You might also like
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Day 2 - Ulcerative Colitis PDFDocument14 pagesDay 2 - Ulcerative Colitis PDFMaria Charis Anne IndananNo ratings yet
- Pancreatic AdenocarcinomaDocument6 pagesPancreatic AdenocarcinomafikriafisNo ratings yet
- Cefadroxil: Antibiotic ClassDocument2 pagesCefadroxil: Antibiotic ClassTariNo ratings yet
- HIV and Its TreatmentDocument24 pagesHIV and Its Treatmentaathira_kNo ratings yet
- Lung CancerDocument2 pagesLung CancerAurea Jasmine DacuycuyNo ratings yet
- DM Case StudyDocument21 pagesDM Case StudyBern TolentinoNo ratings yet
- Pathophysiology: Rectal CarcinomaDocument25 pagesPathophysiology: Rectal CarcinomaCristina CristinaNo ratings yet
- Acute Myeloid Leukemia (Drug Study)Document3 pagesAcute Myeloid Leukemia (Drug Study)Krisianne Mae Lorenzo FranciscoNo ratings yet
- Managing Nause and Vomiting-Crit-Care-Nurse-2003-Garrett-31-50 PDFDocument22 pagesManaging Nause and Vomiting-Crit-Care-Nurse-2003-Garrett-31-50 PDFpmuftiaNo ratings yet
- Gastric CancerDocument7 pagesGastric CancerMicah PingawanNo ratings yet
- CAD - EBM September 2020 EditionDocument17 pagesCAD - EBM September 2020 EditionNaga Venkatamanoj Kumar PakalapatiNo ratings yet
- DPatho ProstateDocument2 pagesDPatho Prostateshujin_samaNo ratings yet
- Understanding Addison's Disease: Causes, Symptoms and TreatmentDocument10 pagesUnderstanding Addison's Disease: Causes, Symptoms and TreatmentAnn KelseaNo ratings yet
- Nursing Process OsteosarcomaDocument34 pagesNursing Process OsteosarcomaDonJohnNo ratings yet
- Addison's Disease: An Overview of Etiology, Pathogenesis and Clinical PresentationDocument11 pagesAddison's Disease: An Overview of Etiology, Pathogenesis and Clinical PresentationKertiasihwayanNo ratings yet
- ConceptMap AMLDocument1 pageConceptMap AMLnursing concept mapsNo ratings yet
- UTI (Urinary Tract Infection)Document9 pagesUTI (Urinary Tract Infection)Carson BirthNo ratings yet
- Epidemiology, Pathogenesis, and Pathology of NeuroblastomaDocument21 pagesEpidemiology, Pathogenesis, and Pathology of NeuroblastomaHandre PutraNo ratings yet
- Gastric CarcinomaDocument21 pagesGastric CarcinomaAli Abbas100% (2)
- PathophysiologyDocument5 pagesPathophysiologyJessyl GirayNo ratings yet
- CholelitiasisDocument42 pagesCholelitiasisEdwin YosuaNo ratings yet
- Philippine Urological Association, Inc.: Executive Committee and Board Members 1997Document12 pagesPhilippine Urological Association, Inc.: Executive Committee and Board Members 1997mits98No ratings yet
- Pamantasan NG Cabuyao College of Health Allied Sciences College of NursingDocument43 pagesPamantasan NG Cabuyao College of Health Allied Sciences College of NursingSofea MustaffaNo ratings yet
- Prostate Cancer: Symptoms, Diagnosis, Treatment, and RehabilitationDocument4 pagesProstate Cancer: Symptoms, Diagnosis, Treatment, and RehabilitationParixit DasNo ratings yet
- HPV Virus Causes Recurrent Respiratory Papillomatosis in BoyDocument21 pagesHPV Virus Causes Recurrent Respiratory Papillomatosis in BoyDaffa IbnurasyNo ratings yet
- Lab 5 Diabetes InsipidusDocument6 pagesLab 5 Diabetes InsipidusLisa EkapratiwiNo ratings yet
- Case 052: Biliary ColicDocument4 pagesCase 052: Biliary ColicZauzaNo ratings yet
- Colorectal CancerDocument29 pagesColorectal CancerLeeyanBhadzzVagayNo ratings yet
- Case Scenario Osteoarthritis Week 16 GerontologDocument5 pagesCase Scenario Osteoarthritis Week 16 GerontologMary Josette NavarraNo ratings yet
- Pathophysiology of Prostate Cancer Risk FactorsDocument3 pagesPathophysiology of Prostate Cancer Risk Factorsmkho100% (1)
- Pharmacologic management of bleomycinDocument1 pagePharmacologic management of bleomycinKim ApuradoNo ratings yet
- Chapter 24.child With CancerDocument42 pagesChapter 24.child With Cancerjayme4schrankNo ratings yet
- Case Study 4th Year 1st Sem 2 Final FixDocument30 pagesCase Study 4th Year 1st Sem 2 Final FixHerschel QuerimitNo ratings yet
- Pathophysiology of Acute CholecystitisDocument2 pagesPathophysiology of Acute CholecystitisKush KhannaNo ratings yet
- Pat 2 Medsurg1Document20 pagesPat 2 Medsurg1api-300849832No ratings yet
- Bacterial Pneumonia PharmacologyDocument70 pagesBacterial Pneumonia PharmacologyMarc Imhotep Cray, M.D.No ratings yet
- Renal Concept MapDocument8 pagesRenal Concept MapXtine CajiNo ratings yet
- Case Study 1: Nicole: 1. Discuss The Significance of Nicole's Laboratory FindingsDocument12 pagesCase Study 1: Nicole: 1. Discuss The Significance of Nicole's Laboratory FindingsClint NavarroNo ratings yet
- Cancer NursingDocument53 pagesCancer Nursingfairwoods100% (1)
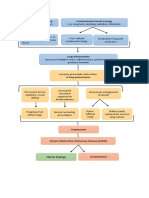
- COPD: Pathogenesis Environmental Insult To Lungs Genetic SusceptibilityDocument1 pageCOPD: Pathogenesis Environmental Insult To Lungs Genetic SusceptibilityMaria Vhanesa AbuyanNo ratings yet
- Pa Tho Physiology of Cad NstemiDocument2 pagesPa Tho Physiology of Cad Nstemianreilegarde100% (1)
- Pathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsDocument2 pagesPathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsAb Staholic Boii100% (1)
- V. Pathophysiology Modifiable: Non - ModifiableDocument2 pagesV. Pathophysiology Modifiable: Non - ModifiableMary Grace BanezNo ratings yet
- Cushing's SyndromeDocument5 pagesCushing's SyndromesummerduskNo ratings yet
- Case Study For LeukemiaDocument5 pagesCase Study For LeukemiaGabbii CincoNo ratings yet
- Para Neoplastic SyndromeDocument5 pagesPara Neoplastic SyndromeSamir Sarkar100% (1)
- Addison'sDocument4 pagesAddison'sKoRnflakesNo ratings yet
- A. A Sudden Change in How Brain Cells Send Electrical Signals To One AnotherDocument70 pagesA. A Sudden Change in How Brain Cells Send Electrical Signals To One AnotherMwansaay Twain HolyNo ratings yet
- Medications and Nursing Responsibilities for Bone HealthDocument6 pagesMedications and Nursing Responsibilities for Bone HealthDarla JoyceNo ratings yet
- Thyroid Papillary Carcinoma CaseDocument6 pagesThyroid Papillary Carcinoma CaseRandy F BabaoNo ratings yet
- CVD Bleed Case StudyDocument25 pagesCVD Bleed Case StudyMargaret Jenaw JenawNo ratings yet
- Hepatocellula R CarcinomaDocument45 pagesHepatocellula R Carcinomamhean azneitaNo ratings yet
- CellulitisDocument5 pagesCellulitisaimigdragonNo ratings yet
- Polycythemia in NewbornDocument25 pagesPolycythemia in NewbornTheva Thy100% (2)
- Cervical Cancer Screening and TreatmentDocument104 pagesCervical Cancer Screening and TreatmentArie PratamaNo ratings yet
- A Case Report of Classical Hodgkin's Lymphoma Presented With Anemia of Chronic Disease As Microcytic Hypochromic TypeDocument3 pagesA Case Report of Classical Hodgkin's Lymphoma Presented With Anemia of Chronic Disease As Microcytic Hypochromic TypeIOSRjournalNo ratings yet
- Perforated Peptic Ulcer Symptoms and DiagnosisDocument68 pagesPerforated Peptic Ulcer Symptoms and DiagnosisSaibo BoldsaikhanNo ratings yet
- A Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutFrom EverandA Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutRating: 5 out of 5 stars5/5 (1)
- Dimorphic Systemic MycosesDocument65 pagesDimorphic Systemic Mycoseskedar karkiNo ratings yet
- CHN 2 SET A (Key Answers)Document7 pagesCHN 2 SET A (Key Answers)Marie Ordonia de Pona100% (1)
- First AidDocument26 pagesFirst Aidmih abdouNo ratings yet
- Neuro-Ophthalmology: Introduction: James Goodwin, MD (Attending)Document4 pagesNeuro-Ophthalmology: Introduction: James Goodwin, MD (Attending)Mariano FioreNo ratings yet
- Zydus HospitalDocument28 pagesZydus HospitalSunil TakNo ratings yet
- Course Exercise - ACLS Precourse Self-Assessment and Precourse WorkDocument3 pagesCourse Exercise - ACLS Precourse Self-Assessment and Precourse WorksameerocksNo ratings yet
- Morse Fall Scale AssessmentDocument5 pagesMorse Fall Scale AssessmentQueen ShNo ratings yet
- FHP Health Care ProductsDocument62 pagesFHP Health Care ProductsKamlesh Kumar Mandal100% (3)
- Activity Notification and Consent Form (Under 18yrs) : Sensitive: Personnel (When Participant's Details Are Entered)Document2 pagesActivity Notification and Consent Form (Under 18yrs) : Sensitive: Personnel (When Participant's Details Are Entered)Alvin JacobNo ratings yet
- Nebulization TherapyDocument2 pagesNebulization TherapySamantha Nicole MendozaNo ratings yet
- MS2 - Neurologic Disorder My ReportDocument30 pagesMS2 - Neurologic Disorder My ReportNeil Lansang BallobanNo ratings yet
- Blepharoplasty: ExtendedDocument4 pagesBlepharoplasty: ExtendedBFF BotoxNo ratings yet
- Antiplatelet DrugsDocument31 pagesAntiplatelet DrugsSyed Usama Rashid100% (2)
- Closure of Oroantral Communications A Review of The LiteratureDocument8 pagesClosure of Oroantral Communications A Review of The LiteratureFaisal H RanaNo ratings yet
- Office of The Provincial Governor: Province of Oriental MindoroDocument1 pageOffice of The Provincial Governor: Province of Oriental MindoroZyreen Kate BCNo ratings yet
- Suspected Adverse Reactions To COVID 19 Vaccination and Safety of SoHODocument11 pagesSuspected Adverse Reactions To COVID 19 Vaccination and Safety of SoHOVevveNo ratings yet
- 310-Article Text-582-1-10-20210312-1Document13 pages310-Article Text-582-1-10-20210312-1Ni Putu SwastyNo ratings yet
- Communith Health SurveyDocument3 pagesCommunith Health SurveyDivina Gracia Vibal CieloNo ratings yet
- Critical Nursing IntroductionDocument4 pagesCritical Nursing IntroductionJo Traven AzueloNo ratings yet
- Parasitology Lab Study ChartDocument2 pagesParasitology Lab Study ChartnoneyabuNo ratings yet
- International Ayurvedic Medical Journal explores Madhuyashti and yogaDocument7 pagesInternational Ayurvedic Medical Journal explores Madhuyashti and yogaVatsas JoshiNo ratings yet
- All Obgyn Osce (2) Good Book For OsceDocument75 pagesAll Obgyn Osce (2) Good Book For OsceMohamed Hassan91% (47)
- P7b11toc Gastroenterology and NutritionDocument19 pagesP7b11toc Gastroenterology and NutritionWidya Lestari CapawatyNo ratings yet
- Ashley Fagert ResumeDocument1 pageAshley Fagert Resumeapi-455767165No ratings yet
- x9585374 Rev1117b Pro Mag Ultra Automatic Biopsy InstrumentDocument9 pagesx9585374 Rev1117b Pro Mag Ultra Automatic Biopsy InstrumentJonathan David Castillo SanchezNo ratings yet
- Emergency Assistance Plan by TW 12oct21Document7 pagesEmergency Assistance Plan by TW 12oct21Than WinNo ratings yet
- Role of Autologous Platelet-Rich Plasma in Z-PlastyDocument3 pagesRole of Autologous Platelet-Rich Plasma in Z-PlastyasclepiuspdfsNo ratings yet
- PKMDocument3 pagesPKMSarah ArumNo ratings yet
- Diagnostic Test DesignDocument30 pagesDiagnostic Test DesignDika Gita PratamaNo ratings yet
- Intern Survival Guide: Department of Internal MedicineDocument35 pagesIntern Survival Guide: Department of Internal MedicineSuvetha TamilarasanNo ratings yet