You might also like
- ECG Rhythm InterpretationDocument16 pagesECG Rhythm InterpretationJanettNo ratings yet
- Modul EKGDocument101 pagesModul EKGAjeng Dwik01No ratings yet
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- Short Answer Question SurgeryDocument9 pagesShort Answer Question SurgeryJohn M. Hemsworth100% (2)
- 12 Weeks To Your Hottest Body EverDocument49 pages12 Weeks To Your Hottest Body EverSixp8ck100% (1)
- Electrocardiography: Dr. Anand PatelDocument155 pagesElectrocardiography: Dr. Anand PatelDeepika PatelNo ratings yet
- ECG Interpretation: DR S J Bhosale DM, FPCC (Canada) Associate Professor Tata Memorial CentreDocument90 pagesECG Interpretation: DR S J Bhosale DM, FPCC (Canada) Associate Professor Tata Memorial Centrevaishali TayadeNo ratings yet
- DR Kupe - ECGDocument14 pagesDR Kupe - ECGIrfan ZiadNo ratings yet
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationFrom EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationRating: 3 out of 5 stars3/5 (1)
- EcgDocument57 pagesEcgenii_ta100% (9)
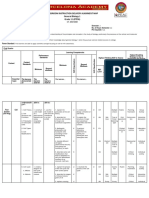
- Classroom Instruction Delivery Alignment Map General Biology 1 Grade 11 (STEM)Document6 pagesClassroom Instruction Delivery Alignment Map General Biology 1 Grade 11 (STEM)JunedelMirallesPerez50% (2)
- ECG InterpretationDocument48 pagesECG InterpretationKervayse St.ClairNo ratings yet
- 11-Vital Signs Unit 12 To 17Document74 pages11-Vital Signs Unit 12 To 17Rashid HussainNo ratings yet
- Ecg in DogsDocument107 pagesEcg in DogsPLABITA GOSWAMI100% (2)
- 006 Pathology MCQ ACEM Primary CellularDocument5 pages006 Pathology MCQ ACEM Primary CellularIrum RafeeqNo ratings yet
- ElectrocardiogramDocument52 pagesElectrocardiogramTuong HoangManhNo ratings yet
- ECG Lesson 1Document5 pagesECG Lesson 1Marwan M.No ratings yet
- Elektrokardiogramm) Is A Graphic Produced by An ElectrocardiographDocument5 pagesElektrokardiogramm) Is A Graphic Produced by An ElectrocardiographReverie ManalaysayNo ratings yet
- EKGDocument153 pagesEKGOsmy JuniorNo ratings yet
- Electrocardiography: An Introduction To The ECGDocument76 pagesElectrocardiography: An Introduction To The ECGInnocent Clifford MaranduNo ratings yet
- CVS Physiology (Assignment) : Abu BakarDocument6 pagesCVS Physiology (Assignment) : Abu BakarAbu BakarNo ratings yet
- ECG Made EasyDocument82 pagesECG Made EasyBobby SodhiNo ratings yet
- ECG 11 HikDocument21 pagesECG 11 Hikmdee02031999mNo ratings yet
- Lab ManualDocument33 pagesLab Manualg8248418302No ratings yet
- I. The Standard 12 Lead ECGDocument2 pagesI. The Standard 12 Lead ECGapi-376925250% (2)
- Presentation 1Document33 pagesPresentation 1Даша КонстантиноваNo ratings yet
- ElectrocardiographDocument5 pagesElectrocardiographGeorge MagedNo ratings yet
- Ecg Physio LectureDocument60 pagesEcg Physio LectureAninze Chidera100% (1)
- Bipolar Limb Leads (Frontal Plane)Document7 pagesBipolar Limb Leads (Frontal Plane)jonna casumpangNo ratings yet
- 9 EcgDocument12 pages9 EcgTommy CharwinNo ratings yet
- ECG With ImageDocument7 pagesECG With ImagemathavanNo ratings yet
- Basic ECGDocument152 pagesBasic ECGTuấn Thanh VõNo ratings yet
- Project 2 Electrocardiography: Practical TasksDocument16 pagesProject 2 Electrocardiography: Practical TasksFahad ShahidNo ratings yet
- Ecg Engl Large 126Document125 pagesEcg Engl Large 126Andreea-Sânziana StanciuNo ratings yet
- L10 PDFDocument13 pagesL10 PDFMiles HuiNo ratings yet
- Ecg FileDocument29 pagesEcg Fileneha miriNo ratings yet
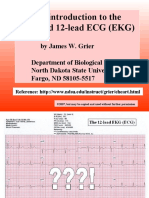
- A Brief Introduction To The Standard 12-Lead ECG (EKG)Document29 pagesA Brief Introduction To The Standard 12-Lead ECG (EKG)Lazar BoskovicNo ratings yet
- ECG Dr. JabeenDocument164 pagesECG Dr. JabeenMohsan RafiqNo ratings yet
- Lecture 3c Interpretation of ECG - The Heart Model EM Theory & Applications II Spring Semester 2006Document27 pagesLecture 3c Interpretation of ECG - The Heart Model EM Theory & Applications II Spring Semester 2006hebaNo ratings yet
- ECG Waves and Intervals:: Simultaneously)Document2 pagesECG Waves and Intervals:: Simultaneously)blade157721No ratings yet
- Electrical Conduction Pathway: Course Lesson Student Email Atika - Salsabila91@ui - Ac.idDocument12 pagesElectrical Conduction Pathway: Course Lesson Student Email Atika - Salsabila91@ui - Ac.idlemon kyuteaNo ratings yet
- Electrocardiogram (Ecg) : Base Line or Isopotential LineDocument15 pagesElectrocardiogram (Ecg) : Base Line or Isopotential Linegyspsunshine girlNo ratings yet
- Cardiac Cycle: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraDocument27 pagesCardiac Cycle: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraFira TasyaNo ratings yet
- Electrocardiogram Asyik GuysDocument29 pagesElectrocardiogram Asyik Guysdesinta mrNo ratings yet
- Cardiovascular Lecture 2 - 2023 2024Document11 pagesCardiovascular Lecture 2 - 2023 2024inegbenosegideonNo ratings yet
- Peer 2 Im1Document9 pagesPeer 2 Im1fabrahamNo ratings yet
- Ekg Normal PapdiDocument51 pagesEkg Normal PapdifennyaliskaNo ratings yet
- How Procedure Is Performed: ElectrocardiogramDocument10 pagesHow Procedure Is Performed: ElectrocardiogramJonathan AlvarezNo ratings yet
- 2020 EcgDocument49 pages2020 EcgHannah HalimNo ratings yet
- NMTEC 211-ECG Lab InstructionsDocument4 pagesNMTEC 211-ECG Lab InstructionsRisleNo ratings yet
- Ecg LP 1Document97 pagesEcg LP 1Cosmina GheorgheNo ratings yet
- Cardiologia - EletrocardiografiaDocument40 pagesCardiologia - EletrocardiografiaDANIEL ALEJANDRONo ratings yet
- ECG EKG InterpretationDocument11 pagesECG EKG InterpretationGunma AkagiNo ratings yet
- 05 - ElektrokardiogramDocument39 pages05 - ElektrokardiogramNauval Zilal FananyNo ratings yet
- Ecg (Ekg) : Dr. Jamal Dabbas Interventional Cardiologist & InternistDocument87 pagesEcg (Ekg) : Dr. Jamal Dabbas Interventional Cardiologist & Internistsara rababahNo ratings yet
- Electrical Activity of The HeartDocument40 pagesElectrical Activity of The HeartMichael Ajak GhaiNo ratings yet
- CCApostol ECGDocument115 pagesCCApostol ECGAlanis ApostolNo ratings yet
- Electrocardiogram (Ecg) Introduction of Basic Principles: Dian Puspita SariDocument47 pagesElectrocardiogram (Ecg) Introduction of Basic Principles: Dian Puspita SariArie Krisnayanti Ida AyuNo ratings yet
- ECG PracticalDocument48 pagesECG PracticalbvkjtzrvnyNo ratings yet
- ECG EKG: BasicsDocument191 pagesECG EKG: BasicsSabio DenmenNo ratings yet
- (K29) Electrocardiogram CVSDocument43 pages(K29) Electrocardiogram CVSXeniel AlastairNo ratings yet
- K-22 Fisio Intrinsic Conducting System - CVS-K22Document43 pagesK-22 Fisio Intrinsic Conducting System - CVS-K22Jane Andrea Christiano DjianzonieNo ratings yet
- Case StudyDocument2 pagesCase StudySanjay RanaNo ratings yet
- Emergenc Eof Services EconomyDocument29 pagesEmergenc Eof Services EconomySanjay RanaNo ratings yet
- 5B. ESE-Question Paper PatternDocument1 page5B. ESE-Question Paper PatternSanjay RanaNo ratings yet
- Cervical FractureDocument84 pagesCervical FractureSanjay RanaNo ratings yet
- FormsDocument9 pagesFormsSanjay RanaNo ratings yet
- The SpineDocument113 pagesThe SpineSanjay RanaNo ratings yet
- District PCPNDT FormatsDocument6 pagesDistrict PCPNDT FormatsSanjay RanaNo ratings yet
- POI Lab ReviewerDocument2 pagesPOI Lab ReviewerJerick JusayNo ratings yet
- Harm Reduction: A British Columbia Community GuideDocument30 pagesHarm Reduction: A British Columbia Community GuideStephen OlsonNo ratings yet
- Thesis Statement Examples Cervical CancerDocument5 pagesThesis Statement Examples Cervical Cancerbrittanyjonescolumbia100% (1)
- Tamoxifen CitrateDocument3 pagesTamoxifen Citrateapi-3797941No ratings yet
- Cordyceps 16mayvjDocument2 pagesCordyceps 16mayvjwarpansy15No ratings yet
- Nephrotic Syndrome (Nephrosis)Document9 pagesNephrotic Syndrome (Nephrosis)Madhusmita SatapathyNo ratings yet
- Unit 7 Teachers BookDocument14 pagesUnit 7 Teachers BookOx ScarNo ratings yet
- Thyroid Disorders in PregnancyDocument46 pagesThyroid Disorders in PregnancyMara Medina - BorleoNo ratings yet
- Nursing Assessment 1Document70 pagesNursing Assessment 1Amira AttyaNo ratings yet
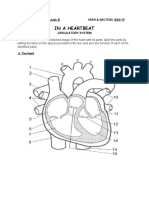
- Circulatory System ActivityDocument5 pagesCirculatory System ActivityKeen Jude CaminosNo ratings yet
- PROSIDING 1 - Ami (ICES 2017) - The Impact of Parents Education Level On Career) - 2018!11!19T07!28!13.721ZDocument296 pagesPROSIDING 1 - Ami (ICES 2017) - The Impact of Parents Education Level On Career) - 2018!11!19T07!28!13.721ZCindi UtariNo ratings yet
- Case Presentation On Ischemic Cardiomyopathy & Ccf-1-1Document18 pagesCase Presentation On Ischemic Cardiomyopathy & Ccf-1-1Maliha aliNo ratings yet
- IGNOU Block 4 Unit 1 Epidemiology of Non-Communicable DiseasesDocument12 pagesIGNOU Block 4 Unit 1 Epidemiology of Non-Communicable Diseaseserice.researchNo ratings yet
- ActinomycetesDocument15 pagesActinomycetesBenson100% (3)
- Modulo Di Rimborso Spese Mediche ClaimForm-EnglishDocument2 pagesModulo Di Rimborso Spese Mediche ClaimForm-EnglishCarlo_Sturlese_4203No ratings yet
- @ebookmedicin 2017 Textbook of Radiology Abdomen and PelvisDocument23 pages@ebookmedicin 2017 Textbook of Radiology Abdomen and PelviskinexNo ratings yet
- Sexual Assault Opinion PieceDocument2 pagesSexual Assault Opinion Pieceapi-253813581No ratings yet
- 05 N026 31333Document13 pages05 N026 31333Ankur AggarwalNo ratings yet
- Clinphar M2-M3 Answer Case StudyDocument1 pageClinphar M2-M3 Answer Case StudyGwen Myles JoverNo ratings yet
- Smoking As A Risk Factor For Dry Socket ComplicationDocument15 pagesSmoking As A Risk Factor For Dry Socket ComplicationI Gusti Ayu WulanNo ratings yet
- Typology of Nursing2Document40 pagesTypology of Nursing2Patrisha JumahariNo ratings yet
- Weekly Plan3 - TNDocument37 pagesWeekly Plan3 - TNABDULGAFFAR MNo ratings yet
- Learning Format in Ateneo de Zamboanga University.: Definition of TermsDocument2 pagesLearning Format in Ateneo de Zamboanga University.: Definition of TermsFATIMA SHANNON INDASAN. PAKANNANo ratings yet
- Answer Sheet - Module 6Document6 pagesAnswer Sheet - Module 6sjhdjshakjNo ratings yet
- Septic Shock: Ask The ExpertDocument4 pagesSeptic Shock: Ask The ExpertIvy Dianne PascualNo ratings yet