You might also like
- Brainwave Cymatic Frequency ListingDocument28 pagesBrainwave Cymatic Frequency ListingUverso100% (1)
- Focus 3 2nd Word StoreDocument19 pagesFocus 3 2nd Word StoreSvetlana Bykovshchenko-Tymoshok0% (1)
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeFrom EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeNo ratings yet
- Essentials of Marketing Research 5th Edition Zikmund Test BankDocument18 pagesEssentials of Marketing Research 5th Edition Zikmund Test Bankbrittanylamsfwkpbmzce100% (18)
- Necklace and Magi CCDocument1 pageNecklace and Magi CCMarimar MarianoNo ratings yet
- INF-γ biomarker in differentiating tuberculosis pleural effusionDocument3 pagesINF-γ biomarker in differentiating tuberculosis pleural effusionflik_gantengNo ratings yet
- Diagnostic Accuracy of Pleural Effusion Mononuclear Cells/Leukocyte Ratio in Tuberculous PleurisyDocument7 pagesDiagnostic Accuracy of Pleural Effusion Mononuclear Cells/Leukocyte Ratio in Tuberculous PleurisykhaulahkarimahNo ratings yet
- Comparison of Laboratory Testing Methods For The Diagnosis of Tuberculous Pleurisy in ChinaDocument5 pagesComparison of Laboratory Testing Methods For The Diagnosis of Tuberculous Pleurisy in ChinaclaryntafreyaaNo ratings yet
- Procalcitonin 6Document11 pagesProcalcitonin 6zivl1984No ratings yet
- PIIS2214109X23001353Document14 pagesPIIS2214109X23001353Joaquin OlivaresNo ratings yet
- Diagnostic Potential Of 16 Kda (Hspx, Α-Crystalline) Antigen For Serodiagnosis Of TuberculosisDocument7 pagesDiagnostic Potential Of 16 Kda (Hspx, Α-Crystalline) Antigen For Serodiagnosis Of TuberculosispouralNo ratings yet
- PIIS1201971218345090Document9 pagesPIIS1201971218345090favorendaNo ratings yet
- Fcimb 11 585919Document9 pagesFcimb 11 585919Asu AlexNo ratings yet
- Diagnostic Performance of Adenosine Deaminase Activity in Pleural Fluid A Single-CenterDocument5 pagesDiagnostic Performance of Adenosine Deaminase Activity in Pleural Fluid A Single-Centerq8xx75sjnyNo ratings yet
- Pi Is 1201971213002142Document5 pagesPi Is 1201971213002142melisaberlianNo ratings yet
- RetrieveDocument11 pagesRetrieveMICHAEL NUGROHONo ratings yet
- The Utility of Peripheral Blood Leucocyte Ratios As Biomarkers in Infectious Diseases A Systematic Review and Meta-AnalysisDocument10 pagesThe Utility of Peripheral Blood Leucocyte Ratios As Biomarkers in Infectious Diseases A Systematic Review and Meta-AnalysisYenis RodriguezNo ratings yet
- Biomarkers in Infectious DiseasesDocument6 pagesBiomarkers in Infectious DiseasesjuangbuenoNo ratings yet
- Granulomatous Epididymo-Orchitis: Diagnosis by Fine Needle AspirationDocument4 pagesGranulomatous Epididymo-Orchitis: Diagnosis by Fine Needle AspirationAnonymous tlIQeKLriNo ratings yet
- Performance of Radiologists in Differentiating COVID-19 From Non-COVID-19 Viral Pneumonia at Chest CTDocument9 pagesPerformance of Radiologists in Differentiating COVID-19 From Non-COVID-19 Viral Pneumonia at Chest CTrishaNo ratings yet
- Lembar Jawaban SoalDocument5 pagesLembar Jawaban SoalWahyuNo ratings yet
- JurnalDocument5 pagesJurnalgustina mariantiNo ratings yet
- 209 Full PDFDocument8 pages209 Full PDFAngga PratamaNo ratings yet
- Marneffei: Cytological Diagnosis of Penicillium InfectionDocument5 pagesMarneffei: Cytological Diagnosis of Penicillium InfectionAnonymous oQtve4oNo ratings yet
- Ann Thorac Surg 2015Document5 pagesAnn Thorac Surg 2015sraimundo_1No ratings yet
- Pooled Analysis of 163 Published Tuberculous Peritonitis Cases From TurkeyDocument7 pagesPooled Analysis of 163 Published Tuberculous Peritonitis Cases From TurkeyDumitru RadulescuNo ratings yet
- Adilistya 2020Document1 pageAdilistya 2020shahhareshNo ratings yet
- 2165-Article Text-2597-1-10-20200105Document7 pages2165-Article Text-2597-1-10-20200105IKA 79No ratings yet
- Limitation Graft BiopsyDocument11 pagesLimitation Graft BiopsyWEE LENG GANNo ratings yet
- Meta-Analysis of Diagnostic Procedures For Pneumocystis Carinii Pneumonia in HIV-1-infected PatientsDocument8 pagesMeta-Analysis of Diagnostic Procedures For Pneumocystis Carinii Pneumonia in HIV-1-infected PatientsJenniffer M. Rodiño MontoyaNo ratings yet
- Cytological Analysis of Bronchial Washings in RSUD Pasar MingguDocument8 pagesCytological Analysis of Bronchial Washings in RSUD Pasar MingguReza DigambiroNo ratings yet
- BestDocument11 pagesBestSalmiyah HasibuanNo ratings yet
- Turner Et Al.2020Document13 pagesTurner Et Al.2020pelleNo ratings yet
- Correlation of Neutrophil-Lymphocyte Ratio (NLR) With Sofa Score As A Parameter of Organic Dysfunction of Sepsis Patients in ICU Haji Adam Malik (HAM) General Hospital MedanDocument5 pagesCorrelation of Neutrophil-Lymphocyte Ratio (NLR) With Sofa Score As A Parameter of Organic Dysfunction of Sepsis Patients in ICU Haji Adam Malik (HAM) General Hospital MedanInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Resistencia de Uropatógenos en Infecciones de Tracto Urinario en Leon NicaraguaDocument4 pagesResistencia de Uropatógenos en Infecciones de Tracto Urinario en Leon NicaraguaMiguel AnguianoNo ratings yet
- Clinical and Laboratory Differences Between PDFDocument11 pagesClinical and Laboratory Differences Between PDFAli GhufronNo ratings yet
- Erj Pleural TBDocument9 pagesErj Pleural TBmalleshmadeshNo ratings yet
- Varicella-Zoster Virus Detection by Polymerase Chain Reaction Using Bronchoalveolar Lavage SpecimensDocument2 pagesVaricella-Zoster Virus Detection by Polymerase Chain Reaction Using Bronchoalveolar Lavage SpecimensRichel Edwin Theofili PattikawaNo ratings yet
- HPV E6E7 mRNA 1173 PatientDocument9 pagesHPV E6E7 mRNA 1173 PatienthippopotamasNo ratings yet
- Chest X Ray in CAPDocument7 pagesChest X Ray in CAPsahatmanurungNo ratings yet
- PneumocystisDocument10 pagesPneumocystisJESSICA QUISPE HUASCONo ratings yet
- Artigo 02 Geneexpert TBDocument4 pagesArtigo 02 Geneexpert TBpriscila pimentel martinelliNo ratings yet
- Different Roles of Staphylococcus Aureus Enterotoxin in Different Subtypes of Nasal PolypsDocument6 pagesDifferent Roles of Staphylococcus Aureus Enterotoxin in Different Subtypes of Nasal PolypsSiq Febri SmnjtkNo ratings yet
- Validacion CPISDocument5 pagesValidacion CPISXavier AbrilNo ratings yet
- Risk Factors For Extra-Pulmonary Tuberculosis Compared To Pulmonary TuberculosisDocument6 pagesRisk Factors For Extra-Pulmonary Tuberculosis Compared To Pulmonary TuberculosisLily SmithNo ratings yet
- Necrotizing Pneumonia in Cancer Patients A.8Document4 pagesNecrotizing Pneumonia in Cancer Patients A.8Manisha UppalNo ratings yet
- Community-Acquired Lung Respiratory Infections in HIV-infected Patients: Microbial Aetiology and OutcomeDocument11 pagesCommunity-Acquired Lung Respiratory Infections in HIV-infected Patients: Microbial Aetiology and OutcomeMuchamad Nur HadiNo ratings yet
- Acute Pyelonephritis in Adults: A Case Series of 223 PatientsDocument6 pagesAcute Pyelonephritis in Adults: A Case Series of 223 PatientsshiaNo ratings yet
- Extrapulmonary Tuberculosis Comparative Analysis of Diagnostic Modalities Used in A Tertiary Healthcare SettingDocument2 pagesExtrapulmonary Tuberculosis Comparative Analysis of Diagnostic Modalities Used in A Tertiary Healthcare SettingBIOMEDSCIDIRECT PUBLICATIONSNo ratings yet
- Efusi Pleural in MassDocument4 pagesEfusi Pleural in MassRofi IrmanNo ratings yet
- S Stercoralis 30 Casos ClinicosDocument6 pagesS Stercoralis 30 Casos ClinicosYisellNo ratings yet
- Urinary Sediment Microscopy in Acute Kidney Injury Associated With COVID-19Document11 pagesUrinary Sediment Microscopy in Acute Kidney Injury Associated With COVID-19Gabriel Felipe CGNo ratings yet
- AMJ-Volume 50-Issue 2 - Page 1489-1496Document8 pagesAMJ-Volume 50-Issue 2 - Page 1489-1496Pandu Putra Wijaya RestaNo ratings yet
- Img#Document5 pagesImg#AngelNo ratings yet
- Jurnal Anti JamurDocument4 pagesJurnal Anti JamurYusvinaNo ratings yet
- PIIS1473309920301961Document10 pagesPIIS1473309920301961agboxNo ratings yet
- !PORTAL - Wwpob Page - ShowDocument5 pages!PORTAL - Wwpob Page - ShowgamhaelNo ratings yet
- Omi 2017 0070Document13 pagesOmi 2017 0070Heldrian dwinanda SuyuthieNo ratings yet
- Our Experience With Bicytopenia in Patients Treated at The Ankara Hospital Pediatric ClinicDocument5 pagesOur Experience With Bicytopenia in Patients Treated at The Ankara Hospital Pediatric ClinicRonny DoankNo ratings yet
- PCR-based Sepsis@ Quick Test Is Superior in Comparison With Blood Culture For Identification of Sepsis-Causative PathogensDocument7 pagesPCR-based Sepsis@ Quick Test Is Superior in Comparison With Blood Culture For Identification of Sepsis-Causative Pathogensfaraz.mirza1No ratings yet
- Urine Dipstick of Sputum For The Rapid Diagnosis of Community Acquired PneumoniaDocument4 pagesUrine Dipstick of Sputum For The Rapid Diagnosis of Community Acquired PneumoniaStephen JohanNo ratings yet
- Persistence and Complex Evolution of Fluoroquinolone-Resistant Streptococcus Pneumoniae CloneDocument7 pagesPersistence and Complex Evolution of Fluoroquinolone-Resistant Streptococcus Pneumoniae CloneMark ReinhardtNo ratings yet
- CID Evaluation of Laboratory Methods For Diagnosis of VaricellaDocument10 pagesCID Evaluation of Laboratory Methods For Diagnosis of VaricellaK3 KoordinatorNo ratings yet
- Anti-Neutrophil Cytoplasmic Antibody (ANCA) Associated VasculitisFrom EverandAnti-Neutrophil Cytoplasmic Antibody (ANCA) Associated VasculitisRenato Alberto SinicoNo ratings yet
- This Study Resource WasDocument4 pagesThis Study Resource WasDinesh tallaparthiNo ratings yet
- Problem Set 6 Fall 2018 With SolutionsDocument5 pagesProblem Set 6 Fall 2018 With SolutionsrickNo ratings yet
- 03 BodoDocument39 pages03 BodotheaarickNo ratings yet
- Verse 1: @0:11: HappierDocument2 pagesVerse 1: @0:11: HappierKristian GatchalianNo ratings yet
- Tackling Deepfakes in - European PolicyDocument116 pagesTackling Deepfakes in - European PolicyIvan DoriNo ratings yet
- Biometric DevicesDocument10 pagesBiometric DevicesAnonymous rC393RQm5VNo ratings yet
- Present Status and Future Directions Microbiology of Endodontic Infections - 2021Document19 pagesPresent Status and Future Directions Microbiology of Endodontic Infections - 2021bogdimNo ratings yet
- Math 165: Final Exam - Part 1 Fall 2017: Name: Section #Document8 pagesMath 165: Final Exam - Part 1 Fall 2017: Name: Section #Mohammed IbrahimNo ratings yet
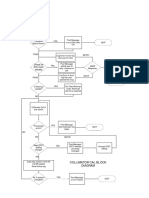
- Check For Dirty Mylar Window: Collimator Cal Block DiagramDocument1 pageCheck For Dirty Mylar Window: Collimator Cal Block DiagramMai Thanh SơnNo ratings yet
- Specification For Aluminum-Alloy Sand Castings: SB-26 /SB-26MDocument17 pagesSpecification For Aluminum-Alloy Sand Castings: SB-26 /SB-26MHernan RiveraNo ratings yet
- Bahasa Inggris Kamilatun Najihah 22610085Document4 pagesBahasa Inggris Kamilatun Najihah 22610085Maria Septiana Uto KeninNo ratings yet
- Practical 2 - Working With Scikit-LearnDocument6 pagesPractical 2 - Working With Scikit-LearnNima DorjiNo ratings yet
- Nit Goa CutoffDocument10 pagesNit Goa CutoffManu KapoorNo ratings yet
- List of Bluesign Approved Chemical Products of TransfarDocument8 pagesList of Bluesign Approved Chemical Products of TransfarMainulHoqueNo ratings yet
- 2-Competitiveness, Strategy, and ProductivityDocument14 pages2-Competitiveness, Strategy, and ProductivityBeepo ZahiaNo ratings yet
- Lab Report 2Document3 pagesLab Report 2Hassan MehmoodNo ratings yet
- AlunsinaDocument2 pagesAlunsinaIzuShiawaseNo ratings yet
- Tesis Salatiga Contoh.Document22 pagesTesis Salatiga Contoh.Bahrul QomarNo ratings yet
- P2 CH 4-8+SM1 Practice Paper - QP3Document12 pagesP2 CH 4-8+SM1 Practice Paper - QP3Thi Hanh Nguyen LeNo ratings yet
- Jessica - Journal (Revisi)Document7 pagesJessica - Journal (Revisi)jessica paulimaNo ratings yet
- Page 3 of 31Document29 pagesPage 3 of 31Septian Nendra SaidNo ratings yet
- Access Modifiers in JavaDocument5 pagesAccess Modifiers in JavaVenu DNo ratings yet
- Hien - Motivational LetterDocument2 pagesHien - Motivational Letterqhuyvu0% (1)
- Karakteristik Film Sinar-X Yang Digunakan Pada RadiologiDocument13 pagesKarakteristik Film Sinar-X Yang Digunakan Pada Radiologifikal 'sNo ratings yet
- 301 enDocument263 pages301 enFedja NetjasovNo ratings yet