0% found this document useful (0 votes)
2K views1 pageAuto Insurance Declarations Page Sample
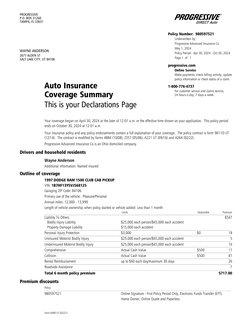
This document is an auto insurance declaration page for Wayne Anderson outlining the coverage, limits, deductibles and premiums for his 1997 Dodge Ram pickup truck. It provides liability, uninsured motorist, underinsured motorist, comprehensive, collision and additional coverages for a 6 month policy period from April 30, 2024 to October 30, 2024.
Uploaded by
deronmarcum0Copyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
2K views1 pageAuto Insurance Declarations Page Sample
This document is an auto insurance declaration page for Wayne Anderson outlining the coverage, limits, deductibles and premiums for his 1997 Dodge Ram pickup truck. It provides liability, uninsured motorist, underinsured motorist, comprehensive, collision and additional coverages for a 6 month policy period from April 30, 2024 to October 30, 2024.
Uploaded by
deronmarcum0Copyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as PDF, TXT or read online on Scribd
- Auto Insurance Coverage Summary: This section outlines the summary of auto insurance coverage, including effective dates, insured vehicle, contact information, and specific coverage details such as liability limits and premium costs.