You might also like
- Drug ListDocument127 pagesDrug Listnehal choudharyNo ratings yet
- N202669852876 Template012 131071016 09 22 2020 05 19 17 ENDocument8 pagesN202669852876 Template012 131071016 09 22 2020 05 19 17 ENmaraki2012No ratings yet
- Reg 2-Primary Care Claim Form-31 Oct 2008Document2 pagesReg 2-Primary Care Claim Form-31 Oct 2008Pradeep KhubchandaniNo ratings yet
- Cameron Handbook - TA3000 Product Manual Rev 4Document141 pagesCameron Handbook - TA3000 Product Manual Rev 4mongojerry75% (4)
- ItaliaRail - Itinerary Details PDFDocument3 pagesItaliaRail - Itinerary Details PDFChristopher MillerNo ratings yet
- Netaji Subhash College of Nursing, Palampur: MASTER ROTATION PLAN 2022-2023 (B.SC Nursing 3rd Semester)Document2 pagesNetaji Subhash College of Nursing, Palampur: MASTER ROTATION PLAN 2022-2023 (B.SC Nursing 3rd Semester)Priya100% (6)
- ABILIFY® (Aripiprazole) Savings Card ProgramDocument2 pagesABILIFY® (Aripiprazole) Savings Card ProgramGisele PhaloNo ratings yet
- SingulairDocument1 pageSingulairNava GrahazNo ratings yet
- LinzessSavingCardPDF 2Document1 pageLinzessSavingCardPDF 2tqzj54jmxnNo ratings yet
- BRILINTA CAD $5 No FTO PDFDocument1 pageBRILINTA CAD $5 No FTO PDFperaNo ratings yet
- Apriso Savings Card: Bin: Group: ID: ExpirationDocument1 pageApriso Savings Card: Bin: Group: ID: ExpirationuserillusionNo ratings yet
- Prescription Reimb Claim FormDocument2 pagesPrescription Reimb Claim FormimthedciNo ratings yet
- Relistor Savings Card: 0 CopayDocument1 pageRelistor Savings Card: 0 CopayJulieann RodgersNo ratings yet
- Pparx ApplicationsDocument8 pagesPparx ApplicationsJames MullinsNo ratings yet
- Mosquito Repellent Is Available As A Statewide Benefit: Covered ProgramsDocument5 pagesMosquito Repellent Is Available As A Statewide Benefit: Covered ProgramsJuanNo ratings yet
- Pay As Little As: Savings ProgramDocument1 pagePay As Little As: Savings ProgramelasticemperorNo ratings yet
- Savings CardDocument1 pageSavings CardAvinash MalladhiNo ratings yet
- Galderma Pharmaceutical BrochureDocument1 pageGalderma Pharmaceutical BrochureJamesNo ratings yet
- KombiglyzeXR Savings CardDocument1 pageKombiglyzeXR Savings CardRodolfo ArangoNo ratings yet
- Understanding My Benefits: Pre - Auth@Document2 pagesUnderstanding My Benefits: Pre - Auth@Jonelle Morris-DawkinsNo ratings yet
- Lantus Co-Pay Savings CardDocument1 pageLantus Co-Pay Savings CardAnthony Mckenzie0% (1)
- 3o4fxm7kk24mh6hFAQs Insurance - Daily Cash AllowanceDocument6 pages3o4fxm7kk24mh6hFAQs Insurance - Daily Cash AllowanceKajal AvchareNo ratings yet
- Zer - Pay: Every Fill. Every MonthDocument1 pageZer - Pay: Every Fill. Every MonthrebecaNo ratings yet
- Morningstar India Private Limited: Hospitalization Benefit PlanDocument10 pagesMorningstar India Private Limited: Hospitalization Benefit PlandevanyaNo ratings yet
- Health Insurance FAQ From IntrawestDocument9 pagesHealth Insurance FAQ From IntrawestScott FranzNo ratings yet
- GL3655EDocument0 pagesGL3655EandyhrNo ratings yet
- Eligibility NoticeDocument17 pagesEligibility NoticeFlintston3No ratings yet
- 2012 Comprehensive Formulary: List of Covered DrugsDocument51 pages2012 Comprehensive Formulary: List of Covered DrugsKapilNo ratings yet
- Humana 2022 Plan 2 RX3 Drug List - StandardDocument104 pagesHumana 2022 Plan 2 RX3 Drug List - StandardWalter PilimonNo ratings yet
- Medi Claim FAQsDocument9 pagesMedi Claim FAQsMOVIES BRONo ratings yet
- Brochure Online PDFDocument3 pagesBrochure Online PDFSrikanth MudivarthiNo ratings yet
- Eligibility NoticeDocument17 pagesEligibility NoticeRobert MckenzieNo ratings yet
- HeathGuard BrochureDocument2 pagesHeathGuard BrochureKumud GandhiNo ratings yet
- FAQ One Medical (Eng)Document5 pagesFAQ One Medical (Eng)Razman ZaidiNo ratings yet
- Welcome To Medicare!: Things To Think About When You Compare Medicare Drug CoverageDocument4 pagesWelcome To Medicare!: Things To Think About When You Compare Medicare Drug CoverageAlsayed General HospitalNo ratings yet
- Gmail - Your Amerigroup Application - Important Plan InformationDocument2 pagesGmail - Your Amerigroup Application - Important Plan InformationIsmael LanderosNo ratings yet
- 50a580af40315 PDFDocument1 page50a580af40315 PDFSorbito ComettoNo ratings yet
- Prescription Assistance Programs: What Resources Are Available To Help Locate An Assistance Program For My Medications?Document1 pagePrescription Assistance Programs: What Resources Are Available To Help Locate An Assistance Program For My Medications?Sorbito ComettoNo ratings yet
- Formulary - Good ReadDocument121 pagesFormulary - Good ReadJananiRajamanickamNo ratings yet
- Patient Assistance Program: How To ApplyDocument3 pagesPatient Assistance Program: How To ApplyDavid NowakowskiNo ratings yet
- 2023 - Oe - Notice - 2008 - FinalDocument5 pages2023 - Oe - Notice - 2008 - FinalabroughearNo ratings yet
- 2019 TN Formulary H0251 002 EN PDFDocument121 pages2019 TN Formulary H0251 002 EN PDFVijay YajivNo ratings yet
- 3CCO OHP Drug Formulary FinalWebDocument124 pages3CCO OHP Drug Formulary FinalWebKandraNo ratings yet
- Your Eligibility Results: Department of Health and Human Services 465 Industrial Boulevard London, Kentucky 40750-0001Document16 pagesYour Eligibility Results: Department of Health and Human Services 465 Industrial Boulevard London, Kentucky 40750-0001John SpiersNo ratings yet
- Bharati SHIP BrochureDocument2 pagesBharati SHIP Brochurehrocking1No ratings yet
- TMB UNI Family Health Care PolicyDocument24 pagesTMB UNI Family Health Care Policysubu_devasena6782100% (1)
- What Everybody Ought To Know About Health Benefit Cards: Lawsuits GuidelineDocument3 pagesWhat Everybody Ought To Know About Health Benefit Cards: Lawsuits Guidelineapi-77613236No ratings yet
- ComprKaiehensive FormularyDocument77 pagesComprKaiehensive Formularypeter_rabbitNo ratings yet
- Eligibility NoticeDocument17 pagesEligibility NoticeDJPhrostNo ratings yet
- 2011 PDP Classic FormularyDocument74 pages2011 PDP Classic FormularyEdmund NgNo ratings yet
- Coordination of Benefits: Where Can I Get More Information?Document2 pagesCoordination of Benefits: Where Can I Get More Information?api-309082881No ratings yet
- Welcome To Rio Grande Hospital and Clinics!Document2 pagesWelcome To Rio Grande Hospital and Clinics!swarnaNo ratings yet
- 2020-1769-4 Summary BrochureDocument9 pages2020-1769-4 Summary Brochurekalli Nagarjun ReddyNo ratings yet
- Health Companion 12 - 2011an-02Document2 pagesHealth Companion 12 - 2011an-02sprashant5No ratings yet
- HIS Claim Guide Lines - 0.3Document3 pagesHIS Claim Guide Lines - 0.3Chirag Kumar VegadNo ratings yet
- Company Your Policy ExplainedDocument34 pagesCompany Your Policy ExplaineddeonptNo ratings yet
- FS PrivateInsuranceDocument2 pagesFS PrivateInsuranceIndiana Family to FamilyNo ratings yet
- Bupa Advantage Care Membership GuideDocument40 pagesBupa Advantage Care Membership GuidePatricia GuzmanNo ratings yet
- International Exclusive Policy WordingDocument44 pagesInternational Exclusive Policy WordingKetan VashishthaNo ratings yet
- TRAVEL CF - Out of ProvinceDocument4 pagesTRAVEL CF - Out of ProvinceSaid Safa TurabiNo ratings yet
- Mymedicare Registration FormDocument2 pagesMymedicare Registration Formbonnakoy72No ratings yet
- Sisc Q ADocument7 pagesSisc Q Aapi-204910805No ratings yet
- ORV SSV MY23 SPEC Can Am MAVX3 RS TURBO RR EN HRDocument1 pageORV SSV MY23 SPEC Can Am MAVX3 RS TURBO RR EN HRmongojerryNo ratings yet
- Teco ManualDocument1 pageTeco ManualmongojerryNo ratings yet
- EDP - DSP-90 - Air - NEXTDocument2 pagesEDP - DSP-90 - Air - NEXTmongojerryNo ratings yet
- Cog WorksheetDocument1 pageCog WorksheetmongojerryNo ratings yet
- Wsu Mthatha Faculty of Health Sciences Prospectus 2021 FullDocument144 pagesWsu Mthatha Faculty of Health Sciences Prospectus 2021 FullThandoNo ratings yet
- Teachers NHS Patient Journey PowerPoint Presentation 08032016Document40 pagesTeachers NHS Patient Journey PowerPoint Presentation 08032016Dave KokNo ratings yet
- CHN211 Week2 PPT The Healthcare Delivery System (Voice Recorded)Document55 pagesCHN211 Week2 PPT The Healthcare Delivery System (Voice Recorded)Krystel Anne MilanNo ratings yet
- Unit 5 Factors Affecting The Healthcare SystemDocument29 pagesUnit 5 Factors Affecting The Healthcare SystemYuri ChanNo ratings yet
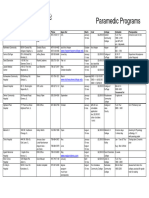
- Paramedic ProgramsDocument2 pagesParamedic Programsimurph3No ratings yet
- Journal Homepage: - : IntroductionDocument6 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Digitel Outbound Transfer Script UpdatedDocument2 pagesDigitel Outbound Transfer Script UpdatedFRAULIEN GLINKA FANUGAONo ratings yet
- Pendampingan Praktik Mandiri Bidan (PMB) Bidan Delima Dalam Melaksanakan Pendokumentasian Pelayanan Asuhan KebidananDocument9 pagesPendampingan Praktik Mandiri Bidan (PMB) Bidan Delima Dalam Melaksanakan Pendokumentasian Pelayanan Asuhan KebidananWahyu HidayatNo ratings yet
- Leave Report Ni MamaDocument20 pagesLeave Report Ni MamaMichael Angelo SarabiaNo ratings yet
- Test Bank For Medical-Surgical Nursing: Concepts & Practice, 2Nd Edition, Susan C. Dewit, Isbn-10: 1437717071, Isbn-13: 9781437717075Document36 pagesTest Bank For Medical-Surgical Nursing: Concepts & Practice, 2Nd Edition, Susan C. Dewit, Isbn-10: 1437717071, Isbn-13: 9781437717075saucisseserratedv8s97100% (22)
- IELTS Listening Practice Test 5: Section 1Document9 pagesIELTS Listening Practice Test 5: Section 1HoaiNhiNguyenNo ratings yet
- PRC FORMS New Format 3Document5 pagesPRC FORMS New Format 3mark OrpillaNo ratings yet
- International Air Waybill: From: Shipper'S AddressDocument1 pageInternational Air Waybill: From: Shipper'S AddressAIRF ZAMANNo ratings yet
- SB RESOLUTION NO. 24 s2020Document2 pagesSB RESOLUTION NO. 24 s2020Rave PerezNo ratings yet
- Initial and Comprehensive Patient Assessments: ScopeDocument3 pagesInitial and Comprehensive Patient Assessments: ScopeAngelica Mae BautistaNo ratings yet
- Nursing InfoooooooooooooooDocument6 pagesNursing InfoooooooooooooooIsabelNo ratings yet
- Settled Invoice IB150523J002605Document2 pagesSettled Invoice IB150523J002605thapliyalneeraj1985No ratings yet
- A Medical Outreach Elective CourseDocument11 pagesA Medical Outreach Elective CourseRobert SmithNo ratings yet
- Major Stakeholders of Health Care: Presented By-Maj Kavita Kumari 1St Yr MSC (N)Document29 pagesMajor Stakeholders of Health Care: Presented By-Maj Kavita Kumari 1St Yr MSC (N)Kavita kumari100% (1)
- 2814 PDFDocument388 pages2814 PDFgvvsrk1980 chowdaryNo ratings yet
- Service Rutin Genset September 2020Document10 pagesService Rutin Genset September 2020Wahyu Alfa OmegaNo ratings yet
- Colleges of Education - Ghana Academic Calendar For 2022/2023Document2 pagesColleges of Education - Ghana Academic Calendar For 2022/2023Adwoa LeeNo ratings yet
- Cbki4103 Knowledge ManagementDocument14 pagesCbki4103 Knowledge Managementlya natasyaNo ratings yet
- A2 Contemporary Healthdocx 290747Document3 pagesA2 Contemporary Healthdocx 290747Soumyadeep BoseNo ratings yet
- Arero Primary Hospital Consultation ProtocolDocument16 pagesArero Primary Hospital Consultation Protocolsami ketema100% (4)
- 04 2017 TT-BYT enDocument45 pages04 2017 TT-BYT endanhhomylinh99No ratings yet
- Bhopal All Liist DRDocument20 pagesBhopal All Liist DRvishalrai.ddNo ratings yet
- NCM 109 SL Module 2Document2 pagesNCM 109 SL Module 2Christine DonatoNo ratings yet