You might also like
- Ancestral Healing Summit 2022 Day 3Document7 pagesAncestral Healing Summit 2022 Day 3Paul Ioan PopescuNo ratings yet
- Detailed Lesson Plan in Science 5 1st QuarterDocument8 pagesDetailed Lesson Plan in Science 5 1st QuarterAndrewNo ratings yet
- JHA LiftingDocument4 pagesJHA Liftingsyamimi balkhisNo ratings yet
- TICKLER-PRINT Pedia PDFDocument8 pagesTICKLER-PRINT Pedia PDFCarlos H. AcuñaNo ratings yet
- The Herbst Appliance Research BasedDocument252 pagesThe Herbst Appliance Research BasedMu'taz ArmanNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Covid SedDocument12 pagesCovid SedJov1dNo ratings yet
- Estudio de Cohorte ObservacionalDocument22 pagesEstudio de Cohorte ObservacionalHARUMI DEL ROSARIO MONTALVAN VEGANo ratings yet
- Early Versus Late Awake Prone Positioning in Non-Intubated Patients With COVID-19Document9 pagesEarly Versus Late Awake Prone Positioning in Non-Intubated Patients With COVID-19Fadil AhmadNo ratings yet
- Huang2020 Article ImpactOfCoronavirusDisease2019Document10 pagesHuang2020 Article ImpactOfCoronavirusDisease2019yuris hikmanNo ratings yet
- Association Between Early Tracheostomy and Patient Outcomes in Critically Ill Patients On Mechanical Ventilation A Multicenter Cohort StudyDocument10 pagesAssociation Between Early Tracheostomy and Patient Outcomes in Critically Ill Patients On Mechanical Ventilation A Multicenter Cohort StudyEloisa Hoyo MacouzetNo ratings yet
- Diagnosing Ventilator-Associated Pneumonia (Vap) in Uk Nhs Icus: The Perceived Value and Role of A Novel Optical TechnologyDocument11 pagesDiagnosing Ventilator-Associated Pneumonia (Vap) in Uk Nhs Icus: The Perceived Value and Role of A Novel Optical Technologycarmen rosa secce pedrazaNo ratings yet
- ALGORITMODocument9 pagesALGORITMOCristianMP96No ratings yet
- Lung Function and Breathing Patterns in Hospitalised COVID-19 Survivors: A Review of post-COVID-19 ClinicsDocument12 pagesLung Function and Breathing Patterns in Hospitalised COVID-19 Survivors: A Review of post-COVID-19 ClinicsRiandhani UpitariniaNo ratings yet
- Debilidad Gral y DiafragmaticaDocument9 pagesDebilidad Gral y DiafragmaticaterapiafisicapilaresNo ratings yet
- Debilidad Gral y DiafragmaticaDocument9 pagesDebilidad Gral y DiafragmaticaGustavoGarcíaNo ratings yet
- Clinical Characteristics and Durations of Hospitalized Patients With COVID-19 in BeijingDocument18 pagesClinical Characteristics and Durations of Hospitalized Patients With COVID-19 in BeijingTOMMYNo ratings yet
- Apa GituDocument8 pagesApa GituRiadi RifqiNo ratings yet
- Maximum CT ScoreDocument11 pagesMaximum CT ScoreChavdarNo ratings yet
- Sequelae of COVID-19 Among Previously Hospitalized Patients Up To 1 Year After Discharge - A Systematic Review and Meta-AnalysisDocument43 pagesSequelae of COVID-19 Among Previously Hospitalized Patients Up To 1 Year After Discharge - A Systematic Review and Meta-AnalysisRicardo Pariona LlanosNo ratings yet
- Goh2020 Article PreparingYourIntensiveCareUnitDocument19 pagesGoh2020 Article PreparingYourIntensiveCareUnitBAGUIO CATSNo ratings yet
- Preparing Your Intensive Care Unit For The COVID-19 Pandemic: Practical Considerations and StrategiesDocument12 pagesPreparing Your Intensive Care Unit For The COVID-19 Pandemic: Practical Considerations and Strategiesririn puspasariNo ratings yet
- Construct Validity of The Post-COVID-19 Functional Status Scale in Adult Subjects With COVID-19Document10 pagesConstruct Validity of The Post-COVID-19 Functional Status Scale in Adult Subjects With COVID-19Patricia Acevedo ArancibiaNo ratings yet
- Luyt2020 Article Ventilator-associatedPneumoniaDocument10 pagesLuyt2020 Article Ventilator-associatedPneumoniaAlexandra Pavel SucmanschiNo ratings yet
- Zhao - 2023 - The Impact of The New Acute Respiratory Distress SDocument10 pagesZhao - 2023 - The Impact of The New Acute Respiratory Distress Sgavain.ferronsNo ratings yet
- In For The Long-Haul? Seropositivity and Sequelae 1 Year Post COVID-19Document2 pagesIn For The Long-Haul? Seropositivity and Sequelae 1 Year Post COVID-19Danielle AlmeidaNo ratings yet
- Infection Related Catheter Complications in Patients Undergoing Prone Positioning For Acute Respiratory Distress Syndrome: An Exposed/unexposed StudyDocument9 pagesInfection Related Catheter Complications in Patients Undergoing Prone Positioning For Acute Respiratory Distress Syndrome: An Exposed/unexposed Studyluandry medinaNo ratings yet
- The PROMIZING Trial Enrollment Algorithm For Early Identification of Patients Ready For Unassisted BreathingDocument9 pagesThe PROMIZING Trial Enrollment Algorithm For Early Identification of Patients Ready For Unassisted BreathingGeorge Morales MuñozNo ratings yet
- Comprehensive Risk Assessment For Hospital-AcquireDocument12 pagesComprehensive Risk Assessment For Hospital-AcquirevonnyNo ratings yet
- Systematic Review and Meta-Analysis of TracheostomyDocument12 pagesSystematic Review and Meta-Analysis of Tracheostomycelma44No ratings yet
- Valor PX Score US COVIDDocument12 pagesValor PX Score US COVIDTeresa MontesNo ratings yet
- CT Radiomics Facilitates More Accurate Diagnosis of COVID-19 Pneumonia: Compared With CO-RADSDocument12 pagesCT Radiomics Facilitates More Accurate Diagnosis of COVID-19 Pneumonia: Compared With CO-RADSVlad VictorNo ratings yet
- Congestión Por LíquidosDocument10 pagesCongestión Por Líquidosandres ruizNo ratings yet
- Prediction of Extubation Outcome in Critically Ill Patients: A Systematic Review and Meta-AnalysisDocument12 pagesPrediction of Extubation Outcome in Critically Ill Patients: A Systematic Review and Meta-AnalysisLucas ViolaNo ratings yet
- Acupressure Therapy and Liu Zi Jue Qigong For Pulmonary Function and Quality of Life in Patients With Severe Novel Coronavirus Pneumonia (COVID-19) : A Study Protocol For A Randomized Controlled TrialDocument11 pagesAcupressure Therapy and Liu Zi Jue Qigong For Pulmonary Function and Quality of Life in Patients With Severe Novel Coronavirus Pneumonia (COVID-19) : A Study Protocol For A Randomized Controlled TrialArif RahmatullahNo ratings yet
- cs3 Protocol-V2.5Document8 pagescs3 Protocol-V2.5CheferishNo ratings yet
- A Systematic Review of The Systematic Review of Post COVID-19 SyndromeDocument6 pagesA Systematic Review of The Systematic Review of Post COVID-19 Syndromeeditorial.boardNo ratings yet
- Frontiers - Biomarkers in Long COVID-19 - A Systematic ReviewDocument15 pagesFrontiers - Biomarkers in Long COVID-19 - A Systematic Review9jz5dzj5gwNo ratings yet
- s13054 023 04429 2Document10 pagess13054 023 04429 2404140No ratings yet
- Preprint corticoidesNeuminiaCOVIDDocument16 pagesPreprint corticoidesNeuminiaCOVIDJorgelina BernetNo ratings yet
- Jurnal Soal DDocument15 pagesJurnal Soal DrianarahmadhanyNo ratings yet
- Y. AL HashmiDocument11 pagesY. AL HashmiAzam alausyNo ratings yet
- Focused Liquid Ultrasonography in Dropsy Protocol For Quantitative Assessment of Subcutaneous EdemaDocument12 pagesFocused Liquid Ultrasonography in Dropsy Protocol For Quantitative Assessment of Subcutaneous EdemaLex X PabloNo ratings yet
- 2021 Article 988Document5 pages2021 Article 988Jhosua MendezNo ratings yet
- 2022 The Effects of Hyperbaric Oxygen Therapy (HBOT) On Coronavirus Disease-2019 (COVID-19) - A Systematic ReviewDocument12 pages2022 The Effects of Hyperbaric Oxygen Therapy (HBOT) On Coronavirus Disease-2019 (COVID-19) - A Systematic ReviewabnfojoNo ratings yet
- Prolonged Prone Position Ventilation For Sars-Cov-2 Patients Is Feasible and EffectiveDocument3 pagesProlonged Prone Position Ventilation For Sars-Cov-2 Patients Is Feasible and Effectivecarlos_julianNo ratings yet
- ExperimentalDocument6 pagesExperimentalDiego TorresNo ratings yet
- Multi-Organ Point-Of-Care Ultrasound For Covid-19 (Pocus4Covid) : International Expert ConsensusDocument18 pagesMulti-Organ Point-Of-Care Ultrasound For Covid-19 (Pocus4Covid) : International Expert ConsensusAnna JuniedNo ratings yet
- Clinical Characteristics of COVID-19 Complicated With Pleural EffusionDocument10 pagesClinical Characteristics of COVID-19 Complicated With Pleural EffusionInternal MedicineNo ratings yet
- Long-Term Symptoms After Sars-Cov-2 Infection in A Cohort of Hospital Employees: Duration and Predictive FactorsDocument10 pagesLong-Term Symptoms After Sars-Cov-2 Infection in A Cohort of Hospital Employees: Duration and Predictive FactorsWestwickateNo ratings yet
- s12941 021 00454 7Document8 pagess12941 021 00454 7taufik.abdiNo ratings yet
- An Updated Systematic Review of The Therapeutic Role of Hydroxychloroquine in Coronavirus Disease 19 (COVID 19)Document11 pagesAn Updated Systematic Review of The Therapeutic Role of Hydroxychloroquine in Coronavirus Disease 19 (COVID 19)johngeniusboyNo ratings yet
- s13017 020 00343 yDocument10 pagess13017 020 00343 yPintakasari WNo ratings yet
- Im 2022Document10 pagesIm 2022YogiHadityaNo ratings yet
- Prona Estendida SDRADocument9 pagesProna Estendida SDRAdado_rossiNo ratings yet
- Novel Criteria To Classify ARDS Severity Using A Machine Learning ApproachDocument9 pagesNovel Criteria To Classify ARDS Severity Using A Machine Learning ApproachTeofanes PonceNo ratings yet
- Jurnal 8Document9 pagesJurnal 8kalstarNo ratings yet
- Pilot Trial of High-Dose Vitamin C in Critically Ill COVID-19 PatientsDocument12 pagesPilot Trial of High-Dose Vitamin C in Critically Ill COVID-19 Patientska waiiNo ratings yet
- Role of Respiratory Intermediate Care Units During The SARS-CoV-2 PandemicDocument7 pagesRole of Respiratory Intermediate Care Units During The SARS-CoV-2 PandemicJHNo ratings yet
- Fmed 09 837420Document12 pagesFmed 09 837420Amanda SchaefferNo ratings yet
- Los Systematic Review Main UpdateDocument26 pagesLos Systematic Review Main UpdateMuhammad sadadNo ratings yet
- Cid RT PCR Positive Over TimeDocument12 pagesCid RT PCR Positive Over TimePatrick CoNo ratings yet
- 2020 04 24 20078782v1 FullDocument41 pages2020 04 24 20078782v1 FullAbay SisayNo ratings yet
- Pham Et. Al. (2021)Document16 pagesPham Et. Al. (2021)Sukrit PalNo ratings yet
- 1160 4636 1 PBDocument23 pages1160 4636 1 PBEka NovitaNo ratings yet
- Phase 1 IntroDocument7 pagesPhase 1 Intro22024552 Hà Đăng LongNo ratings yet
- 2022 Nursing Skills Checklist 2104p 1Document5 pages2022 Nursing Skills Checklist 2104p 1api-664680120No ratings yet
- Sample FS ProtocolDocument47 pagesSample FS ProtocolAika May GarbeNo ratings yet
- US Ganjil Cls XI Bhs - Inggris 2019Document9 pagesUS Ganjil Cls XI Bhs - Inggris 2019FitrianaNo ratings yet
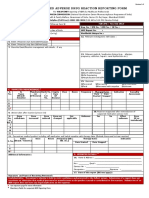
- ADRnewReporting Form 1.4Document2 pagesADRnewReporting Form 1.4Sourabh kundara0% (1)
- Methylene Blue InstructionsDocument1 pageMethylene Blue InstructionsnepretipNo ratings yet
- Obsessive Compulsive Disorder Punjabi Instant Download 1Document3 pagesObsessive Compulsive Disorder Punjabi Instant Download 1Ameera ChauhanNo ratings yet
- PT10V Quick Reference ManualDocument6 pagesPT10V Quick Reference ManualOscar LaraNo ratings yet
- VAIP BLS Ambulance Checklist 20220701Document9 pagesVAIP BLS Ambulance Checklist 20220701jonathan layaNo ratings yet
- 763 2409 1 PBDocument4 pages763 2409 1 PBBagus Adi PratamaNo ratings yet
- Newswriting ExercisesDocument13 pagesNewswriting ExercisesMichelle Alejo CortezNo ratings yet
- The Relationship Between Physical and Mental Health: A Mediation AnalysisDocument9 pagesThe Relationship Between Physical and Mental Health: A Mediation AnalysisFeiga MaharaniNo ratings yet
- Prediction of The Age of Maximum Puberal Growth in Body HeightDocument11 pagesPrediction of The Age of Maximum Puberal Growth in Body HeightNico A Ore LudeNo ratings yet
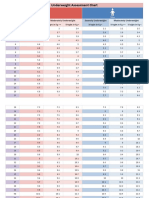
- Underweight Assessment Chart: Weight in KG Weight in KG Weight in KGDocument3 pagesUnderweight Assessment Chart: Weight in KG Weight in KG Weight in KGYuvraj GargNo ratings yet
- FINAL Result 2021 FAICODocument2 pagesFINAL Result 2021 FAICOarnabbiswasNo ratings yet
- Dahmer Monster The Jeffrey Dahmer Story 106 Silenced 2022Document40 pagesDahmer Monster The Jeffrey Dahmer Story 106 Silenced 2022Jarret MataNo ratings yet
- O'Leary v. Cannon and DulyDocument16 pagesO'Leary v. Cannon and DulyCrainsChicagoBusinessNo ratings yet
- NO Nama Barang Pabrik Sisa Satuan: Daftar HargaDocument33 pagesNO Nama Barang Pabrik Sisa Satuan: Daftar HargaMalik TeamNo ratings yet
- Interceptive Orthodontic Treatment in Singapore: A Descriptive StudyDocument6 pagesInterceptive Orthodontic Treatment in Singapore: A Descriptive StudyShourovNo ratings yet
- Ayurveda Jeevana VedamDocument48 pagesAyurveda Jeevana Vedamlilly1468388% (16)
- Referral Slip - Friendlycare FoundationDocument1 pageReferral Slip - Friendlycare Foundationmathhew bepplerNo ratings yet
- Manual Oregon Scientific BPW120Document121 pagesManual Oregon Scientific BPW120Marcelo PolicarpoNo ratings yet
- Fall Asleep FastDocument3 pagesFall Asleep Fastrzn34185No ratings yet
- Medical Form NITJSR-ACD-ADM-002 - BTechDocument2 pagesMedical Form NITJSR-ACD-ADM-002 - BTechFUN FACTNo ratings yet