You might also like
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Blood TransfusionDocument104 pagesBlood TransfusionrodelagapitoNo ratings yet
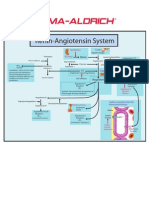
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Blood Transfusion: DR Vishwabharathi TDocument28 pagesBlood Transfusion: DR Vishwabharathi TSuma0% (1)
- Blood Transfusion - Indications, Administration and Adverse Reactions PDFDocument9 pagesBlood Transfusion - Indications, Administration and Adverse Reactions PDFStacey WoodsNo ratings yet
- RBC AliquotsDocument1 pageRBC AliquotsARIF AHAMMEDNo ratings yet
- Blood Tranfusion11Document60 pagesBlood Tranfusion11Marites Angeles Bautista100% (2)
- Theory UrinalysisDocument23 pagesTheory UrinalysisAnggi Dyah AristiNo ratings yet
- CASE REPORT - Syphilis in PregnancyDocument28 pagesCASE REPORT - Syphilis in PregnancymuhammadrubaiNo ratings yet
- Blood TransfusionDocument28 pagesBlood TransfusionChristina DienteNo ratings yet
- RH IcompatibilityDocument3 pagesRH IcompatibilitySourabh SharafNo ratings yet
- Practice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearDocument44 pagesPractice Teaching On Anemia: Presented By: Mr. Hari Singh Nagar M. SC Nursing 1 YearSundarNo ratings yet
- II. General and Specific ObjectivesDocument5 pagesII. General and Specific ObjectivesRae Marie AquinoNo ratings yet
- Aplastic AnemiaDocument11 pagesAplastic AnemiaToni Shiraishi-Aque RuizNo ratings yet
- Genitourinary Assessment: Jan Bazner-Chandler RN, MSN, CNS, CPNPDocument27 pagesGenitourinary Assessment: Jan Bazner-Chandler RN, MSN, CNS, CPNPJason Nisky100% (1)
- Chronic Kidney DiseaseDocument7 pagesChronic Kidney DiseaseLardel Balbiran LafortezaNo ratings yet
- Chapter 1 Fundamental Concepts SPSS - Descriptive StatisticsDocument4 pagesChapter 1 Fundamental Concepts SPSS - Descriptive StatisticsAvinash AmbatiNo ratings yet
- Transfusion of Blood & Blood Components1Document45 pagesTransfusion of Blood & Blood Components1Chamika Huruggamuwa100% (1)
- Graves DseDocument5 pagesGraves DseHester Marie SimpiaNo ratings yet
- G3 IAH and ACSDocument29 pagesG3 IAH and ACSRoshin Mae E. TejeroNo ratings yet
- Obstetric Case Study CesarianDocument16 pagesObstetric Case Study CesarianRazan NasereddineNo ratings yet
- Introduction of Pediatric Nursing: Om Nursing Academy Anil Kantiwal Gudha (Whatsapp 9694936335)Document4 pagesIntroduction of Pediatric Nursing: Om Nursing Academy Anil Kantiwal Gudha (Whatsapp 9694936335)Preeti ChouhanNo ratings yet
- PhototherapyDocument8 pagesPhototherapyNylia AtibiNo ratings yet
- Hiv Case StudyDocument2 pagesHiv Case Studyapi-485814878No ratings yet
- Von Willebrand DiseaseDocument9 pagesVon Willebrand DiseaserandyNo ratings yet
- Pediatric Nursing Care Plan Impaired Physical MobilityDocument5 pagesPediatric Nursing Care Plan Impaired Physical Mobilityapi-3077327050% (1)
- Hemolytic Disease of The Newborn: (Erythroblastosis Fetalis)Document17 pagesHemolytic Disease of The Newborn: (Erythroblastosis Fetalis)sandeepv08No ratings yet
- Benign Prostate Hyperplasia (BPH)Document81 pagesBenign Prostate Hyperplasia (BPH)Salaxar Senpai100% (1)
- Insulin AdministrationDocument15 pagesInsulin Administrationmec17No ratings yet
- Central Venous PressureDocument10 pagesCentral Venous PressureAngelo ArquizaNo ratings yet
- Nursing Care Plan General Objective: To Promote Safety Through Prevention of The Spread of InfectionDocument3 pagesNursing Care Plan General Objective: To Promote Safety Through Prevention of The Spread of InfectionitsmeayaNo ratings yet
- Case Study JatDocument45 pagesCase Study JatHSEINNo ratings yet
- CNN Practice QuestionsDocument5 pagesCNN Practice QuestionsUri Perez MontedeRamosNo ratings yet
- Anemia IntroductionDocument15 pagesAnemia IntroductionNitesh Kotian100% (1)
- Glasgow Coma Scale: - Eye-Opening - Motor - Verbal ResponsesDocument13 pagesGlasgow Coma Scale: - Eye-Opening - Motor - Verbal ResponsesSofianNo ratings yet
- Lydia Hall: Reporters: Gwenn Marielle Galdo Kristine CustodioDocument15 pagesLydia Hall: Reporters: Gwenn Marielle Galdo Kristine CustodioKristine CustodioNo ratings yet
- Theoretical Framework of Nursing PracticeDocument18 pagesTheoretical Framework of Nursing PracticeIsrael AgrisNo ratings yet
- NCP Poststreptococcal GlomerulonephritisDocument12 pagesNCP Poststreptococcal GlomerulonephritisScarlet ScarletNo ratings yet
- Critical Care - Criteria For Admission & Role of NurseDocument64 pagesCritical Care - Criteria For Admission & Role of NurseProf. Ramsharan MehtaNo ratings yet
- Blood Transfusion Reaction 3032018Document33 pagesBlood Transfusion Reaction 3032018Kelly YeowNo ratings yet
- Portal HypertensionDocument65 pagesPortal HypertensionVenu MadhavNo ratings yet
- CBC InterpretationDocument6 pagesCBC InterpretationKate Basa100% (1)
- About Creamy LayerDocument17 pagesAbout Creamy LayerbaluskbNo ratings yet
- Assessment and Management of Patients With Hematologic DisordersDocument124 pagesAssessment and Management of Patients With Hematologic DisordersAngelicaMarieRafananNo ratings yet
- Case Presentation OsteomylitisDocument64 pagesCase Presentation OsteomylitisDemi Rose Bolivar100% (1)
- Liver Function Test FinalDocument98 pagesLiver Function Test FinalHussain AzharNo ratings yet
- Blood Transfusion Reactions: Dr. Madhuvan GuptaDocument42 pagesBlood Transfusion Reactions: Dr. Madhuvan GuptaDr. Madhuvan GuptaNo ratings yet
- Atun Maricris Jorre Ca2 Au Legarda Leadership Managemet Research DownloadableDocument2 pagesAtun Maricris Jorre Ca2 Au Legarda Leadership Managemet Research DownloadableCharissa Magistrado De LeonNo ratings yet
- Blood TransfusionDocument18 pagesBlood TransfusionJeeduu frostNo ratings yet
- Asthma2 Case StudyDocument8 pagesAsthma2 Case StudyGlenn Asuncion PagaduanNo ratings yet
- ICU Burns GuidelineDocument24 pagesICU Burns GuidelineJonas BlaineNo ratings yet
- GBS Nursing MangementDocument21 pagesGBS Nursing MangementJoseph Namita SunnyNo ratings yet
- Assisting A Patient With Ambulation Using A Walker: Page 1/2Document2 pagesAssisting A Patient With Ambulation Using A Walker: Page 1/2Mac Cristian A. CaraganNo ratings yet
- Who Par To GraphDocument59 pagesWho Par To GraphHandri Rezki VebrianNo ratings yet
- Ca CHN Copar ReviewDocument23 pagesCa CHN Copar Reviewapril punzalanNo ratings yet
- Chronic GastritisDocument7 pagesChronic GastritisDivina AquinoNo ratings yet
- Hemolytic Disease of NewbornDocument15 pagesHemolytic Disease of Newborncyphochilus100% (1)
- Blood TransfusionDocument55 pagesBlood Transfusionanand7504100% (2)
- Frontal Lobes Parietal Lobes (Basic Brain Anatomy Here)Document6 pagesFrontal Lobes Parietal Lobes (Basic Brain Anatomy Here)ejkohNo ratings yet
- Case Hernia2Document19 pagesCase Hernia2ejkohNo ratings yet
- Need To Know: Isolated Systolic Hypertension: AnemiaDocument8 pagesNeed To Know: Isolated Systolic Hypertension: Anemiaemlyn_lanonNo ratings yet
- C C C ! "##$%& ' $#+ ,-C " % .# .# " / 1 !% ! 23 "% 23 ! C % !Document4 pagesC C C ! "##$%& ' $#+ ,-C " % .# .# " / 1 !% ! 23 "% 23 ! C % !ejkohNo ratings yet
- Blood ConversationDocument300 pagesBlood ConversationMohsin NabeelNo ratings yet
- Blood TransfusionDocument35 pagesBlood TransfusionMarvin Dela Cruz100% (1)
- ABO Blood Group Harmening PDFDocument30 pagesABO Blood Group Harmening PDFKathe Deanielle Dayon100% (1)
- Educationandadministration: Development of A Validated Exam To Assess Physician Transfusion Medicine KnowledgeDocument6 pagesEducationandadministration: Development of A Validated Exam To Assess Physician Transfusion Medicine KnowledgeFOURAT OUERGHEMMI100% (1)
- Reaksi Transfusi, TRALI Vs TACODocument12 pagesReaksi Transfusi, TRALI Vs TACOifadhrohayatNo ratings yet
- PathologyDocument36 pagesPathologySayeed KhanNo ratings yet
- ARDS Meduri JAMA 1998Document8 pagesARDS Meduri JAMA 1998Rivaneide AmorimNo ratings yet
- Noncardiogenic Pulmonary Edema - UpToDateDocument17 pagesNoncardiogenic Pulmonary Edema - UpToDateStefani AtlleNo ratings yet
- Transfusion ReactionsDocument36 pagesTransfusion Reactionsmarky203No ratings yet
- Prevention of Adverse ReactionsDocument15 pagesPrevention of Adverse Reactionscupuwatie cahyaniNo ratings yet
- Complication of Blood TransfusionDocument89 pagesComplication of Blood TransfusionyohannesNo ratings yet
- Pre Exam Surgical Notes 2Document166 pagesPre Exam Surgical Notes 2flor vickyNo ratings yet
- DR Zalina - Trafusion Reaction and Management PDFDocument77 pagesDR Zalina - Trafusion Reaction and Management PDFvasu_5iveNo ratings yet
- Complications of Blood TransfusionDocument10 pagesComplications of Blood Transfusionpinkcherub4No ratings yet
- Blood Transfusion Reactions: Dr. Madhuvan GuptaDocument42 pagesBlood Transfusion Reactions: Dr. Madhuvan GuptaDr. Madhuvan GuptaNo ratings yet
- How Should We Use Convalescent Plasma Therapies For The Management of COVID-19?Document9 pagesHow Should We Use Convalescent Plasma Therapies For The Management of COVID-19?Asep tepiyanaNo ratings yet
- Pocketbookofobstetricneonatalnpediatricemergencies PDFDocument378 pagesPocketbookofobstetricneonatalnpediatricemergencies PDFDANANo ratings yet
- Surgery 5 - Answers v1 (Wide)Document56 pagesSurgery 5 - Answers v1 (Wide)Humzala BashamNo ratings yet
- Blood Transfusion ReactionsDocument33 pagesBlood Transfusion Reactionsmarianne.bilaoen09No ratings yet
- Republic Act 7719Document10 pagesRepublic Act 7719Jenny-Ann Baliday100% (1)
- Blood Transfusion Guidelines 2014Document10 pagesBlood Transfusion Guidelines 2014Trang HuynhNo ratings yet
- Hematology NotesDocument32 pagesHematology NotesbrittaNo ratings yet
- Hemovigilancia ISBT 2011Document12 pagesHemovigilancia ISBT 2011Leonardo Borges dos SantosNo ratings yet
- Blood Components: Red CellsDocument4 pagesBlood Components: Red CellsKyle Ambis SyNo ratings yet
- Fluido y ElectrolitosDocument9 pagesFluido y ElectrolitosHen RyNo ratings yet
- Clinical Guidelines For The Use of Granulocyte TransfusionsDocument13 pagesClinical Guidelines For The Use of Granulocyte Transfusionssm19790% (1)
- Acute Respiratory Distress SyndromeDocument14 pagesAcute Respiratory Distress SyndromeAila BarbaNo ratings yet
- Blood Conservation Techniques in Obstetrics: A UK PerspectiveDocument9 pagesBlood Conservation Techniques in Obstetrics: A UK PerspectiveRizky FadhilahNo ratings yet
- Final Blood 2015 Last Edite 1Document184 pagesFinal Blood 2015 Last Edite 1aliNo ratings yet
- Surgery Slide 6 - Blood TransfusionsDocument54 pagesSurgery Slide 6 - Blood TransfusionsEman NazzalNo ratings yet
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthFrom EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthRating: 4 out of 5 stars4/5 (6)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 4.5 out of 5 stars4.5/5 (3)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonFrom EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonRating: 3.5 out of 5 stars3.5/5 (33)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeFrom EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeRating: 4 out of 5 stars4/5 (3)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodFrom EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodNo ratings yet
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarFrom EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarRating: 5 out of 5 stars5/5 (351)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainFrom EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainRating: 3.5 out of 5 stars3.5/5 (38)
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeFrom EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeRating: 4 out of 5 stars4/5 (3)
- The End of Craving: Recovering the Lost Wisdom of Eating WellFrom EverandThe End of Craving: Recovering the Lost Wisdom of Eating WellRating: 4.5 out of 5 stars4.5/5 (82)
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (1)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)From EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Rating: 4 out of 5 stars4/5 (411)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingFrom EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingRating: 4 out of 5 stars4/5 (3)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyFrom EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNo ratings yet
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- Keto Friendly Recipes: Easy Keto For Busy PeopleFrom EverandKeto Friendly Recipes: Easy Keto For Busy PeopleRating: 3.5 out of 5 stars3.5/5 (2)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)
- The Complete Beck Diet for Life: The 5-Stage Program for Permanent Weight LossFrom EverandThe Complete Beck Diet for Life: The 5-Stage Program for Permanent Weight LossRating: 3.5 out of 5 stars3.5/5 (6)
- How Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseFrom EverandHow Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseRating: 4.5 out of 5 stars4.5/5 (84)
- Molecules of Emotion: Why You Feel the Way You FeelFrom EverandMolecules of Emotion: Why You Feel the Way You FeelRating: 4 out of 5 stars4/5 (128)