadosNo ratings yet
- Obstructive Sleep Apnoea and AnaesthesiaDocument8 pagesObstructive Sleep Apnoea and AnaesthesiaBilly AsifNo ratings yet
- 2014 - Sleep Breath - Greenberg - Increased Prevelance of Obst Lung Disease and OSADocument7 pages2014 - Sleep Breath - Greenberg - Increased Prevelance of Obst Lung Disease and OSAManuel MendezNo ratings yet
- Decreased Blood Pressure Among Community Dwelling Older Adults Following Progressive Muscle Relaxation and Music Therapy (RESIK)Document6 pagesDecreased Blood Pressure Among Community Dwelling Older Adults Following Progressive Muscle Relaxation and Music Therapy (RESIK)Rara Mitha64No ratings yet
- 3 PDFDocument6 pages3 PDFivanNo ratings yet
- Review Article Obstructive Sleep Apnea and Cardiovascular Diseases: Sad Realities and Untold Truths Regarding Care of Patients in 2022Document10 pagesReview Article Obstructive Sleep Apnea and Cardiovascular Diseases: Sad Realities and Untold Truths Regarding Care of Patients in 2022Hashan AbeyrathneNo ratings yet
- CPAP Vs MADDocument13 pagesCPAP Vs MADsikawat thanaviratananichNo ratings yet
- Long Term Management of Obstructive Sleep Apnea AnDocument9 pagesLong Term Management of Obstructive Sleep Apnea AnsukiyantoNo ratings yet
- Punjabi, 2008Document8 pagesPunjabi, 2008a3llamNo ratings yet
- Genome Wide Gene Expression Array Identifies NovelDocument16 pagesGenome Wide Gene Expression Array Identifies NovelAswin RNo ratings yet
- Obstructive Sleep ApneaDocument21 pagesObstructive Sleep ApneaIJAR JOURNALNo ratings yet
- The Efficacy and Safety of Acupuncture WANGDocument4 pagesThe Efficacy and Safety of Acupuncture WANGlucasaguiar1996No ratings yet
- 2021 Nov 10 Sas Fenotip Final SasDocument51 pages2021 Nov 10 Sas Fenotip Final SasClaudia ToncaNo ratings yet
- A 5-Year Follow-Up Study On The Relationship Between Obstructive Sleep Apnea and Parkinson DiseaseDocument6 pagesA 5-Year Follow-Up Study On The Relationship Between Obstructive Sleep Apnea and Parkinson DiseaseQonita Aizati QomaruddinNo ratings yet
- Pulmonary & Respiratory MedicineDocument6 pagesPulmonary & Respiratory MedicineOliver Febrian SampelilingNo ratings yet
- Obstructive Sleep Apnea in Chronic Obstructive PulmonaryDocument5 pagesObstructive Sleep Apnea in Chronic Obstructive PulmonaryGeorge Cătălin AlexandruNo ratings yet
- Retrospective Analysis of Real-World Data For The Treatment ofDocument10 pagesRetrospective Analysis of Real-World Data For The Treatment ofvenancioNo ratings yet
- Apnea and InflammationDocument19 pagesApnea and Inflammationarcm1949No ratings yet
- European Journal of Internal Medicine: Morohunfolu E. Akinnusi, Ranime Saliba, Jahan Porhomayon, Ali A. El-SolhDocument8 pagesEuropean Journal of Internal Medicine: Morohunfolu E. Akinnusi, Ranime Saliba, Jahan Porhomayon, Ali A. El-SolhBochand CoolNo ratings yet
- Evidence For The Pathophysiology of Insomnia.: Sleep May 2009Document3 pagesEvidence For The Pathophysiology of Insomnia.: Sleep May 2009citra dewiNo ratings yet
- The Bidirectional Relationship Between Obstructive Sleep Apnea and Metabolic DiseaseDocument14 pagesThe Bidirectional Relationship Between Obstructive Sleep Apnea and Metabolic DiseaseVenny SarumpaetNo ratings yet
- Variation of Cognition and Cerebral Activity With Severity of Airflow Obstruction in CopdDocument9 pagesVariation of Cognition and Cerebral Activity With Severity of Airflow Obstruction in CopdIJAR JOURNALNo ratings yet
- Agneta 2Document13 pagesAgneta 2ganesh goreNo ratings yet
- Nihms 735051Document17 pagesNihms 735051diah_budiarti_1No ratings yet
- Bhattacharjee2010-Adenotonsillectomy Outcomes in Treatment of Obstructive Sleep Apnea in ChildrenDocument8 pagesBhattacharjee2010-Adenotonsillectomy Outcomes in Treatment of Obstructive Sleep Apnea in ChildrenCEBDOF BRASILNo ratings yet
- 2016 Article 950 PDFDocument7 pages2016 Article 950 PDFTitan LinggastiwiNo ratings yet
- Fast Facts: Excessive Daytime Sleepiness Associated with Obstructive Sleep ApneaFrom EverandFast Facts: Excessive Daytime Sleepiness Associated with Obstructive Sleep ApneaNo ratings yet
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationFrom EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehNo ratings yet
- The Volatile Oil of Ziziphora: HispanicaDocument3 pagesThe Volatile Oil of Ziziphora: HispanicaРусланNo ratings yet
- Chocolate Cake RecipesDocument59 pagesChocolate Cake Recipesiki292No ratings yet
- Surgical Management of Dilocated Lens: Mohammad Ghoreishi, MDDocument15 pagesSurgical Management of Dilocated Lens: Mohammad Ghoreishi, MDwawan 88No ratings yet
- Fuel Supply Proposal - PDF - Safety - Filtration 1 PDFDocument6 pagesFuel Supply Proposal - PDF - Safety - Filtration 1 PDFSuleimanNo ratings yet
- Escrow Rbi RulesDocument2 pagesEscrow Rbi RulesAtiqur Rahman BarbhuiyaNo ratings yet
- First-Order Partial DerivativesDocument4 pagesFirst-Order Partial DerivativesRochelle ParedesNo ratings yet
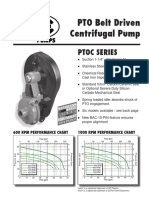
- Ptoc 03-13Document4 pagesPtoc 03-13Matias Contreras KöbrichNo ratings yet
- Capability-Based DevelopmentDocument46 pagesCapability-Based DevelopmentEero HosiaisluomaNo ratings yet
- 329-Article Text-1006-1-10-20190603Document16 pages329-Article Text-1006-1-10-20190603Jia QuijanoNo ratings yet
- Lecture 2 - Project ManagementDocument30 pagesLecture 2 - Project ManagementktubdaNo ratings yet
- Estros Cycle in DogsDocument3 pagesEstros Cycle in DogsnessimmounirNo ratings yet
- Eom SummaryDocument103 pagesEom SummaryJonNo ratings yet
- Gas Engine Technical Data: Load 100% 75% 50% Rating and EfficiencyDocument3 pagesGas Engine Technical Data: Load 100% 75% 50% Rating and EfficiencyAM76No ratings yet
- French Conjugating The Verb MangerDocument6 pagesFrench Conjugating The Verb MangerMiss Evie ElenorNo ratings yet
- BAUSER Brochure Time Counters Pulse Counters Modules Time Switchers 1709 en v1.6Document40 pagesBAUSER Brochure Time Counters Pulse Counters Modules Time Switchers 1709 en v1.6Csaba SándorNo ratings yet
- Schools PDFDocument211 pagesSchools PDFpankajbaberwalNo ratings yet
- Formal Essay ExamplesDocument2 pagesFormal Essay Examplesfz6etcq7No ratings yet
- Statistics and ProbabilityDocument20 pagesStatistics and ProbabilityAngel Lorayne SalvacionNo ratings yet
- Ptosis Definition of Eyelid Ptosis: Abnormally Low Position of The Upper Eyelid Margin Caused by PoorDocument6 pagesPtosis Definition of Eyelid Ptosis: Abnormally Low Position of The Upper Eyelid Margin Caused by PoortiamaharaniNo ratings yet
- Parent Record 74-75Document6 pagesParent Record 74-75Sujan BaralNo ratings yet
- Opportunities and Challenges of Petroleum Fuel Subsidy: by Reginald C. Stanley Executive Secretary, PPPRADocument13 pagesOpportunities and Challenges of Petroleum Fuel Subsidy: by Reginald C. Stanley Executive Secretary, PPPRAmuktar ibrahimNo ratings yet
- T 1699375835 Comparatives and Superlatives Powerpoint Teens A2 b1 - Ver - 2Document26 pagesT 1699375835 Comparatives and Superlatives Powerpoint Teens A2 b1 - Ver - 2carmenNo ratings yet
- Efficacy and Adverse Events of Oral Isotretinoin For Acne: A Systematic ReviewDocument10 pagesEfficacy and Adverse Events of Oral Isotretinoin For Acne: A Systematic ReviewFerryGoNo ratings yet
- TOR Starter Set The ShireDocument56 pagesTOR Starter Set The ShireAugust Tsugua100% (1)
- January Exam ScheduleDocument1 pageJanuary Exam ScheduleLena HannaNo ratings yet
- BadmintonDocument3 pagesBadmintonPratikRoyNo ratings yet
- R.A 9292 Article Vi: Penal Provision and Assistance of Law Enforcement AgenciesDocument12 pagesR.A 9292 Article Vi: Penal Provision and Assistance of Law Enforcement AgenciesMagNo ratings yet