CT Imaging • Original Research
Sabir et al.
Perfusion MDCT of Antiangiogenic Therapy Response
CT Imaging
Original Research
Perfusion MDCT Enables Early
Detection of Therapeutic Response
to Antiangiogenic Therapy
Adeel Sabir 1,2 OBJECTIVE. The objective of our study was to determine whether perfusion CT can be
Rachel Schor-Bardach1,2 used to detect early changes in therapeutic response to antiangiogenic therapy in an animal
Carol J. Wilcox 2,3 tumor model.
Syed Rahmanuddin1,2 MATERIALS and methods. Twenty-five rats implanted with R3230 mammary ade-
Michael B. Atkins 2,4 nocarcinoma (diameter, 1.2–2.0 cm) randomly received 7.5 or 30 mg/kg of an antiangiogenic
agent, sorafenib, by daily gavage for 4 (n = 4), 9 (n = 9), or 14 (n = 5) days. Seven untreated animals
Jonathan B. Kruskal2,3
served as a control group. Perfusion MDCT was performed at days 0, 4, 9, and 14 with 0.4 mL of
Sabina Signoretti2,5 ioversol (350 mg/mL) and included four 5-mm slices covering the entire tumor volume. Changes
Vassilios D. Raptopoulos 2,3 in tumor growth were determined by volumetric analysis of CT data. Serial changes in tumor
S. Nahum Goldberg1,2,3 volume and blood flow were assessed and correlated with pathology findings.
RESULTS. All control tumors grew larger (from 2.0 ± 0.7 cm3 at day 0 to 5.9 ± 1.0 cm3 at day
Sabir A, Schor-Bardach R, Wilcox CJ, et al.
14), whereas all treated tumors shrank (from 2.5 ± 1.1 to 2.1 ± 1.0 cm3), with a statistically sig-
Keywords: antiangiogenic therapy, MDCT, perfusion CT,
perfusion imaging, renal cell carcinoma, sorafenib nificant rate of growth or shrinkage in both groups (p < 0.05). Although perfusion in the control
tumors changed little from day 0 to day 14 (day 0, 18.1 ± 9.2 mL/min/100 g; day 4, 15.8 ± 5.6; day
DOI:10.2214/AJR.07.2848 9, 21.7 ± 12.2; day 14, 27.7 ± 34), in the sorafenib group, the mean blood flow was significantly
lower at day 4 (5.2 ± 3.2 mL/min/100 g, 77% decrease), day 9 (6.4 ± 4.0 mL/min/100 g, 66% de-
Received July 10, 2007; accepted after revision
January 10, 2008.
crease), and day 14 (6.3 ± 5.2 mL/min/100 g, 83% decrease) compared with day 0 (23.8 ± 11.6 mL/
min/100 g) (p < 0.05). Poor correlation was seen between changes in blood flow and tumor volume
This study was supported by a grant from the National for days 0–9 (r2 = 0.34), 4–9 (r2 = 0.0004), and 9–14 (r2 = 0.16). However, when comparing day 4
Cancer Institute (NCI) Dana Farber/Harvard Cancer images with days 9 and 14 images, seven of 14 (50%) sorafenib-treated tumors had focal areas of
Center (DF/HCC) Renal Cancer SPORE grant (no. 1 P50
new perfusion that correlated with areas of histopathologic viability despite the fact that these tu-
CA10194-01). Sorafenib (BAY 43-9006) used for this study
was provided by Bayer, Inc., West Haven, CT. mors were shrinking in size from day 4 onward (day 4, 2.18 ± 0.8 cm3; day 9, 1.98 ± 0.8 cm3).
R. Schor-Bardach is a recipient of a fellowship grant from CONCLUSION. Perfusion MDCT can detect focal blood flow changes even when the tumor
The American Physicians Fellowship for Medicine in Israel. is shrinking, possibly indicating early reversal of tumor responsiveness to antiangiogenic therapy.
1
Given that changes in tumor volume after antiangiogenic therapy do not necessarily correlate with
Minimally Invasive Tumor Therapy Laboratory,
Beth Israel Deaconess Medical Center, Harvard Medical
true treatment response, physiologic imaging of tumor perfusion may be necessary.
School, Boston, MA.
T
he treatment of many vascular tu- [6]. Sorafenib has been shown to produce tu-
2
Renal Cancer Program, Dana Farber/Harvard Cancer mors and of renal cell carcinoma mor shrinkage in up to 80% of patients with
Center, Boston, MA.
(RCC) in particular has undergone advanced RCC and to significantly extend me-
3
Department of Radiology, Beth Israel Deaconess a radical change over the past few dian progression-free survival. Despite these
Medical Center, 1 Deaconess Rd., WCC 308-B, Boston, years because of the advent of targeted antian- impressive results, sorafenib does not produce
MA 02215. Address correspondence to S. N. Goldberg giogenic therapies, such as sorafenib, that complete or durable responses and most tu-
(sgoldber@bidmc.harvard.edu).
block signaling through multiple pathways, in- mors become refractory to treatment within
4
Division of Hematology/Oncology, Beth Israel cluding the vascular endothelial growth factor 6–12 months of initiating therapy [5, 7]. The
Deaconess Medical Center, Harvard Medical School, (VEGF) receptor [1–3]. Sorafenib is an oral mechanism of this resistance is poorly un-
Boston, MA. multikinase inhibitor of Raf-1 and is also ac- derstood, but likely includes a component of
5
tive against VEGF receptors 2 and 3, plate- non-VEGF-mediated angiogenic escape [7].
Department of Pathology, Brigham and Women’s
Hospital, Boston, MA.
let-derived growth factor receptor–β, and c- Traditionally, therapeutic response has been
KIT, giving it potent antiangiogenic ability. assessed by serial tumor size measurements,
AJR 2008; 191:133–139 It has shown significant clinical activity in most notably using the Response Evaluation
0361–803X/08/1911–133
patients with advanced renal cancer [4, 5] Criteria in Solid Tumors (RECIST) [8, 9].
and was recently approved by the U.S. Food However, preclinical assessment of new anti-
© American Roentgen Ray Society and Drug Administration for that indication tumoral therapeutics such as antiangiogenic
AJR:191, July 2008 133
Sabir et al.
agents has highlighted the limitations associ- Imaging Research, Massachusetts General Hospi graphy before CT. Tumor size and composition were
ated with using standard morphologic mea- tal, Boston, MA) measuring 1.5 ± 0.2 cm in the also confirmed by CT during experimentation. On
surements. Tumor response may be better z-axis were used for this study. The experimental completion of the study, the animals were sacrificed
assessed by alterations in vascular perfusion group (n = 15) randomly received 7.5 or 30 mg/kg by barbiturate overdose (Somlethal, J. A. Webster)
rather than tumor size, and functional mea- of the antiangiogenic agent sorafenib (BAY according to IACUC guidelines.
surements may therefore be more appropriate 43-9006, Bayer) by gavage for 4 (n = 4), 9 (n = 9),
[10–12]. In addition, resistance to antiangio- or 14 (n = 5) days. Seven untreated animals served Perfusion CT
genic agents appears inevitable, but the nature as the control group. This tumor model was Perfusion MDCT was performed on days 0, 4,
of this resistance or the ability to detect it be- previously used by Hakime et al. [26] to correlate 9, and 14 as described by Hakime et al. [26]. Rats
fore clinically significant disease progression tumor blood flow changes with perfusion MDCT were scanned using a 16-MDCT scanner (Light
occurs remains limited. This situation high- after the administration of an acute blood flow– Speed Plus, GE Healthcare). Before CT, the tail
lights the need to develop alternative methods reducing agent. vein was catheterized with a 24-gauge cannula for
to assess the effects of treatment on tumors. administration of contrast material. After an intra
Given the limitations of clinical criteria Sorafenib Administration peritoneal injection of a mixture of ketamine
alone, various authors have evaluated the use Sorafenib was administered daily by gavage in (Ketaject, Phoenix Pharmaceutica), at a dose of 50
of single-detector CT for the assessment of blinded fashion as 7.5 or 30 mg/kg depending on mg/kg of body weight, and xylazine (Rompun,
tumor blood flow [13–25]. With the aid of reli- experimental group. Sorafenib was dissolved in a Bayer), at a dose of 5 mg/kg, was administered,
able and accurate commercially available 50% polyethoxylated castor oil (Cremophore EL, rats were placed on the CT table and restrained to
software algorithms, they were able to show Sigma)–50% ethanol mixture at four times (4×) limit movement. When necessary, booster anes
good correlations and reproducibility of mea- the desired highest concentration; for the dose of thetic injections at one tenth of those doses were ad
surements, thus establishing the basis for fur- 30 mg/kg, the concentration of the dosing solution ministered intraperitoneally every 30–60 minutes.
ther experimentation and the use of CT func- was 8 mg/mL, with this 4× solution measuring Initially, an unenhanced study was performed
tional measurements. In a more recent study 32 mg/mL. The compounds were heated to 60°C to identify the tumor for planning purposes using
[26], perfusion MDCT achieved a better cor- for 1 minute and sonicated for 20–30 minutes to the following parameters: helical acquisition; slice
relation to the reference standard laser Dop- suspend the sorafenib. Once in solution, the thickness, 2.5 × 2.5 mm; speed, 27 mm/s; pitch,
pler flowmetry compared with a single-detec- aqueous component was gradually added and 1.3; 120 kV; 240 mA; rotation speed, 0.5 second;
tor technique for detecting acute changes in diluted to generate the 1× dosing solution. The scan field of view (FOV), 24 cm; and matrix,
tumor blood flow induced over 1 hour by the lower dose levels were then made by dilution of 512 × 512. The images were then inspected by two
antivascular agent arsenic trioxide in an ani- this preparation with 12.5% Cremophor EL, of the authors on the CT console; the target slices
mal tumor model. In that study, perfusion 12.5% ethanol, and 75% water [1]. Each dose of were selected to plan subsequent dynamic studies
MDCT also showed potential as an indepen- sorafenib was weighed and stored in dry form to ensure that the entire tumor was covered by the
dent predictor of tumor perfusion and im- away from light and was dissolved to liquid form 20-mm scan volume.
provement in the interobserver agreement immediately before administration. For measurement of perfusion, CT was initiated
compared with perfusion imaging using a 2 seconds before the near-instantaneous manual
single-detector CT technique. Tumor Preparation administration of a 0.4-mL bolus of contrast agent
Other authors have also shown that MDCT A parent tumor (≈ 1 cm in diameter) was initially (2 mL/kg of ioversol [Optiray 350, Mallinckrodt
enables assessment of changes in tumor vas- harvested from a live carrier. Within 30 minutes of Imaging] at 0.05 mL/s); contrast injection was
cularity and perfusion that result from chemo- its dissection and removal, the tumor was homo performed consistently by the same investigator to
therapy and radiation therapy [27, 28]. Never- genized with a tissue homogenizer (PowerGen minimize variation. Images were obtained at
theless, use of this technique over the long model 125, Fisher Scientific) using aseptic tech 1-second intervals covering the entire tumor using
time intervals required for monitoring antian- nique, and the tumor cells were suspended in 7 mL the axial mode (120 kV; 240 mA; FOV, 50 cm;
giogenic therapy requires validation. of a culture medium (RPMI 1640, INC Biomedicals). matrix, 512 × 512) throughout the bolus injection
The purpose of this study was therefore to In prior control experiments in our laboratory, this of contrast agent and continued for a total of 65
determine whether perfusion MDCT can be process resulted in a concentration of 1 × 107 cells seconds. The 20-mm scan volume was recon
used to monitor the effects of antiangiogenic per milliliter, with more than 95% cellular viability. structed into four contiguous slices collimated to
therapy to potentially enable earlier prediction During direct visualization, 0.2–0.3 mL of the 5 mm each. Immediately after the dynamic study,
of tumor response and resistance to therapy tumor cell suspension was injected slowly through an the tumor was imaged in the high-resolution mode
compared with conventionally measured im- 18-gauge needle into the mammary fat pad. Animals for calculation of tumor volumes (helical
aging parameters in an animal tumor model. were monitored every 3–4 days to measure tumor acquisition; collimation, 1.0 mm; rotation speed,
growth. Tumors were allowed to grow for 14–24 days 0.5 second; 120 kV; 240 mA; FOV, 24 cm; and
Materials and Methods until the desired treatment size (1.2–2 cm) was matrix, 512 × 512).
Experimental Design achieved. Tumor size was chosen to optimally match
The protocol was approved by the institutional the size with maximum z-axis coverage (4-MDCT Image Processing
animal care and use committee (IACUC) before acquisition at 5-mm thickness = 20 mm). Tumor For each dynamic CT scan acquisition, four
study initiation. Twenty-five female rats (mean induction, monitoring, and randomization were single perfusion CT image maps, each of 5 mm
weight, 150 ± 20 g; age range, 7–9 weeks; Fisher-344 performed by two authors. Tumors were measured thickness, were obtained from the single scanned
rats, Taconic Farms) implanted with R3230 with calipers daily until reaching the desired size. 20-mm tumor volume. The 400 images from the
mammary adenocarcinoma (Center for Molecular Solid tumor architecture was confirmed by sono dynamic studies were processed using perfusion
134 AJR:191, July 2008
Perfusion MDCT of Antiangiogenic Therapy Response
CT software (Perfusion 2.0, GE Healthcare) with sections were stained with H and E. All tissue all mean tumor blood flow was observed be-
a body tumor perfusion algorithm. This software specimens were examined at their greatest axial tween days 4 and 9 and day 14 (p > 0.10). Fur-
has been previously validated for the determination diameter. Nonviable tumor areas were identified thermore, there was no significant difference
of changes to tumor perfusion by various authors using morphologic criteria by an experienced (p > 0.10) between the two different sorafenib
[21–24]. A processing threshold of 0–120 H was pathologist. Four of 18 animals in the experimental doses (7.5 and 30 mg/kg) in terms of mean
selected to permit appropriate subsequent analysis group were exclusively followed to day 4 and were tumor blood flow and the percentage changes
of both unenhanced and enhanced soft tissue. then sacrificed for purposes of histopathologic from baseline.
Arterial input was determined by placing a verification and comparison. Although there was no significant change in
region of interest (ROI) over the best visualized either tumor volume or mean overall blood
artery in the slice plane (aorta, iliac artery, or Statistical Analysis flow when comparing sorafenib-treated day 9
superficial femoral artery). Time–attenuation Serial changes in tumor volume as determined by or day 14 values with day 4 values, seven of 14
curves were automatically generated for the arterial CT were compared with and correlated to mean sorafenib-treated tumors had focal areas of new
input along with perfusion maps for all the tissues tumor blood flow for each of the scan days 0, 4, 9, blood flow that correlated to areas of increased
within the scanning plane over the 65-second and 14. Visual comparison of a histologic tissue histopathologic viability despite the fact that
perfusion acquisition. To determine tumor per section with the corresponding animal’s perfusion these tumors had shrunk or were stable in size
fusion, an ROI was drawn freehand around the CT images was also performed. All values were (day 4, 2.18 ± 0.8 cm3; day 9, 1.98 ± 0.8 cm3).
peripheral margin of the tumor using an electronic expressed as means with SDs. The Student’s t test These foci were seen in four of nine (44%) tu-
cursor. Care was taken to exclude peritumoral skin was used to correlate changes in tumor volume to mors from day 4 to day 9 and in three of five
and fat and intraluminal gas by viewing the cine changes in mean tumor blood flow. A p value of 0.05 (60%) tumors from day 9 to day 14 (Fig. 2).
loop to gauge the extent of movement during was considered to denote statistical significance. Thus, 50% of the sorafenib-treated tumors ex-
acquisition. A global time–attenuation curve for hibited new foci of increased perfusion from
the selected tumor tissue and the mean blood flow Results day 4 onward as seen from spatial analysis of
for the tumor tissue within the ROI were derived. Tumor Volume the individual perfusion CT slices. These new
The blood flow maps of all four single slices of All control tumors (n = 7) increased in vol- foci of increased perfusion were seen on the
a given dynamic CT study were saved in high- ume from their initial baselines values (69% middle two slices of the four slices covering
resolution gray-scale format. Every picture was increase by day 4, 107% increase by day 9, and each tumor in five of seven (71%) tumors and
then loaded in ImageJ (Image Processing and 143% increase by day 14) for the duration of on one of four and three of four slices in the
Analysis in Java, National Institutes of Health the experiment, whereas all treated for 9–14 other two tumors (2/7, 29%).
Image; available at http://rsb.info.nih.gov/ij/) to days (n = 14) decreased in volume to day 9
calculate the histogram of the perfusion values (32% decrease from baseline) with no substan- Histopathologic Correlation
within the ROIs. The pixel data from the four tial change in the rate of tumor volume shrink- Microscopic analysis of tissue sections
tumor slices were then combined in Microsoft age from day 9 to day 14 (Table 1 and Fig. 1). revealed a close correlation between the per-
Excel to calculate the mean CT perfusion for the Accordingly, although there were no statisti- fusion CT blood flow maps and histopatho-
entire tumor volume blood flow. cally significant differences in the baseline tu- logic features (Fig. 3). We observed small
Blood flow in each perfusion map was mor sizes between the control and treatment areas of central necrosis within the control
represented in a color-coding scheme in rainbow groups (p > 0.05), there were significant differ- tumors and larger areas of cell death in every
format such that a flow of 0 mL/min/100 g was ences in the rate of growth or shrinkage com- tumor treated with 4, 9, or 14 days of
shown in black and maximal blood flow (50 mL/ pared with their baseline (day 0) values (p < sorafenib. Based on this analysis, we were
min/100 g) was shown in bright red. Flow values 0.05). Similarly, significant (p < 0.05) differ- able to correlate the color coding of the blood
between 0 and 50 mL/min/100 g were represented ences in the mean tumor volumes between flow maps to the degree of viability of tumor
as varying shades of blue, green, yellow, and red in animals receiving sorafenib and untreated ani- cells. Specifically, a threshold of 2.5 mL/
order of increasing perfusion. mals at each time point were noted. No signifi- min/100 g represented by light blue on the
For calculation of tumor volumes, high- cant differences (p > 0.1) between the high- color map indicated the presence of viable
resolution axial images were loaded as a single dose (30 mg/kg) and low-dose (7.5 mg/kg) cells as seen by microscopic comparison.
volume to the workstation and were reconstructed treatment groups in terms of the rate of change This threshold and color coding correlated
into multiplanar images that were used separately of tumor volume with therapy were detected. well for representing cell viability versus cell
by two authors to draw outlines around the tumor death across both the control group and the
edges. These outlines were used by the software Tumor Blood Flow sorafenib-treated tumors. Moreover, a thres
algorithm to separate the tumor from the main rat Variable, but not statistically significant, hold of 0–1 mL/min/100 g was associated
body and to calculate its volume. changes in mean tumor blood flow (mL/ with the presence of nonviable areas within
min/100 g) were noted for the control group the tumor across both the control group and
Histopathologic Correlation through day 14 (Table 2). However, in the sorafenib-treated tumors.
All animals in the control and experiment sorafenib-treated groups, the mean blood flow
groups were sacrificed on day 0, 4, 9, or 14 after was significantly lower at day 4 (78% decrease Comparison of Tumor Volume and Mean
their last scheduled CT scan. Tumors were sectioned from day 0, p < 0.05) and progressed to an Tumor Blood Flow
immediately (within 1 hour) in the axial plane average decrease of 75% for days 9 and 14 Poor correlation was seen between chang-
corresponding to the CT slice orientation, fixed in compared with day 0 (p < 0.05). However, no es in blood flow and tumor volume for days
10% formalin, and embedded in paraffin. Tissue statistically significant difference in the over- 0–9 (r 2 = 0.34), 4–9 (r 2 = 0.0004), and 9–14
AJR:191, July 2008 135
Sabir et al.
TABLE 1: Changes in Volume for Control and Sorafenib-Treated R3230 Tumors
Tumor Volume
Day 4 Day 9 Day 14
No. of Day 0 % % %
Group Rats (Mean ± SD) (cm3) Mean ± SD (cm3) Changea Mean ± SD (cm3) Changea Mean ± SD (cm3) Changea
Control 7 2.0 ± 0.7 3.5 ± 1.5 69 4.3 ± 1.8 107 5.9 ± 1.0 143
Sorafenib (all rats) 14 2.5 ± 1.1 1.9 ± 1.0 –24 1.7 ± 0.8 –32 2.1 ± 1.0 –31
Sorafenib (all rats, days 0–9) 9 2.3 ± 1.2 1.7 ± 1.0 –23 1.5 ± 0.80 –32 — —
High dose 4 1.7 ± 0.8 1.7 ± 1.0 –5 1.4 ± 0.6 –14 — —
Low dose (days 0–9) 5 2.7 ± 1.4 1.8 ± 1.2 –37 1.5 ± 1.0 –47 — —
Low dose (days 0–14) 5 2.9 ± 0.8 2.2 ± 0.8 –26 2.0 ± 0.8 –33 2.1 ± 1.0 –31
Note—Percentage change is reported for the mean as compared to baseline (day 0). As a rule, control tumors consistently increased in volume whereas the sorafenib-
treated tumors decreased in volume. Dash (—) indicates not applicable.
aPercentage change values represent the mean of changes calculated on an animal-by-animal basis, not the percent change of the means.
(r 2 = 0.16). Thus, we were unable to establish Discussion genic therapy in a well-established and well-
a clear-cut pattern of increase or decrease in We evaluated the use of perfusion MDCT studied animal tumor model. CT has emerged
blood flow, tumor volume, or both correlat- as an alternative means of determining the recently as a means of rapid, noninvasive as-
ing with progression at 14 days of therapy. blood flow changes associated with antiangio- sessment not only of anatomy, but also of
physiology, as is evident in its ability to reli-
ably measure blood flow [13, 14, 26]. MDCT
is fast, economical, and widely available, all
of which contribute to its enormous potential
in revolutionizing the care of patients with
cancer, particularly those who receive antian-
giogenic agents such as sorafenib.
Hakime et al. [26] previously showed the
superiority of MDCT to single-detector CT
for measuring tumor blood flow, as evidenced
by its higher interobserver agreement and
greater tumor volume coverage. Our study
results further point to the fact that the cur-
rently available systems of tumor monitor-
ing, such as RECIST, alone cannot be en-
tirely relied on when using agents that reduce
tumor blood flow because changes in blood
flow may precede changes in tumor size. Our
A B findings also reveal that a set of tumors re-
ceiving the antiangiogenic agent sorafenib
can exhibit differences in response to that
agent over time, which can range from
changes in mean tumor blood flow to devel-
opment of new zones of perfusion in areas
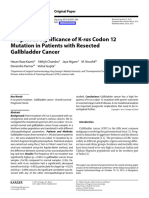
Fig. 1—Perfusion MDCT maps of control group
tumors (outlined regions and arrows) show
progressive increase in size, volume, and blood flow
from days 0–14.
A–D, Images obtained at days 0 (A), 4, (B), 9 (C),
and 14 (D). Blood flow in each perfusion map is
represented in color-coding scheme in rainbow
format such that flow of 0 mL/min/100 g is shown in
black and maximal blood flow (50 mL/min/100 g) is
shown in bright red. Flow values between 0 and 50
mL/min/100 g are represented as varying shades of
blue, green, yellow, and red in order of increasing
perfusion.
C D
136 AJR:191, July 2008
Perfusion MDCT of Antiangiogenic Therapy Response
that initially showed minimal or no blood spond to focal areas of viable tumor and may ther emphasizes the importance of covering
flow. We found that these foci of new perfu- well represent the development of new ves- large volumes of the tumor with MDCT
sion can develop and be detected by perfu- sels that occur despite the administration of techniques to maximize diagnostic sensitiv-
sion CT even when mean tumor blood flow is the antiangiogenic agent, indicating the ity. An alternative approach could be to scan
unchanged or while tumor size or volume is emergence of cells that have developed a and calculate the blood flow in the middle
actively decreasing, greatly emphasizing the means of resistance to the therapeutic agent. two slices (center part) of the tumor only in
importance of perfusion MDCT in such a Furthermore, the fact that the zones of new cases in which full tumor volume coverage is
scenario. Such zones of blood flow corre- perfusion were not seen in every image fur- not possible. In addition, perfusion CT will
TABLE 2: Mean Tumor Blood Flow Values for Control and Sorafenib-Treated R3230 Tumors
Blood Flow
Day 4 Day 9 Day 14
Day 0
No. of (Mean ± SD) Mean ± SD % Mean ± SD % Mean ± SD %
Group Rats (mL/min/100 g) (mL/min/100 g) Changea (mL/min/100 g) Changea (mL/min/100 g) Changea
Control 7 18.1 ± 9.2 15.8 ± 5.6 –13 21.7 ± 12.2 20 27.7 ± 34 78
Sorafenib (all rats) 14 23.8 ± 11.6 5.2 ± 3.2 –78 6.4 ± 4.0 –66 6.3 ± 5.2 –83
Sorafenib (all rats, days 0–9) 9 16.8 ± 6.6 4.0 ± 2.4 –75 6.3 ± 4.6 –60 — —
High dose 4 17.6 ± 6.0 3.1 ± 2.3 –82 4.4 ± 2.0 –75 — —
Low dose (days 0–9) 5 16.2 ± 7.7 4.7 ± 2.5 –70 7.9 ± 5.7 –48 — —
Low dose (days 0–14) 5 34.3 ± 9.4 7.3 ± 3.4 –80 5.4 ± 4.0 –78 5.3 ± 5.3 –83
Note—Percentage change is reported for the mean as compared to baseline (day 0). As a rule, control tumors maintained their blood flow whereas the sorafenib-treated
tumors showed marked decrease in mean tumor blood flow that remained stable from day 9 onward into therapy. Dash (—) indicates not applicable.
aPercentage change values represent the mean of changes calculated on an animal-by-animal basis, not the percent change of the means.
A B C
D E F
Fig. 2—Perfusion CT maps of two rats from sorafenib-treated group show decrease in tumor volume and blood flow from days 0–9.
A–F, Maps of rat 1 (A–C) and rat 2 (D–F) at days 0 (A and D), 4 (B and E), and 9 (C and F). Blood flow in each perfusion map is represented in color-coding scheme in
rainbow format such that flow of 0 mL/min/100 g is shown in black and maximal blood flow (50 mL/min/100 g) is shown in bright red. Flow values between 0 and 50 mL/
min/100 g are represented as varying shades of blue, green, yellow, and red in order of increasing perfusion. In addition, these figures show development of rim of
increased perfusion (arrows, C and F) in sorafenib-treated tumors despite continued decrease in tumor volume. This could possibly represent early development of tumor
resistance to antiangiogenic therapy.
AJR:191, July 2008 137
Sabir et al.
4. This, combined with the limited number
of rats available, led to an experimental de-
sign that did not sacrifice control animals on
days 0 and 4.
Inevitably, although rodent studies allow
minimization of variability of tumor parame-
ters, the size of the model may introduce un-
toward errors in the imaging technique. For
example, perfusion CT is likely to work best
with a tight injection bolus. Nevertheless, by
necessity, we used a near-instantaneous man-
ual bolus of 0.4 mL of contrast material, as
done in previous published studies [26]. Even
though a constant injection rate using a power
injector is perhaps the ideal method, to the
best of our knowledge, there is no power in-
jector commercially available for use in the
tail vein of a 150-g rat. Furthermore, although
rats were positioned almost identically every
Fig. 3—Histopathologic correlation (right) of sorafenib-treated tumor with CT map (left). Areas of increased time they were scanned, this position change
and decreased or absent blood flow (yellow arrows) on perfusion images correspond to viable and nonviable
tumor areas (black arrows), respectively, on tissue section. might have led to variability in tumor volume
measurements for such small tumors. How-
ever, unpublished data from our laboratory
ultimately need to be compared with other points or concerns. Furthermore, Kan et al. show that repeated volume CT scans of the
imaging strategies for mapping perfusion [13] have shown that “functional CT can help same rat tumor with the rat in varying posi-
such as arterial spin-labeling MRI [29] and quantify the perfusion function of mature tions (prone, supine, lateral, and prone again)
dynamic contrast-enhanced Doppler sonog- vessels but not changes in microvessel density have average variability in calculated tumor
raphy [30]. in antiangiogenic therapy.” Perfusion CT of volumes of 1.0% ± 0.5% (range, –1.9% to
Perfusion MDCT was able to successfully thoracic and abdominal tumors may be lim- 1.2%). Accordingly, this degree of error is
identify focal areas of new tumor perfusion ited by breathing motion; nonetheless, previ- way below the changes in tumor volume ob-
9–14 days into antiangiogenic therapy before ous studies [26] using similar techniques and served in this study.
clinically measurable changes in tumor mass an animal model have shown the accuracy of Lastly, some authors have used additional
were seen, perhaps indicating early angio- perfusion CT compared with an established perfusion CT calculation parameters such as
genic escape in this specific animal tumor reference standard. Future advances in imag- blood volume, mean transit time, and perme-
model. However, not all tumors may behave ing software and technology will help to fur- ability surface area for determination of a
in an equal manner with antiangiogenic ther- ther optimize image acquisition and process- tumor’s vascularity in varying tumor models
apy, and thus further experimentation in ing with lower radiation doses. [31, 32]. However, studies from our labora-
other animal, and more importantly human, Several potential limitations in our animal tory [26] have clearly shown tight correlation
tumor models is needed to validate the ef- model and experimental design warrant dis- between blood flow as measured by perfu-
fectiveness of perfusion MDCT for this spe- cussion. Like most other scientific measure- sion MDCT and laser Doppler flowmetry as
cific purpose. Thus, specific clinical testing ment systems, perfusion CT has room for the reference standard in the same animal
in RCC, a disease that is known to be sensi- variation, particularly for heterogeneous bio- model. Thus, we preferentially used this pa-
tive to sorafenib, would be of interest and logic systems such as orthotopic tumors. For rameter over those with which poorer corre-
may or may not reproduce these findings. example, we note that there was a 13% drop lations (unpublished data) were found. More-
Although we were able to correlate the mi- in blood flow in the control rats on day 4 over, various authors have clearly shown that
croscopy findings with the perfusion CT compared with their baseline values, but this of all the commonly calculated perfusion CT
maps to within reasonable limits, our study is decrease is well below the reported coeffi- parameters (i.e., blood flow, blood volume,
limited by the resolution and slice thickness cient of variability in perfusion CT measure- mean transit time, and permeability surface
used for calculating tumor blood flow. This ments [18, 20, 29]. Furthermore, we did not area product), blood flow shows the closest
can be overcome in future studies by the sacrifice control rats on days 0 and 4 for this correlation to histopathology findings and
availability of software that allows higher- study. However, prior experiments in our clinical outcomes [13, 31, 32].
resolution scanning and use of thinner slices, laboratory [26] using the exact same animal If successfully validated, perfusion MDCT
thus enabling tighter correlation with histo- tumor model have shown that untreated could be used to further characterize the
pathology results. As an additional limitation, R3230 tumors of similar sizes have excellent phenomenon of “early breakthrough” in
we relied on conventional histologic criteria solidity and vascularity as indicated by ra- large-scale trials in patients with highly vas-
of cellular viability rather than microvascular diologic–pathologic correlation. Moreover, cular tumors such as RCC, thus enabling us
density. Nevertheless, tumor growth and via- our end point was to determine the vascular- to gain more insight into the physiology and
bility, not angiogenesis, are the primary end ity of the tumors at days 9 and 14, not at day pathogenesis of resistant tumor cells. Earlier
138 AJR:191, July 2008
Perfusion MDCT of Antiangiogenic Therapy Response
identification of resistance through measure- 2005/new01282.html. Accessed March 9, 2007 TY. A CT method to measure hemodynamics in
ment of blood flow would enable clinicians 7. Sosman JA, Puzanov I, Atkins MB. Opportunities brain tumors: validation and application of cere-
to consider an alteration in therapy, including and obstacles to combination targeted therapy in bral blood flow maps. Am J Neuroradiol 2000;
dose or schedule modifications or switching renal cell cancer. Clin Cancer Res 2007; 13(2 Pt 21:462–470
to another agent before tumor growth is doc- 2):764S–769S 21. Purdie TG, Henderson E, Lee TY. Functional CT
umented, possibly preventing or delaying 8. World Health Organization. WHO handbook for imaging of angiogenesis in rabbit VX2 soft-tissue
clinical sequelae of disease progression. reporting results of cancer treatment. Geneva, tumor. Phys Med Biol 2001; 46:3161–3175
Moreover, tumors exhibiting this phenome- Switzerland: World Health Organization, 1979: 22. Gillard JH, Antoun NM, Burnet NG, Pickard JD.
non could then be easily singled out for tar- WHO offset publication no. 48 Reproducibility of quantitative CT perfusion im-
geted biopsy and extraction of the resistant 9. Therasse P, Arbuck SG, Eisenhauer EA, et al. aging. Br J Radiol 2001; 74:552–555
cells, which can be biochemically and ge- New guidelines to evaluate the response to treat- 23. Tsushima Y, Funabasama S, Aoki J, Sanada S,
netically studied to understand and identify ment in solid tumors. European Organization for Endo K. Quantitative perfusion map of malignant
the exact resistance mechanism or mecha- Research and Treatment of Cancer, National Can- liver tumors, created from dynamic computed to-
nisms, thus enabling future development of cer Institute of the United States, National Cancer mography data. Acad Radiol 2004; 11:215–223
targeted therapies. Institute of Canada. J Natl Cancer Inst 2000; 24. Tsushima Y, Unno Y, Koizumi J, Kusano S. He-
In conclusion, in this murine xenograft tu- 92:205–216 patic perfusion changes after transcatheter arteri-
mor model receiving antiangiogenic therapy, 10. Li WW. Tumor angiogenesis: molecular patholo- al embolization (TAE) of hepatocellular carcino-
perfusion MDCT was able to identify chang- gy, therapeutic targeting and imaging. Acad Ra- ma: measurement by dynamic computed
es in tumor blood flow before changes in tu- diol 2000; 7:800–811 tomography (CT). Dig Dis Sci 1998; 43:317–322
mor volume occurred, possibly indicating 11. Grosios K, Holwell SE, McGown AT, Pettit GR, 25. Lin WY, Wang SJ, Yeh SH. Hepatic perfusion in-
early reversal of tumor responsiveness to Bibby MC. In vivo and in vitro evaluation of com- dex in evaluating treatment effect of transcatheter
therapy. Given that changes in tumor volume bretastatin A-4 and its sodium phosphate prodrug. hepatic artery embolization in patients with hepa-
after antiangiogenic therapy do not necessar- Br J Cancer 1999; 81:1318–1327 tocellular carcinoma. Neoplasma 1995; 42:89–92
ily correlate with true treatment response, 12. Chaplin DJ, Pettit GR, Hill SA. Anti-vascular ap- 26. Hakime A, Peddi H, Hines-Peralta AU, et al. CT
noninvasive physiologic imaging of tumor proaches to solid tumor therapy: evaluation of perfusion for determination of pharmacologically
perfusion may be necessary for evaluating combretastatin A4 phosphate. Anticancer Res mediated blood flow changes in an animal tumor
the effectiveness of antiangiogenic agents. 1999; 19:189–195 model. Radiology 2007; 243:712–719
13. Kan Z, Phongkitkarun S, Kobayashi S, et al. 27. Sahani DV, Kalva SP, Hamberg LM, et al. Assess-
References Functional CT for quantifying tumor perfusion in ing tumor perfusion and treatment response in
1. Wilhelm SM, Carter C, Tang L, et al. BAY antiangiogenic therapy in a rat model. Radiology rectal cancer with multisection CT: initial obser-
43-9006 exhibits broad spectrum oral antitumor 2005; 237:151–158 vations. Radiology 2005; 234:785–792
activity and targets the RAF/MEK/ERK pathway 14. Lee TY, Purdie TG, Stewart E. CT imaging of an- 28. Meijerink MR, van Cruijsen H, Hoekman K, et al.
and receptor tyrosine kinases involved in tumor giogenesis. Q J Nucl Med 2003; 47:171–187 The use of perfusion CT for the evaluation of
progression and angiogenesis. Cancer Res 2004; 15. Kan Z, Kobayashi S, Phongkitkarun S, Charnsan- therapy combining AZD2171 with gefitinib in
64:7099–7109 gavej C. Functional CT quantification of tumor cancer patients. Eur Radiol 2007; 17:1700–1713
2. Flaherty KT. Sorafenib in renal cell carcinoma. perfusion after transhepatic arterial embolization 29. De Bazelaire C, Rofsky NM, Duhamel G, Mi-
Clin Cancer Res 2007; 13(2 Pt 2):747S–752S in a rat model. Radiology 2005; 237:144–150 chaelson MD, George D, Alsop DC. Arterial spin
3. Hutson TE, Sonpavde G, Galsky MD. Targeting 16. Fournier LS, Cuenod CA, de Bazelaire C, et al. labeling blood flow magnetic resonance imaging
growth factor and antiangiogenic pathways in Early modifications of hepatic perfusion mea- for the characterization of metastatic renal cell
clear-cell renal cell carcinoma: rationale and on- sured by functional CT in a rat model of hepato- carcinoma (1). Acad Radiol 2005; 12:347–357
going trials. Clin Genitourin Cancer 2006; cellular carcinoma using a blood pool contrast 30. Lamuraglia M, Escudier B, Chami L, et al. To
5[suppl 1]:S31–S39 agent. Eur Radiol 2004; 14:2125–2133 predict progression-free survival and overall sur-
4. Ratain MJ, Eisen T, Stadler WM, et al. Phase II 17. Willett CG, Boucher Y, Di Tomaso E, et al. Direct vival in metastatic renal cancer treated with
placebo-controlled randomized discontinuation evidence that the VEGF-specific antibody bevaci- sorafenib: pilot study using dynamic contrast-
trial of sorafenib in patients with metastatic renal zumab has antivascular effects in human rectal enhanced Doppler ultrasound. Eur J Cancer
cell carcinoma. J Clin Oncol 2006; 24: 2505– cancer. Nat Med 2004; 10:145–147 2006; 42:2472–2479 [Erratum in Eur J Cancer
2512 18. Nabavi DG, Cenic A, Dool J, et al. Quantitative 2007; 43:1336]
5. Escudier B, Eisen T, Stadler WM, et al.; TAR- assessment of cerebral hemodynamics using CT: 31. Sahani DV, Holalkere NS, Mueller PR, Zhu AX.
GET Study Group. Sorafenib in advanced clear- stability, accuracy, and precision studies in dogs. J Advanced hepatocellular carcinoma: CT perfu-
cell renal-cell carcinoma. N Engl J Med 2007; Comput Assist Tomogr 1999; 23:506–515 sion of liver and tumor tissue—initial experience.
356:125–134 [erratum in N Engl J Med 2007; 19. Nabavi DG, Cenic A, Craen RA, et al. CT assess- Radiology 2007; 243:736–743
357:203] ment of cerebral perfusion: experimental valida- 32. Hermans R, Lambin P, Van der Goten A, et al.
6. FDA approves new treatment for advanced kidney tion and initial clinical experience. Radiology Tumoural perfusion as measured by dynamic
cancer. FDA News. P05-107. Published December 1999; 213:141–149 computed tomography in head and neck carcino-
20, 2005. http://www.fda.gov/bbs/topics/news/ 20. Cenic A, Nabavi DG, Craen RA, Gelb AW, Lee ma. Radiother Oncol 1999; 53:105–111
AJR:191, July 2008 139
You might also like
- Algorithm-PALS Ped Systematic Approach 200615Document1 pageAlgorithm-PALS Ped Systematic Approach 200615Erica Yamamoto100% (2)
- Hospital Performance IndicatorsDocument34 pagesHospital Performance IndicatorsSangaThamizhanNo ratings yet
- ACOG Fecal Incontinence.2019Document14 pagesACOG Fecal Incontinence.2019linaNo ratings yet
- Department of A HospitalDocument24 pagesDepartment of A HospitalAnonymous YcdK9FWtH100% (2)
- DCE and DW-MRI Monitoring of Vascular Disruption Following VEGF-Trap Treatment of A Rat Glioma ModelDocument22 pagesDCE and DW-MRI Monitoring of Vascular Disruption Following VEGF-Trap Treatment of A Rat Glioma ModelDong DongNo ratings yet
- A Phase I Trial of Stereotactic Body Radiation TherapyDocument8 pagesA Phase I Trial of Stereotactic Body Radiation TherapyRaul Matute MartinNo ratings yet
- 1 s2.0 S1470204522007835 Main PDFDocument11 pages1 s2.0 S1470204522007835 Main PDFOncología CdsNo ratings yet
- Meddos Published ArticleDocument6 pagesMeddos Published Articleapi-350437453No ratings yet
- Provenge 2Document12 pagesProvenge 2api-675909478No ratings yet
- 1 s2.0 S245210942100097X MainDocument7 pages1 s2.0 S245210942100097X MainhidayatullahhaqyaarNo ratings yet
- Paper 1Document11 pagesPaper 1บอส เลิศเกียรติรัชตะNo ratings yet
- Journal Pre-Proof: International Journal of Radiation Oncology, Biology, PhysicsDocument42 pagesJournal Pre-Proof: International Journal of Radiation Oncology, Biology, PhysicsMilan JovicNo ratings yet
- Clinical InvestigationDocument9 pagesClinical InvestigationOncología CdsNo ratings yet
- Of March 15, 2024. This Information Is Current As K.M. Schmainda, M.A. Prah, Z. Zhang, B.S. Snyder, S.DDocument9 pagesOf March 15, 2024. This Information Is Current As K.M. Schmainda, M.A. Prah, Z. Zhang, B.S. Snyder, S.DAhana MukherjeeNo ratings yet
- Dedifferentiated Chondrosarcoma: The Emerging Role of IDH Mutations in ChondrosarcomaDocument3 pagesDedifferentiated Chondrosarcoma: The Emerging Role of IDH Mutations in ChondrosarcomaAlina LazarNo ratings yet
- Jco 2016 71 7397Document9 pagesJco 2016 71 7397brasilianaraNo ratings yet
- Kapoor SchwannomaDocument7 pagesKapoor SchwannomaAna Clara Nunes SartoriNo ratings yet
- Livsey 2003Document6 pagesLivsey 2003Migue PerezNo ratings yet
- Article. Neoadjuvant Treatment Response As An Early Response Indicator For Patients With Rectal CancerDocument7 pagesArticle. Neoadjuvant Treatment Response As An Early Response Indicator For Patients With Rectal CancerTrí Cương NguyễnNo ratings yet
- The Role of Hypofractionated Radiotherapy in ProstDocument10 pagesThe Role of Hypofractionated Radiotherapy in ProstАнастасия АнохинаNo ratings yet
- 4770 FullDocument7 pages4770 FullEnes ÇakmakNo ratings yet
- Exercise Prehabilitation During Neoadjuvant Chemotherapy May EnhanceDocument15 pagesExercise Prehabilitation During Neoadjuvant Chemotherapy May EnhanceThiago SartiNo ratings yet
- Analysis of Compliance, Toxicity and Survival WeeklyDocument11 pagesAnalysis of Compliance, Toxicity and Survival Weeklydanu20No ratings yet
- Articulo Sesion 2 DMII 2023 Karapetis2008Document9 pagesArticulo Sesion 2 DMII 2023 Karapetis2008abcd 1234No ratings yet
- Annals of Medicine and SurgeryDocument6 pagesAnnals of Medicine and SurgeryAbbyAbbsNo ratings yet
- Genética Clínica 2Document10 pagesGenética Clínica 2Victor MarquesNo ratings yet
- 05 - LaceBio KrasTsize JThoracOncol2012Document26 pages05 - LaceBio KrasTsize JThoracOncol2012Omar SettiNo ratings yet
- EeDocument8 pagesEeEstiPramestiningtyasNo ratings yet
- Dose-Fractionation Sensitivity of Prostate Cancer Deduced From Radiotherapy Outcomes of 5969 Patients y Seven International Insttutional DatasetDocument8 pagesDose-Fractionation Sensitivity of Prostate Cancer Deduced From Radiotherapy Outcomes of 5969 Patients y Seven International Insttutional DatasetrgergerNo ratings yet
- Nejmoa 0908721Document9 pagesNejmoa 0908721Gustavo BraccoNo ratings yet
- Huang 2010Document11 pagesHuang 2010OZGE DENIZ YESILNo ratings yet
- Head-to-Head Comparison of Subcutaneous Abatacept Versus Adalimumab For Rheumatoid ArthritisDocument11 pagesHead-to-Head Comparison of Subcutaneous Abatacept Versus Adalimumab For Rheumatoid ArthritislilingNo ratings yet
- 1 s2.0 S1936523312800143 MainDocument7 pages1 s2.0 S1936523312800143 MainIsrael Arias GonzálezNo ratings yet
- Healthcare 07 00120Document9 pagesHealthcare 07 00120Ryantino IrdanNo ratings yet
- Enhanced Efficacy of Sitravatinib in Metastatic Models of Antiangiogenic Therapy Resistance.Document2 pagesEnhanced Efficacy of Sitravatinib in Metastatic Models of Antiangiogenic Therapy Resistance.Arturo Martí-CarvajalNo ratings yet
- Association Between Statin Use and The Prognosis of Hepatocell - 2023 - EclinicaDocument11 pagesAssociation Between Statin Use and The Prognosis of Hepatocell - 2023 - Eclinicaronaldquezada038No ratings yet
- Reuter 2010Document8 pagesReuter 2010Hector Javier BurgosNo ratings yet
- tmpDC1A TMPDocument43 pagestmpDC1A TMPFrontiersNo ratings yet
- Inhibition of Vascular Endothelial Growth Factor VDocument10 pagesInhibition of Vascular Endothelial Growth Factor VDong DongNo ratings yet
- Sutent GistDocument10 pagesSutent Gistapi-26302710No ratings yet
- Trifiletti Et AlDocument22 pagesTrifiletti Et AlsuanjayaNo ratings yet
- CrizotinibDocument10 pagesCrizotinibLuca StamerraNo ratings yet
- Ournal of Linical Ncology: PurposeDocument7 pagesOurnal of Linical Ncology: PurposeIvor Wiguna Hartanto WilopoNo ratings yet
- 10 1111@codi 15424Document22 pages10 1111@codi 15424yongky sugandaNo ratings yet
- New Evidence For Managing Gram-Negative Bloodstream InfectionsDocument12 pagesNew Evidence For Managing Gram-Negative Bloodstream Infectionsjhon edisson dueñas ariasNo ratings yet
- Expert Consensus Contouring Guidelines For Intensity Modulated Radiation Therapy in Esophageal and Gastroesophageal Junction CancerDocument10 pagesExpert Consensus Contouring Guidelines For Intensity Modulated Radiation Therapy in Esophageal and Gastroesophageal Junction CancermarrajoanaNo ratings yet
- Glynne Jones2015Document3 pagesGlynne Jones2015Robert ChristevenNo ratings yet
- 1999 - Duchesne, Peters - What Is The Alphabeta Ratio For Prostate Cancer Rationale For Hypofractionated High-Dose-Rate BrachytherapyDocument2 pages1999 - Duchesne, Peters - What Is The Alphabeta Ratio For Prostate Cancer Rationale For Hypofractionated High-Dose-Rate BrachytherapyPoljarLijanNo ratings yet
- 10 1016@j Critrevonc 2020 102962Document16 pages10 1016@j Critrevonc 2020 102962bouh aichetouNo ratings yet
- 9 ErDocument13 pages9 Ermartin Ignacio Zapata LaguadoNo ratings yet
- Cesium 131 Prostate BrachytherapyDocument7 pagesCesium 131 Prostate BrachytherapyPablo Del PozoNo ratings yet
- RRP Radical ProstatectomyDocument6 pagesRRP Radical ProstatectomybojanvuckovicNo ratings yet
- Nodal - Multi-Institut Oligo - Plus COREDocument13 pagesNodal - Multi-Institut Oligo - Plus COREsilviuNo ratings yet
- Expression of Survivin mRNA in Gallbladder Cancer - A Diagnostic and Prognostic Marker 1.29.38 PMDocument6 pagesExpression of Survivin mRNA in Gallbladder Cancer - A Diagnostic and Prognostic Marker 1.29.38 PMJaya Kunal DubeyNo ratings yet
- Prognostic Significance of K - Ras Codon 12 Mutation in Resected GBC 1.29.44 PMDocument7 pagesPrognostic Significance of K - Ras Codon 12 Mutation in Resected GBC 1.29.44 PMJaya Kunal DubeyNo ratings yet
- Metformin Inhibits Metastatic Breast Cancer Progression and Improves Chemosensitivity by Inducing Vessel Normalization Via PDGF-B DownregulationDocument17 pagesMetformin Inhibits Metastatic Breast Cancer Progression and Improves Chemosensitivity by Inducing Vessel Normalization Via PDGF-B DownregulationJackson HakimNo ratings yet
- Determination of Prostate VolumeDocument6 pagesDetermination of Prostate VolumeChristian ToalongoNo ratings yet
- Allen2021 Article ChemotherapyVersusChemotherapyDocument8 pagesAllen2021 Article ChemotherapyVersusChemotherapyXavier QuinteroNo ratings yet
- Wyatt 2002Document18 pagesWyatt 2002mod_naiveNo ratings yet
- 2017 Article 3322Document7 pages2017 Article 3322Kevin MandakNo ratings yet
- Cook2011 Article TheDiagnosticUtilityOfTheFlareDocument7 pagesCook2011 Article TheDiagnosticUtilityOfTheFlare蘇柏霖No ratings yet
- Strouthos 2017Document8 pagesStrouthos 2017Evelynππ θσυNo ratings yet
- Ni Hms 935657Document15 pagesNi Hms 935657AHMAD FUDHAIL AHMAD ZAKINo ratings yet
- Adaptative RT For Prostate Cancer Using KV CBCT - Jasper NijkampDocument8 pagesAdaptative RT For Prostate Cancer Using KV CBCT - Jasper NijkampMarcos sajcabunNo ratings yet
- Laboratory Discussion: MLS 2309 Clinical BacteriologyDocument3 pagesLaboratory Discussion: MLS 2309 Clinical Bacteriologycarina smithNo ratings yet
- Note On Cardiopulmonary Physiotherapy PDFDocument16 pagesNote On Cardiopulmonary Physiotherapy PDFTsz Kwan CheungNo ratings yet
- Thoracic Trauma: Dr. Bareera AmjadDocument45 pagesThoracic Trauma: Dr. Bareera AmjadMuhammad MuaazNo ratings yet
- Pain Pathways IntroductionDocument7 pagesPain Pathways Introductionganpur01100% (1)
- Pediatric Q&ADocument12 pagesPediatric Q&AMateen ShukriNo ratings yet
- HERNIA - Case StudyDocument8 pagesHERNIA - Case StudyMa Jaimeliz Mae MuñizNo ratings yet
- Cellular AberrationDocument6 pagesCellular Aberrationirene gomez100% (1)
- Andrology - 2017 - Semet - The Impact of Drugs On Male Fertility A ReviewDocument24 pagesAndrology - 2017 - Semet - The Impact of Drugs On Male Fertility A ReviewAbhishek RampalNo ratings yet
- Test 6Document4 pagesTest 6xIcExNo ratings yet
- Advocacy LetterDocument5 pagesAdvocacy Letterapi-381362041No ratings yet
- Symptoms: What Is Dyspepsia?Document4 pagesSymptoms: What Is Dyspepsia?Ratna Widya SariNo ratings yet
- Analgesics - Uses, Treatment, RisksDocument5 pagesAnalgesics - Uses, Treatment, RisksHonour JamesNo ratings yet
- Preanalytical Variables Influence On Laboratory Results and Patient CareDocument4 pagesPreanalytical Variables Influence On Laboratory Results and Patient Caredarko_600054071No ratings yet
- 2010 Goh Vulnera - EngDocument5 pages2010 Goh Vulnera - EngFernandoCedroNo ratings yet
- 2222 PDFDocument700 pages2222 PDFlaaaallaaNo ratings yet
- Patterson's Allergic Diseases (6ed, 2002) (509s)Document509 pagesPatterson's Allergic Diseases (6ed, 2002) (509s)gonzalophNo ratings yet
- PRUBSN Heatlh Enrich PlusDocument2 pagesPRUBSN Heatlh Enrich PlusMalik TaufiqNo ratings yet
- LM PotencyDocument9 pagesLM PotencyNisha JoshiNo ratings yet
- Checklist 7 Step of Occupational Diagnosis - 2021-2022Document4 pagesChecklist 7 Step of Occupational Diagnosis - 2021-2022Putri NoviyantiNo ratings yet
- The Origin of SARS-CoV-2Document10 pagesThe Origin of SARS-CoV-2habomuninNo ratings yet
- Grade 8 Chapter I II FinalDocument9 pagesGrade 8 Chapter I II FinalDenmier OldscoNo ratings yet
- RUHS Pre D.M.medical Gastroenterology Entrance Exam Question Paper 2014Document17 pagesRUHS Pre D.M.medical Gastroenterology Entrance Exam Question Paper 2014narasimhahanNo ratings yet
- Drug Name Dosage, Route, Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesDocument1 pageDrug Name Dosage, Route, Frequency Mechanism of Action Indication Contraindication Adverse Effect Nursing ResponsibilitiesJonna Mae TurquezaNo ratings yet
- Diabetes CaseDocument2 pagesDiabetes CaseRuss RochaNo ratings yet
- The Nose, Upper Airway, and Obstructive Sleep ApneaDocument7 pagesThe Nose, Upper Airway, and Obstructive Sleep ApneaDaniel Celestino DiazNo ratings yet
- Ob/Gyn Instruments: Done byDocument30 pagesOb/Gyn Instruments: Done byDrHassan Ahmed ShaikhNo ratings yet